Article Text

Abstract
The pharmacist may play a relevant role in primary and secondary prevention of cardiovascular diseases, mainly through patient education and counselling, drug safety management, medication review, monitoring and reconciliation, detection and control of specific cardiovascular risk factors (eg, blood pressure, blood glucose, serum lipids) and clinical outcomes. Systematic reviews of randomised controlled and observational studies have documented an improved control of hypertension, dyslipidaemia or diabetes, smoking cessation and reduced hospitalisation in patients with heart failure, following a pharmacist’s intervention. Limited proof for effectiveness is available for humanistic (patient satisfaction, adherence and knowledge) and economic outcomes. A multidisciplinary approach, including medical input plus a pharmacist, specialist nurse or both, and a greater involvement of community rather than hospital pharmacists, seems to represent the most efficient and modern healthcare delivery model. However, further well-designed research is demanded in order to quantitatively and qualitatively evaluate the impact of pharmacist’s interventions on cardiovascular disease and to identify specific areas of impact of collaborative practice. Such research should particularly focus on the demonstration of a sensitivity to community pharmacist’s intervention. Since pharmacy services are easily accessible and widely distributed in the community setting, a maximum benefit should be expected from interventions provided in this context.
- hypertension
- coronary artery disease
- heart failure
- pharmacist
- diabetes
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
The relationship between decreasing cardiovascular disease risk factors and the improvement in cardiovascular disease outcomes is well established, and current guidelines recommend an aggressive reduction in these risks in order to prevent major cardiovascular accidents.1 The pharmacist may play a relevant role in primary and secondary prevention of cardiovascular diseases. In addition to medication dispensing, the pharmacist can provide more direct interventions (eg, medication education and disease management), as a support to the physician’s action, in order to improve medication adherence, to achieve the goals of desired therapeutic outcomes and to improve safe medication use and humanistic control.2 The direct pharmacist’s intervention in patients’ care, in alternative to conventional approach, has proved to favourably affect therapeutic and safety outcomes in different diseases or conditions including diabetes, dyslipidaemia, arterial hypertension, obesity, asthma or chronic obstructive pulmonary disease, infective diseases (including influenza immunisation), psychiatric conditions and osteoporosis prevention.3–5 A recent overview of systematic reviews has documented a positive impact on patients’ outcomes (blood pressure and haemoglobin A1c reduction) of clinical pharmacy services targeting specific cardiovascular conditions, such as hypertension or diabetes mellitus.6 Effects on humanistic outcomes such as patient adherence, patient satisfaction, patient knowledge and quality of life were variable and inconclusive across the various studies.
Given these premises, in the present review, we aim to update the reader on the current services that the pharmacist may provide in order to help manage the patients with cardiovascular disease or individuals at risk of cardiovascular disease. We will also discuss the actual benefits of such interventions at the light of the current evidence from randomised or observational studies and the perspectives and potentials for the development of appropriate healthcare delivery models. The primary focus of this review will be the discussion of current evidence on the benefit provided by models based on a multidisciplinary approach, which is the most popular and best accepted by the medical community worldwide.
Given the large amount of available studies, with different levels of quality, and the heterogeneity of settings (hospital, outpatient clinic and community) and outcomes, we opted for showing results from large and well-conducted meta-analyses published in the literature in recent years.
Pharmacy services for patients with cardiovascular disease
Pharmacy services provided to patients with cardiovascular disease may be roughly classified into three groups: activities directed at patients, activities directed at healthcare professionals and those provided within the frame of a multidisciplinary teamwork.7 8 A simplified list of most common services is provided in box 1.
Pharmacy services for cardiovascular prevention and management
Educational activities directed at patients
Patient education and counselling
Drug safety management
Informative activities directed at healthcare professionals
Documenting adverse drug reactions occurring to the patients
Monitoring patient’s adherence to physician’s prescription
Direct intervention in a multidisciplinary team
Collaborative medication management (including drug administration)
Medication review and dose adjustment or titration
Medication monitoring and reconciliation
Definition and application of disease management pathways and protocols
Detection, prevention or control of specific cardiovascular risk factors
Monitoring patients’ outcomes
Posthospital discharge follow-up and home visits for critical patients
Patient education and counselling about medication, diseases and non-pharmacological treatment (including indication on appropriate lifestyle) are traditional pharmacist’s activities. These services are aimed at improving patient knowledge and at promoting the correct use of medicines, favouring the adherence to treatment and preserving a healthy status. The pharmacist also needs to assess possible issues related to drug safety in treated patients, providing specific advises and documenting such occurrences to the physician in charge of the patient. However, the most interesting and potentially successful and useful activities which a pharmacist may accomplish are those involving a direct intervention in a multidisciplinary team: the potentiality of such an approach will be addressed and discussed in detail in the present paper. Team-based multidisciplinary services include medication review and drug therapy adjustments, in which the pharmacist has the autonomy to manage medicines according to predefined clinical protocols or collaborative agreements with the physician, and elaboration or refinement of a complete and reliable medication history and therapeutic reconciliation following hospital discharge and follow-up. Of particular interest is the development of structured programmes for detection, prevention or control of specific risk factors, including measurement of blood pressure, blood glucose and lipids, and provision of diagnostic tests with medical reporting, such as 12-lead resting ECG, 24 hour ambulatory blood pressure monitoring or 24 hour ECG Holter monitoring, through telemedicine tools, in connection with providers of medical reporting services.
In the current practice more complex interventions, such as for instance those focused on the application of clinical guidelines and dosage adjustment and titration are typically provided by hospital pharmacists, whereas community pharmacists are usually more concerned with improving patient knowledge and compliance, eventually by monitoring some patient’s outcomes. The pharmacist working within a community pharmacy is also sometimes in charge of home visits of critical or frail patients under the supervision of a primary care outpatient clinic.
Effectiveness of the pharmacist’s intervention in diverse cardiovascular conditions
In the last decade, several systematic reviews were conducted to measure the effect of indirect or direct pharmacist care of patients with cardiovascular diseases. We searched the literature for such publications, which included both randomised controlled and observational studies, performed in specific settings or pooling together interventions from different settings (community, outpatient clinic or hospital). The results of these meta-analyses are summarised in table 1 and will be discussed in detail in the next sections.
Summary of principal systematic reviews or meta-analyses assessing the impact of the pharmacist’s intervention on cardiovascular risk factors and diseases
Patients with multiple risk factors for coronary disease
One of the first published work evaluating the effectiveness of the pharmacist’s intervention to reduce risk behaviours and risk factors for coronary heart disease was limited to community pharmacy-based activities. The systematic review included 9 studies and 4091 individuals at high risk for coronary heart disease and showed a clear positive contribution of pharmacist to smoking cessation and an important role in managing lipid levels.9 However, these benefits were evident only in the few randomised controlled studies and the authors concluded that further investigations were warranted in this area. Santschi et al 10 conducted a systematic review of 30 randomised controlled studies and documented a significant reduction in blood pressure (8.1 (10.1 to 5.9) mm Hg for systolic and 3.8 (5.3 to 2.3) mm Hg for diastolic; P<0.001 for both), total cholesterol (17.4 (25.5 to 9.2) mg/L; P<0.001) and low density lipoprotein (LDL) cholesterol (13.4 (23.0 to 3.8) mg/L; P=0.006) and a reduction in the risk of smoking (relative risk: 0.77 (0.67 to 0.89); P=0.001), following pharmacist’s intervention, which in some cases included a direct care in collaboration with the physician. Tan et al 5 reviewed 17 studies based on clinical pharmacy services delivered in primary care general practice clinics. The pharmacist’s intervention, mainly involving medication review with or without other activities delivered collaboratively with the family physician, resulted in significant (P<0.05) reductions in blood pressure (5.7 (7.1 to 4.3) mm Hg for systolic and 3.5 (4.4 to 2.6) mm Hg for diastolic), haemoglobin A1c (0.9 (1.2, 0.6) %), LDL-cholesterol (18.7 (34.1 to 3.4) mg/dL), total cholesterol (32.0 (54.9 to 9.1) mg/dL) and 10-year Framingham risk score (1.8 (3.7 to 0.0) %). More recently, Brown et al 11 identified 24 relevant studies of pharmacy-delivered interventions, with most of the evidence focused on smoking cessation interventions (behavioural support and/or nicotine replacement therapy). These interventions were effective and cost-effective in helping adults to stop smoking, particularly compared with usual care (the OR was 1.85 (1.125 to 2.75), an indicator of positive effect of the intervention on 9714 participants smoking cessation). Pharmacy-based weight loss interventions appeared to be as effective as similar interventions in other primary care settings, but not as effective or cost-effective as commercially provided weight management services in community settings. In the five studies evaluating multicomponent interventions (pharmacotherapy and lifestyle changes) compared with usual care in participants with comorbidities (diabetes mellitus, dyslipidaemia and hypertension), a significant improvement in the relevant primary outcomes of glycaemic control, lipids and blood pressure could be observed. However, a quantitative meta-analysis could not be performed because of the paucity of available studies.
In summary, in all the aforementioned meta-analyses a benefit of pharmacy services on major cardiovascular risk factors and an improvement in inappropriate lifestyles predisposing to cardiovascular disease could be demonstrated. However, a common finding of these reviews was the substantial heterogeneity among the various studies.
Hypertension
As shown in a recent systematic review of the literature which examined 520 articles published in the last 40 years, reporting 439 randomised controlled trials assessing clinical pharmacy services, the most successful results were observed when specific medical conditions such as hypertension or diabetes were considered.12
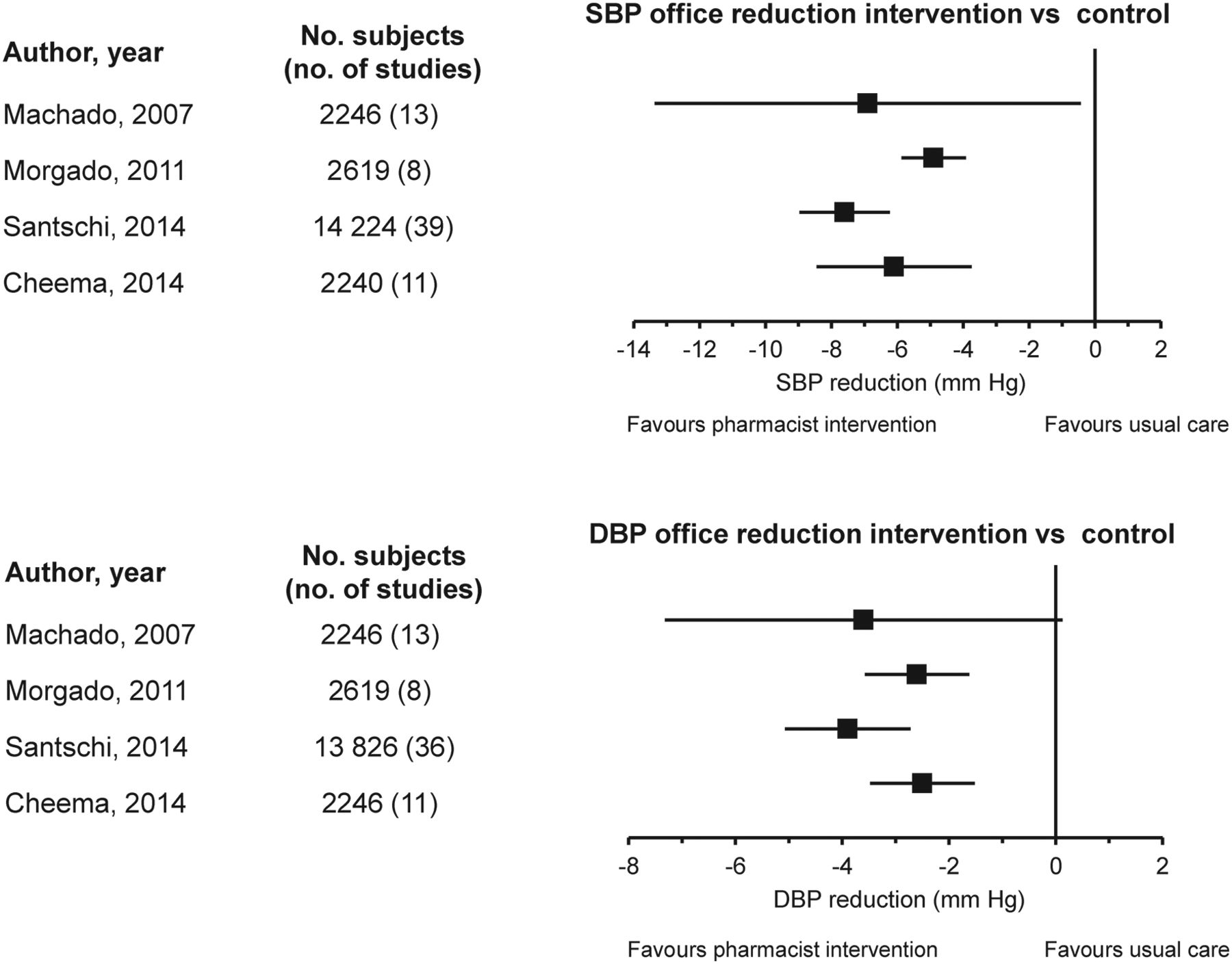
In case of hypertension, systematic reviews and meta-analyses concluded that pharmacist’s intervention, including education and blood pressure measurement, enhances blood pressure control and improves adherence to antihypertensive therapy (figure 1).
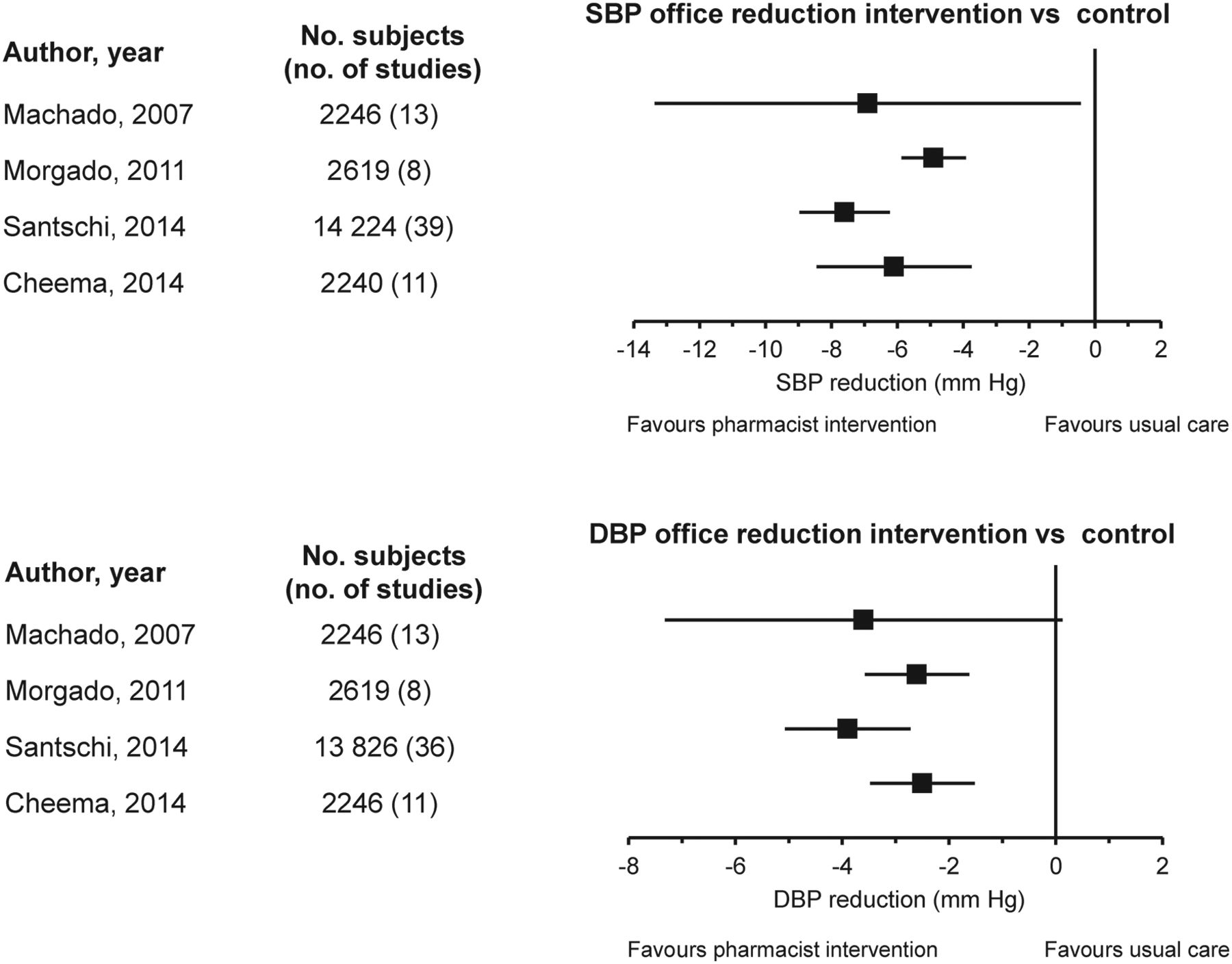
Difference in changes in SBP and DBP in patients with hypertension after the pharmacist’s intervention versus control. Data are shown as mean difference and 95% CI (redrawn from 13−16 with permission). DBP, diastolic blood pressure; SBP, systolic blood pressure.
In the meta-analysis of Machado et al,13 including 2246 patients from 13 studies, systolic blood pressure was significantly (P=0.002) reduced by 10.7±11.6 mm Hg following the pharmacist’s intervention, while it remained unchanged in the standard care group (3.2±12.1 mm Hg, P=0.361), with a further reduction in systolic blood pressure over controls following pharmacist’s intervention of 6.9±12.1 mm Hg (P=0.047). Medication management (82%) and hypertension education (68%) were the most used interventions. In this meta-analysis, pharmacist’s intervention did not have a significant influence on diastolic blood pressure, adherence to the therapy (five of three studies with significant effect) and quality of life (one of eight significant). Another meta-analysis by Morgado et al,14 including 2619 patients recruited in 8 studies, found that the pharmacist’s intervention reduced both systolic blood pressure (19.4±3.5 mm Hg) and diastolic blood pressure (8.8±2.9 mm Hg) significantly (P<0.001) more than in the control group (11.3±4.2 and 4.9±3.0 mm Hg). Also, the rate of blood pressure control was larger in the intervention group (62.8% vs 32.6% control group). Interestingly, medication adherence increased only when the intervention significantly reduced blood pressure. A more recent meta-analysis of 39 randomised controlled trials and 14 224 patients showed that the pharmacist’s intervention was associated with greater blood pressure reductions compared with usual care and that the effect tended to be larger if the intervention was led by the pharmacist (systolic and diastolic blood pressure reductions 8.5 and 4.6 mm Hg vs 6.3 and 2.8 mm Hg under collaborative care) and was done at least monthly (9.1/4.5 mm Hg vs 6.7/1.9 mm Hg less than once a month).15
Cheema et al 16 examined 16 randomised controlled trials studying 3032 patients with or without associated cardiovascular comorbidities and found that community pharmacist-led interventions were associated with significant (P<0.001) reductions in systolic blood pressure (6.1 (3.8 to 8.4) mm Hg) and diastolic blood pressure (2.5 (1.5 to 3.4) mm Hg) compared with usual care, thus contributing to improve clinical management of hypertension. A non-significant trend was observed for a smaller blood pressure reduction from community pharmacist’s interventions in patients with cardiovascular comorbidities in comparison to those without comorbidities (systolic blood pressure difference: 1.9 (–3.1 to –6.9) mm Hg and diastolic blood pressure difference: 1.5 (–0.4 to –3.4) mm Hg; P=0.460 and 0.127, respectively). Adherence was increased more often in the intervention group (OR 12.1 (4.2 to 34.6), P<0.001).
Community pharmacies may represent the ideal site for implementing community-based self-screening to detect hypertension in the population. Fleming et al 17 systematically analysed 73 studies which described screening in 9 settings, with pharmacies representing the most common setting (22% of studies) followed by public areas or retail (15%). Although authors found a high heterogeneity across studies, they were able to show an average proportion of 39% of patients with hypertension detected in community pharmacies. The rate of screened participants with raised blood pressure was larger in the pharmacy setting than in other sites and in any case the review allowed to demonstrate the usefulness of community screening of blood pressure by non-physician for detecting raised blood pressure, though they concluded that the evidence base for its effectiveness is still very poor.
Dyslipidaemia
In patients with hyperlipidaemia two meta-analyses documented significant improvements as a result of the pharmacist’s intervention on specific, but not all, patient’s health outcomes. The most notable effect was observed on total cholesterol and LDL cholesterol, although both systematic reviews reported a moderate heterogeneity. In the selected studies, most common interventions included education, followed by drug therapy recommendations and adherence assessment.
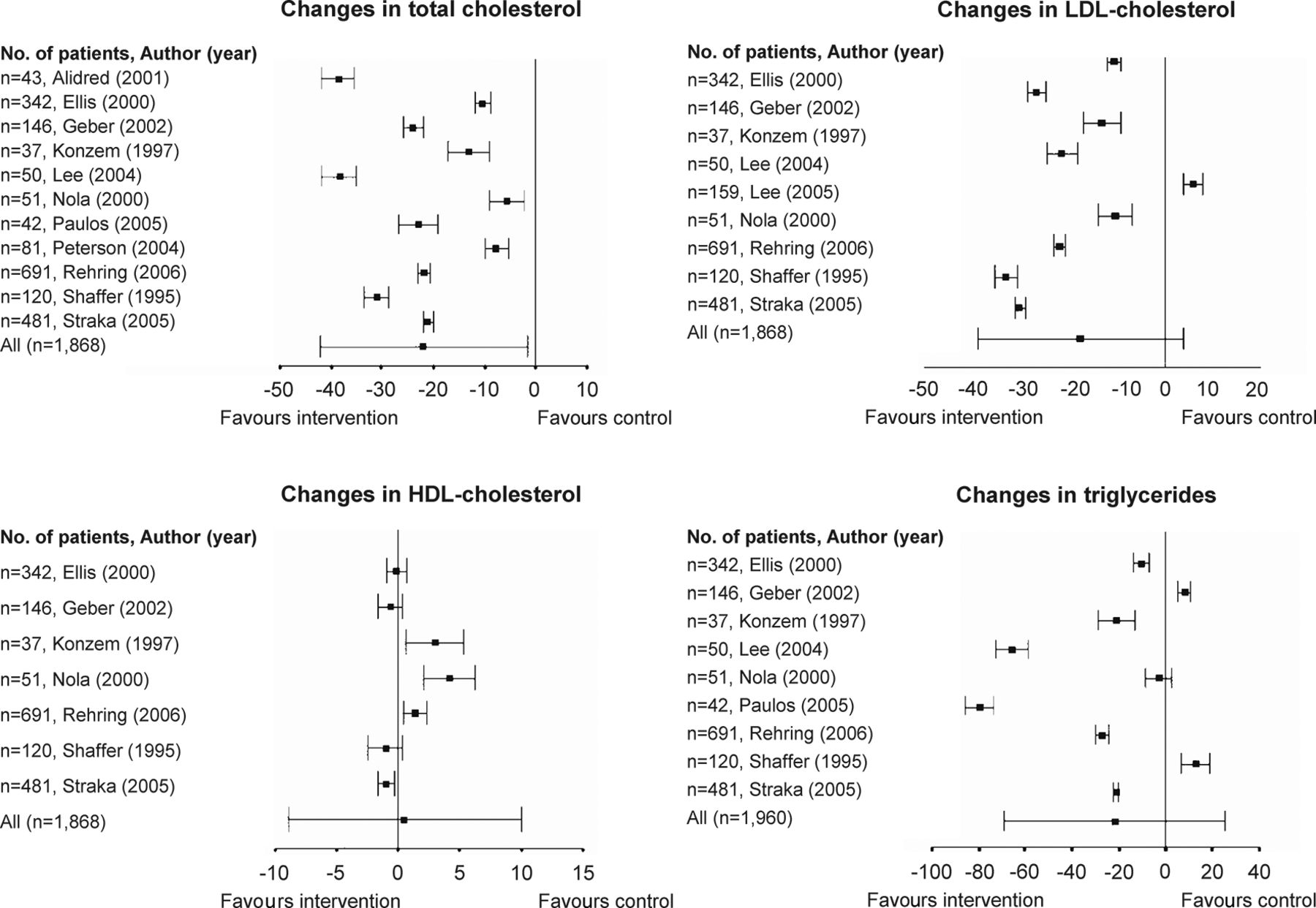
In the systematic review of Machado18 including 23 studies and 2343 patients, the pharmacist’s intervention was associated with a statistically significant (P<0.001) reduction in total cholesterol of 34.2±10.3 mg/dL, corresponding to a further significant (P=0.034) reduction of 22.0±10.4 mg/dL as compared with the control group (figure 2).
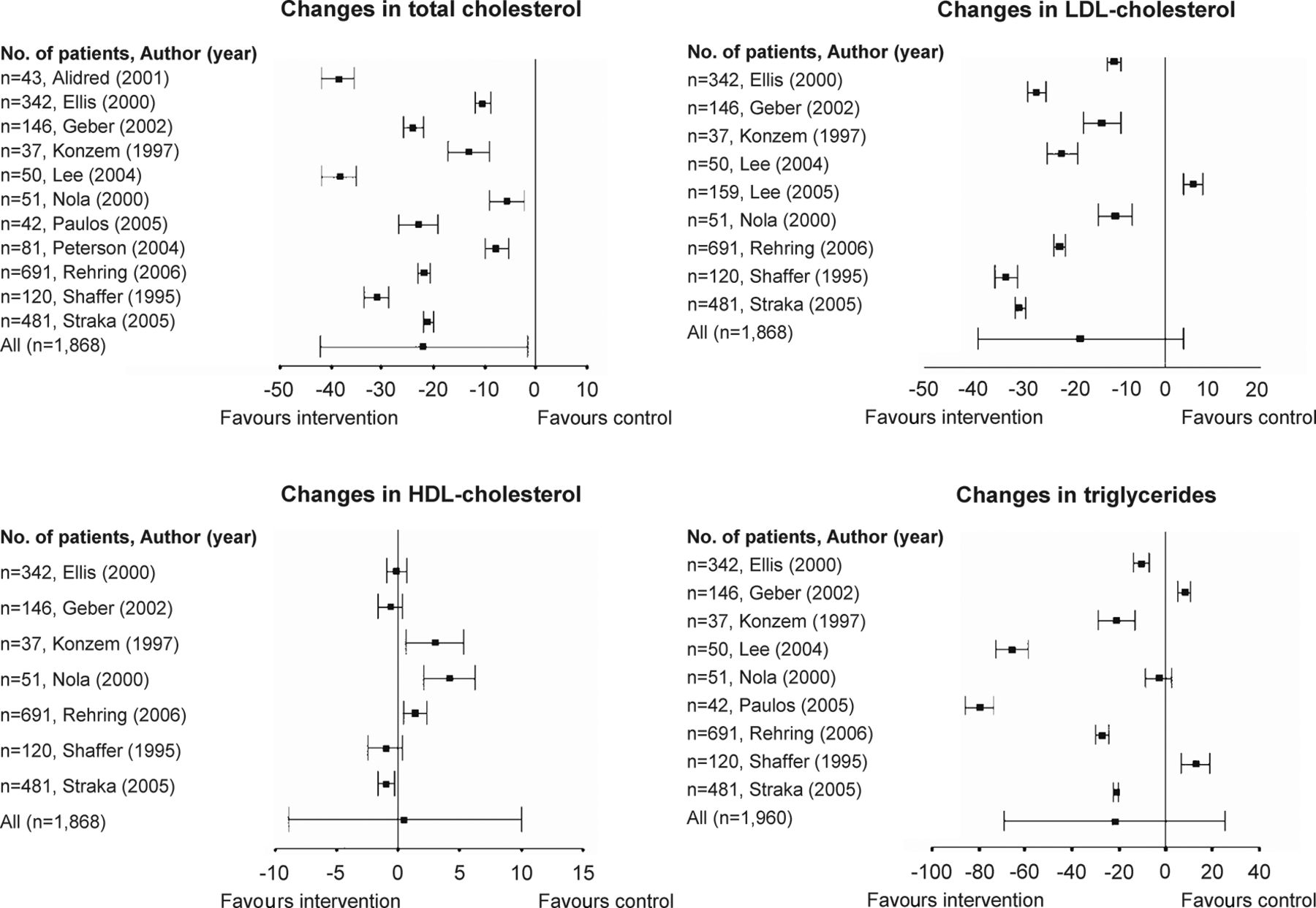
Differences in changes in total cholesterol, LDL-cholesterol, HDL-cholesterol and triglycerides (expressed as mg/dL) between patients with hyperlipidaemia receiving a pharmacist’s intervention and patients in control groups in a meta-analysis of different studies. Data are shown as mean difference and 95% CI (redrawn from 18 with permission). HDL, high density lipoprotein; LDL, low density lipoprotein.
LDL cholesterol and triglycerides levels were also reduced due to pharmacist’s intervention but the additional reduction, although clinically relevant, was not statistically significant compared with that observed in the control group (17.5±10.9 mg/dL P=0.109 for LDL cholesterol and 21.8±24.2 mg/dL P=0.368 for triglycerides) (figure 2). The pharmacist’s intervention did not impact on high density lipoprotein (HDL) cholesterol (0.5±4.8 mg/dL, P=0.910) (figure 2), patient-reported outcomes, adherence and quality of life.
Charrois and coworkers19 evaluated 21 randomised controlled trials, with 5416 patients receiving enhanced pharmacist care or standard care. In this meta-analysis at the end of the follow-up the mean LDL cholesterol level (primary outcome measure) was significantly (P<0.01) lower by 10.7 (16.9, 4.6) mg/dL in the intervention group in the 9 studies reporting this measure. Also, total cholesterol and triglycerides levels were significantly (P<0.01) lower in the enhanced pharmacist care group by 15.2 (24.0 to 6.4) mg/dL and 23.0 (37.2 to 8.9) mg/dL, respectively (10 studies). However, for all these assessments the results were highly heterogeneous. No significant effect of intervention was observed on HDL cholesterol (+0.4 (1.9 to +2.3) mg/dL). Interestingly in this meta-analysis, the primary outcome was compared between subgroups of independent practice (pharmacist directed) versus collaborative care. The latter had a 10.7 mg/dL larger effect on LDL cholesterol than independent care, though the difference did not achieve statistical significance. Finally, patients who received enhanced pharmacist care were more likely than those receiving standard care to attain target lipid levels (OR and 95% CI 2.46 (1.43 to 4.25), eight studies) to have a lipid panel ordered or recommended by a pharmacist during the study (2.02 (1.30 to 3.24), four studies) or to change their lipid-lowering therapy (1.82 (1.09 to 3.06), five studies).
Diabetes
Studies targeting adult diabetic patients documented an overall improvement in glycaemic control (haemoglobin A1c) with various pharmacist’s interventions, across diverse groups of settings and study designs. Strategies that used direct medical management by pharmacists reported the greatest benefit compared with those that used the addition of pharmacists who provided drug reviews and disease education alone.
Wubben and Vivian20 performed a qualitative meta-analysis of 21 studies (9 randomised controlled studies, 1 controlled clinical trial and 11 cohort studies) including 3981 diabetics. All interventions involved additional visits by pharmacists with expanded roles to care for adult patients with diabetes. An overall improvement in haemoglobin A1c was observed in different settings and across multiple study designs: the differences in change for haemoglobin A1c ranged from an increase of 0.2% to a decrease of 2.1%. The same authors also demonstrated that glycaemic control in patients with diabetes is much more improved in case of prescribing pharmacist. As a matter of fact, the improvement in haemoglobin A1c respect to the control group was 1.0% when the pharmacist had the authority to prescribe antidiabetic drugs under the supervision of the physician, whereas was only 0.5% without such authority (P=0.007). Two studies also conducted economic analyses which helped showing a trend to a saving in long-term costs of the disease by improving glycaemic control.
A significant (P<0.001) reduction in haemoglobin A1c (1.0%±0.3%) was observed after pharmacists’ intervention in diabetics but not in control (0.3%±0.3%) also in another meta-analysis of 30 studies, including 2247 patients.21
Diabetes education (69% of cases, consisting in verbal instructions on diet, exercise, drug therapy and disease itself) and medication dosage adjustment (61%) were the most frequently used interventions. In the same meta-analysis, no sensitive outcomes were reported for treatment adherence, changes in lipid levels, knowledge and quality of life, whereas a possible clinical benefit was documented for fasting plasma glucose and systolic blood pressure.
A more recent meta-analysis of 40 studies, of which 11 randomised controlled, failed to document any benefits to major health outcomes following community pharmacist’s intervention.22 The studies involved patient-directed interventions, such as education and follow-up, and physician-directed interventions, the most common of which was the identification of drug-related problems and provision of therapeutic recommendations. Unfortunately, studies were generally of poor quality and evaluated interventions that typically appeared to be time intensive. The interesting aspect of this review is that, at variance from previous meta-analyses, it focused on interventions specific to community pharmacists and included diabetics with additional cardiovascular risk factors or diseases.
Coronary heart disease
The contribution from pharmacists in the management of ischaemic heart disease patients has been evaluated in several studies with mixed results, allegedly because of the limited number of participants in each study and of the small number of studies available so far. While results always highlight and confirm the important role of the pharmacist for the improvement of medication adherence of these patients, the impact of pharmacist care with respect to secondary prevention of morbidity and mortality is still unclear.
Cai et al 23 provided a qualitative analysis of five randomised controlled studies including 2568 patients with coronary heart disease. The outcomes were mortality, cardiovascular events, and hospitalisations in one study (421 patients), medication adherence in five studies, blood pressure in two studies (1914 patients), and lipid management in three studies (932 patients). The interventions of pharmacists included patient education, medication management, feedback to healthcare professionals and disease management. The authors were unable to show any survival benefits or reduction in cardiac events and hospitalisations from pharmacist care. However, significant positive effects of pharmacist’s intervention could be shown on medication adherence in three studies, on blood pressure control in one study and on lipid management in one study.
Altowarijri et al 24 performed a systematic review of 59 studies conducted on patients with coronary heart disease, heart failure or with cardiovascular risk factors. The involvement of a pharmacist demonstrated an ability to improve different outcomes through provision of educational intervention, medicine management intervention or a combination of both. In particular, five of the seven randomised controlled studies assessing improvement in cardiovascular morbidity or mortality as their outcomes were able to show that clinical pharmacists have a significant effect, whereas two showed no effect. The same authors also analysed eight economic studies, demonstrating that the clinical pharmacist may have an impact in decreasing healthcare costs through improvement of cardiovascular disease risk factor control and patient outcomes.
Heart failure
Heart failure is a common and serious public health problem, whose prevalence is increasing because of ageing of the population and improved treatment of acute cardiovascular events.25 Heart failure accounts for substantial morbidity and mortality worldwide and it is the ideal target for multidisciplinary approach for achieving optimal management. Numerous studies have documented the role of the pharmacist in the care of patients with heart failure. These studies analysed services performed with varied scopes, in different settings, but mainly in the hospital, and with various outcome measures. At variance from other cardiovascular diseases and conditions, a substantive body of evidence exists on the effectiveness of the pharmacist’s intervention in terms of decrease length of stay and reduced number of hospital readmissions. Furthermore, improvement in patient wellness and overall self-perception of well-being has been observed in patients with heart failure following educational efforts implemented by the pharmacist.
A first systematic review was published by Ponniah et al 26 and evaluated the prognostic impact of pharmacy services on postdischarge patients with heart failure: in six of the seven included studies positive outcomes, such as decreases in unplanned hospital readmissions, death rates and greater compliance and medication knowledge were demonstrated. Koshman et al 27 identified 12 randomised controlled studies, showing a significant (P=0.020) association between pharmacist care and reductions in the rate of all-cause hospitalisations (OR and 95% CI 0.71 (0.54 to 0.94)) and heart failure hospitalisations (0.69 (0.51 to 0.94)) and a non-significant (P=0.270) association with the reduction in mortality (0.84 (0.61 to 1.15)). In addition, pharmacist collaborative care led to greater (P=0.020) reductions in the rate of heart failure hospitalisation (0.42 (0.24 to 0.74)) than pharmacist-directed care (0.89 (0.68 to 1.17)).
Davis et al 28 specifically assessed the impact and value of pharmacist’s interventions on adherence in patients with heart failure, demonstrating an improvement which lacked durability once the intervention ceased. The study also assessed and listed specific predictors associated with adherence to heart failure medications and concluded that pharmacist’s interventions should be part of a multidisciplinary system of care initiated at discharge and that involves personal contact and must be continued indefinitely in order to sustain the achieved benefits.
Thomas et al 29 demonstrated that interventions delivered by a hospital pharmacist who followed older patients with heart failure after discharge significantly (P<0.01) reduced the risk of unplanned hospital readmission (relative risk and 95% CI 0.75 (0.59 to 0.95)). A review of 13 major studies in the literature confirmed that pharmacist’s interventions based on medication reconciliation, patient education and collaborative medication management, may effect significant positive change in therapeutics outcomes, decrease hospitalisations and readmissions, and improve overall patient perception of self.30 Very recently, Kang et al 31 confirmed in a meta-analysis of 14 randomised controlled studies that pharmacy services in patient with heart failure and coronary heart disease significantly (P<0.05) decrease all-cause hospitalisation (OR and 95% CI 0.74 (0.58 to 0.94)), but neither all-cause mortality (1.04 (0.89 to 1.21)) nor cardiac-related hospitalisation (0.90 (0.78 to 1.03)). They also observed a significantly (P<0.05) higher prescription rate of ACE inhibitor (1.43 (1.07 to 1.91)) and beta-blocker (1.92 (1.24 to 2.96)) in the intervention group. The strength of evidence for other measures of the intervention was either insufficient or low, due to the diversity of pharmaceutical care, the heterogeneity of patient populations or clinical settings.
Limitation of current evidence
Current evidence from the systematic reviews and meta-analyses shows that there are still several methodological limitations in pharmacy practice research (box 2).
Main reasons of the current limited evidence from systematic reviews and meta-analyses on the effectiveness of pharmacist’s intervention in cardiovascular disease management
Non-homogeneous interventions (most interventions based on education, medication or disease management)
Heterogeneity of study designs (few randomised controlled trials)
Benefit of direct care not fully explored
Lack of standardisation of the intervention and of the outcome assessment
Selection bias
Mixed effects of hospital and community pharmacists
Cost effectiveness poorly explored
Heterogeneity is high across studies conducted in this area, and pharmacists’ interventions are often poorly and inconsistently described across primary studies, which limits the performance of meta-analyses. As a matter of fact, after applying sensitivity analyses, in order to remove studies of lower methodological quality, particularly the oldest studies, the strength of the evidence was blunted in most systematic reviews: only few outcomes were sensitive to pharmacists’ interventions from both clinical and statistical perspectives.
Variability in the study designs, specifically with respect to the type and complexity of pharmacist’s intervention, inclusion criteria, duration of observation and follow-up, end-points considered, adequacy of sample size, are major drawbacks of studies in this setting. No standardisation in types of education, drug management protocols and use of self-monitored data (blood pressure, blood glucose, serum lipids) to adjust drug therapy was made across the studies. Most studies were affected by an important selection bias: patients receiving the intervention had often been referred to the pharmacist, while controls were not. Thus, patients in the intervention group were likely more motivated, were interested in their care and were more willing and/or able to comply with study procedures. In most studies addressing patients with hypertension, lipid disorders or diabetes, these conditions were often simultaneously present in the same subjects, thus making it difficult to extrapolate the effectiveness of the pharmacist’s intervention on a given condition or risk factor. In most cases, the magnitude of the effect on blood pressure, blood glucose or serum lipids was modest and thus a relatively small decrease in cardiovascular effect could be expected.
Several studies lacked to focus on variables that are part of the core outcome set in clinical practice guidelines: as a matter of fact interventions using objective parameters such as blood pressure or serum glucose, to assess patients’ health status rather than end-point outcomes such as hospitalisation or mortality, were the most successful in demonstrating the positive impact of the pharmacist’s intervention. Interestingly, a higher chance of success was observed when comorbidities were present or when patients were at higher risk of cardiovascular accidents. In these cases, the strength of the pharmacist’s intervention was sufficient to achieve a clear benefit. In other conditions at lower risk, the effectiveness of the intervention varied widely across studies and was difficult to be properly estimated. Unfortunately, very few studies assessed the healthcare costs associated with pharmacist case managers. The cost-effectiveness of adding a pharmacist case manager, compared with a nurse case manager or a certified educator, thus remains unclear.
Other important limitations of many studies in this field are the lack of randomisation and control, and the high heterogeneity in study settings. Some studies were randomised and controlled, others were non-randomised and non-comparative, very few were prospective, whereas most were observational and retrospective. Some studies took place in a hospital or medical centre, others in community pharmacies. Only few studies focused on prescribing pharmacist, whereas most of them were based on interventions part of a multidisciplinary approach, sometimes involving other healthcare professionals, under the supervision of a physician. Likely, this occurred because the model based on the pharmacist’s independent prescription is rather uncommon, not always well accepted by doctors and thus available only in few countries. Some studies addressed hospitalised or hospital-discharged patients others healthy subjects or relatively low-risk patients dwelled in the community. However, though studies were performed in several types of settings, medical clinics and community pharmacies were the most common settings where pharmacy services were delivered, and a team-based collaborative approach including a physician was the most common healthcare model.
Possible benefits of pharmacist’s intervention in patients with cardiovascular disease
Because of their accessibility, pharmacists are in a distinct position to provide appropriate interaction and/or collaboration with patients and physicians to ensure successful treatment. Pharmacist involvement from screening patients right up to initiation of therapy and follow-up had proved to be essential in achieving positive outcomes in most but not all patients with cardiovascular risk factors or diseases.
Randomised controlled and observational studies have demonstrated that interventions provided by pharmacists are in general beneficial in the management of major cardiovascular risk factors such as hypertension, dyslipidaemia, diabetes or smoking cessation, and in heart failure, with a positive effect on clinical outcomes. However, pharmacist’s intervention to improve humanistic outcomes such as patient satisfaction, adherence and knowledge were found effective in some but not in all studies. A good deal of randomised controlled studies documented a positive impact of pharmacist-directed care, including measurement of cardiovascular risk factors or medication adjustments, particularly in collaboration with the managing physician, but the evidence is not conclusive. A summary of possible benefits of pharmacist’s intervention in patients at high risk of cardiovascular diseases or with established cardiovascular disease is summarised in table 2.
Level of benefit of pharmacist’s intervention on clinical, humanistic and economic outcomes in cardiovascular disease
As shown in figure 3, the benefits of pharmacist’s intervention on the patient with cardiovascular disease may be complex and interrelated.
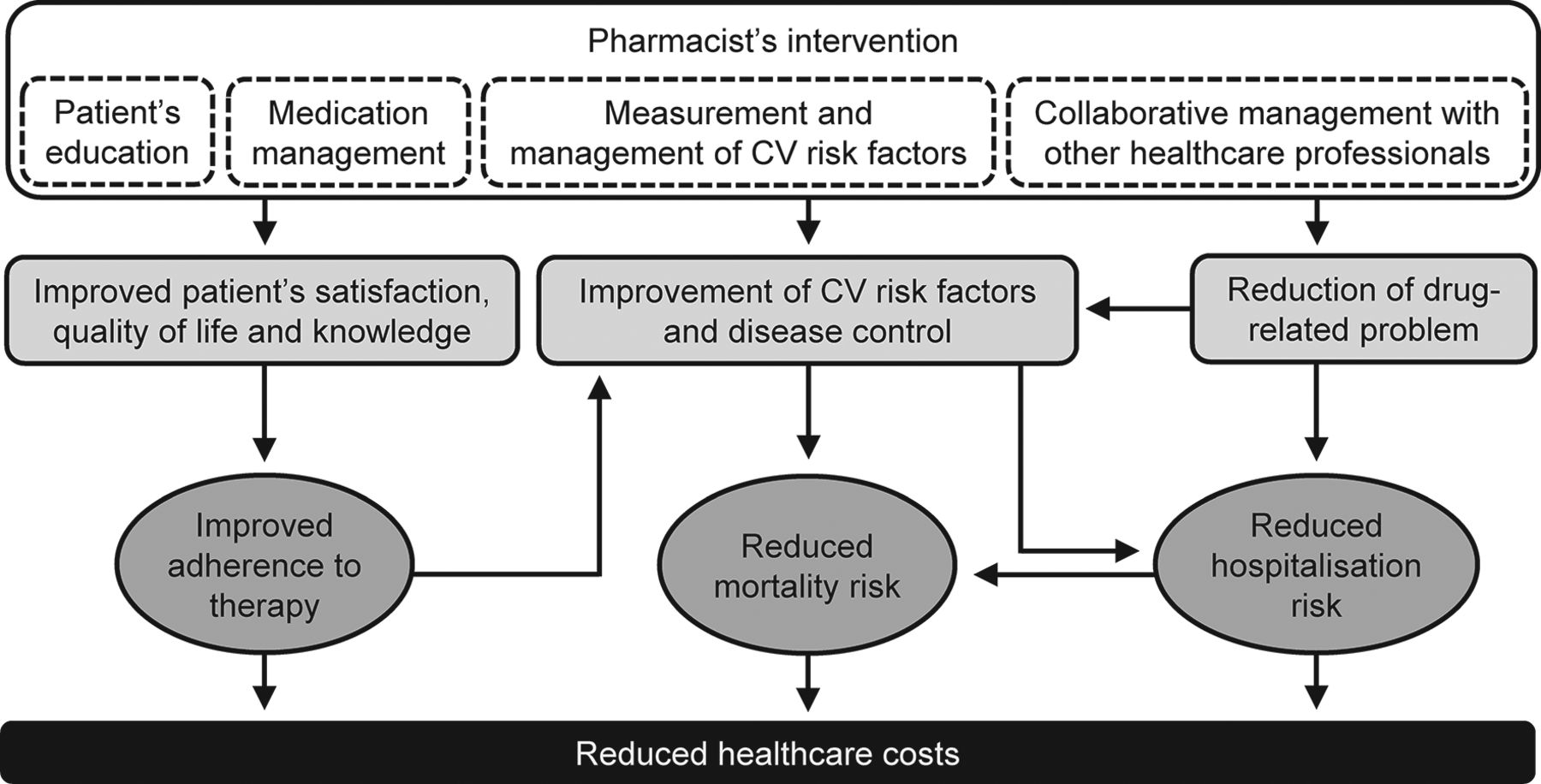
Effects of pharmacist’s intervention on humanistic, clinical and economic outcomes in patients with cardiovascular disease. CV, cardiovascular.
Patient’s education, medicine management, direct measurements and management of cardiovascular risk factors (eg, blood pressure, blood glucose or serum cholesterol) and interprofessional collaborative practice may impact on humanistic (patient’s satisfaction, quality of life and knowledge), clinical (cardiovascular risk factors and diseases, hospitalisation, adherence to treatment, adverse drug reactions and medication errors) and economic outcomes. The net effect of the pharmacist’s intervention is the use of fewer healthcare resources and cost saving, although this evidence still needs to be confirmed in large intervention trials.
Collaborative practice: the future of pharmacy practice?
In studies evaluating the effectiveness of pharmacy services, the interventions were provided independently of other healthcare professionals’ supervision or in the context of a collaborative practice with other healthcare professionals. Indeed, the multidisciplinary approach should be regarded as ideal in order to enhance patient’s outcomes, rather than unilateral interventions: this approach has been the objective of several recent studies.12 In addition to a multidisciplinary approach, more research has been recently oriented toward the primary care setting and home care, and toward a progressive involvement of community rather than hospital pharmacies.
The importance of a collaborative practice has been highlighted in a recent review:12 after the year 2000, many more studies were based on a multidisciplinary approach for early identification and follow-up of specific chronic conditions, in particular for diabetes and arterial hypertension. In recent years, the pharmacist increased the interaction with both the patients and their caregivers, mainly the referring physician, and this has turned out in a greater effectiveness of the pharmacist’s intervention. Overall, evidence demonstrates that the collaborative and patient-centred model of care is beneficial through improving control of chronic diseases, appropriate use of pharmacotherapy or promotion of health and wellness.3
In heart failure, multidisciplinary interventions which included medical input plus a pharmacist, specialist nurse, a health educator, a dietician or a social worker, reduced the risk of all cause admission by 13% (OR and 95% CI 0.87 (0.79 to 0.95); P=0.002), mortality by 21% (0.79 (0.69 to 0.92); P=0.002) and heart failure admission by 30% (0.70 (0.61 to 0.81); P<0.001), in a meta-analysis of 30 trials including 3238 patients.32 Team-based care interventions involving pharmacists were associated with improved blood pressure control compared with usual care in a meta-analysis of 37 studies.33 Interestingly, the effect was larger for studies involving community pharmacies (OR and 95% CI 2.89 (1.83 to 4.55)) than for those involving pharmacists within primary care clinics (2.17 (1.75 to 2.68)). No significant differences were observed in the effect between the studies involving pharmacists rather than nurses. This finding was strengthened in a more recent review based on 52 studies.34 A team-based care approach predominantly including pharmacists, nurses or both, collaborating with hypertensive patients and primary care providers was effective in improving blood pressure outcomes during a median follow-up of 12 months. Patients receiving team-based care were more likely to have blood pressure at target compared with usual care (+12%) and display larger systolic and diastolic blood pressure reductions during follow-up (5.4 and 1.8 mm Hg, respectively). Two interesting findings of this meta-analysis were that the extent of the improvement in blood pressure control was larger when pharmacists rather than nurses were added to the team and that no difference in the effect was observed between interventions provided in the healthcare or in the community settings. Outcomes for diabetes and lipids, other cardiovascular risk factors often comorbid with hypertension, were also analysed by Proia and coworkers. Team-based care resulted in improvement in total cholesterol (−6.3 mg/dL, +13.0% of patients at goal), LDL cholesterol (−4.3 mg/dL,+3.2%), HDL cholesterol (+1.3 mg/dL, +6% at goal), haemoglobin A1c (−0.3%, +10.0%) and blood glucose (−7.0 mg/dL).
As a matter of fact, with the increasing complexity of disease management and drug regimens for patients with cardiovascular disease, pharmacists have become a necessary part of the management team for these patients. Providing care for patients with heart failure or coronary heart disease or for those at high risk of a cardiovascular disease (eg, patients with hypertension or diabetes), with a complementary role to that of the referring physician and nurse practitioner, is a role that continues to emerge for pharmacists. They have the potential to build a strong relationship with patients and become a reliable source of information. Thanks to their enduring relationship with other healthcare providers, pharmacists can serve as a link between these healthcare providers and the patients, thus ensuring continuity of care. In addition, pharmacists may provide recommendations to the patients and their providers in order to optimise therapeutic outcomes.
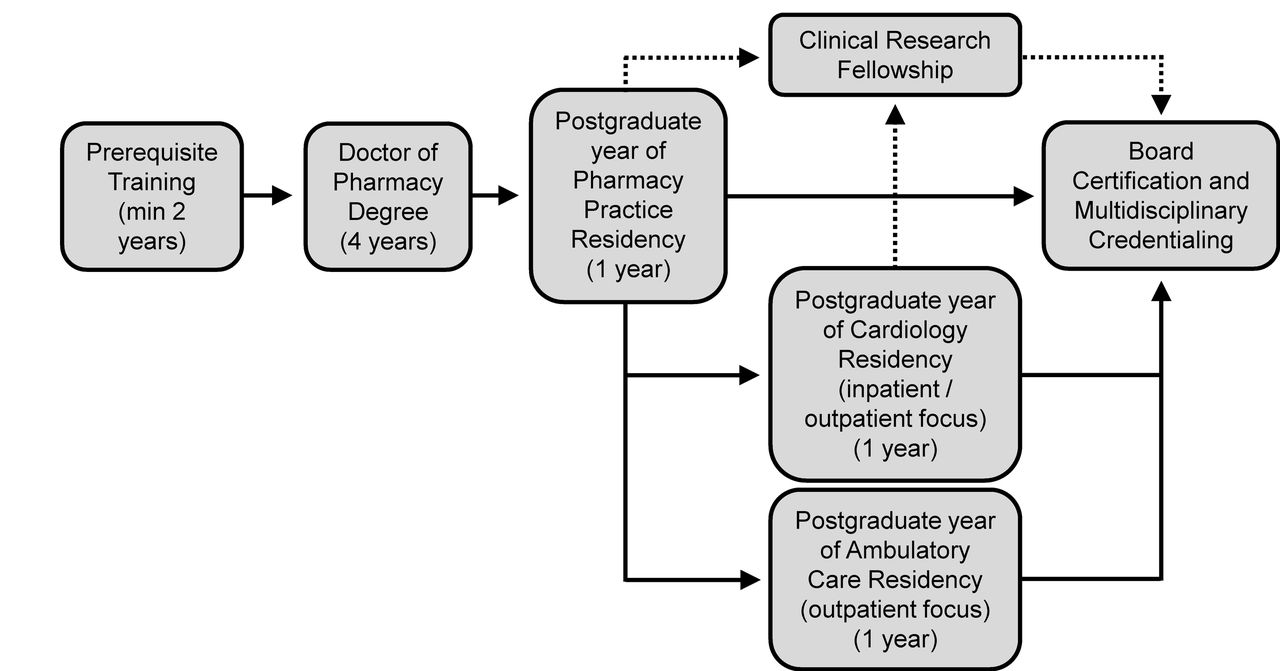
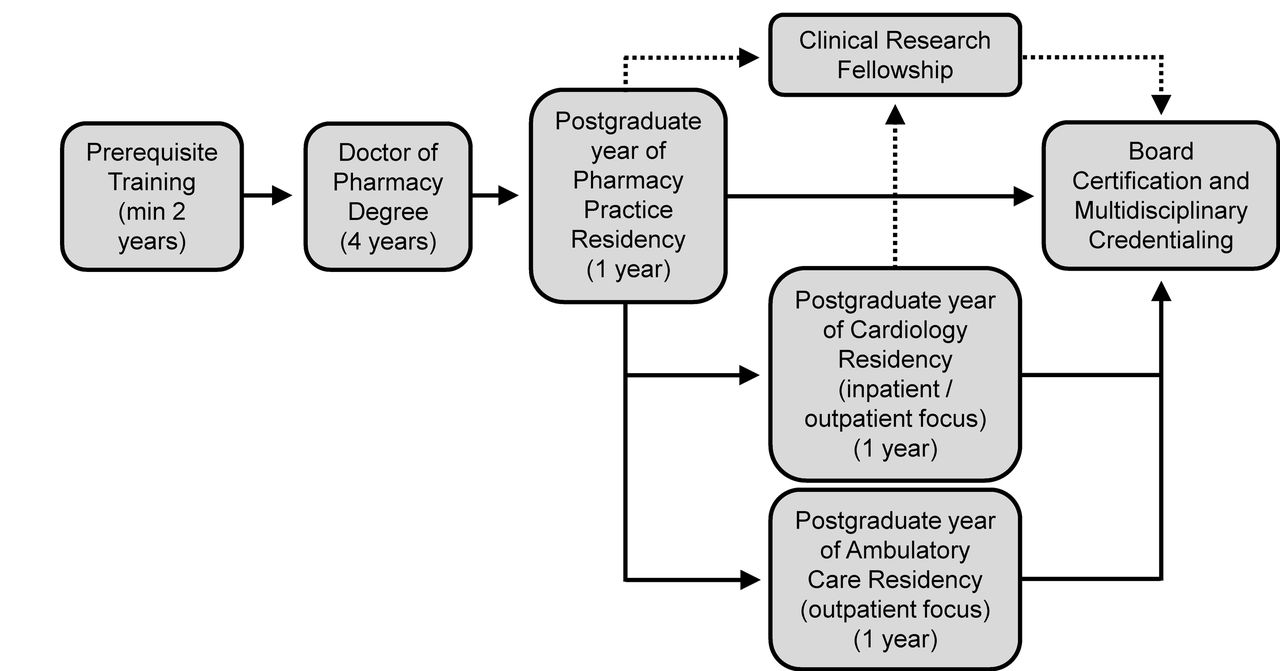
In the future pharmacists and other healthcare professionals, including nurses, may play a relevant role in a patient-centred medical home model for managing cardiovascular diseases, particularly in case of coronary heart disease and heart failure. In such a model, patients have a direct relationship with a provider who coordinates a cooperative team of healthcare professionals, including pharmacists, providing a comprehensive medication management.35 Such an approach will require an individualised care plan that achieves the intended goals of therapy with appropriate follow-up to determine actual patient outcome and will need a cooperation of several healthcare professionals, including the pharmacist. The success of the collaborative practice agreement is strongly dependent on the pharmacist’s ability, time and willingness to change his/her professional attitude. The pharmacist needs to update his/her competencies and skills on specific disease management through training and certification processes under the supervision of the physician. To this regard, the American College of Cardiology has recently published a guide to a training pathway and certification process to be followed by clinical pharmacists in the USA in order to deliver high-quality patient care within the context of a cardiology practice (figure 4).36
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Education and training route of a clinical pharmacist in a cardiology practice (redrawn from36 with permission).
According to this model, following graduation, the pharmacist has to complete a 1-year postgraduate pharmacy residency programme which is intended to produce pharmacy practitioners competent in patient-centred care and pharmacy operational services that can be applied to any practice setting (including the community pharmacy). Individuals desiring more specialised clinical training in a cardiovascular area can complete a further 1 year of residency which serves to train pharmacy practitioners in the care of patients with cardiovascular diseases. Pharmacists may obtain multidisciplinary certification covering various areas of cardiovascular disease prevention and management, such as that of certified anticoagulation care provider, certified diabetes educator or clinical lipid specialist. The residency programme may also train in the conduct of clinical research projects, the interpretation of cardiovascular biomedical published data, quality improvement initiatives, leadership and practice management, teaching and educational activities and advocacy for cardiovascular disease prevention.
Other medical Societies have published similar recommendations to guide pharmacist’s practice in collaboration with the physician. The Heart Failure Society of America and the American College of Clinical Pharmacy Cardiology Practice and Research Network have outlined guidelines for training and certification process of clinical pharmacists in a multidisciplinary heart failure team.37 The Canadian Hypertension Education Programme has published a set of guidelines on hypertension management, for pharmacists.38 The American Association of Colleges of Pharmacy published a document with recommendations on potential delivery care models with integration of pharmacists in primary care practice in the community, in the context of partnership with patients and healthcare service providers.35
Future challenges
Although in the pharmacy setting patient education and medication management are currently the most frequently used interventions, a growing request of additional services is required. These services should be focused on simple rather than complex interventions which could be affected by a number of unknown confounders and make the outcome unpredictable and only partly beneficial to the patient. Such interventions should focus on what the patient is expecting to receive from pharmacist in actual practice.
Future research should quantitatively and qualitatively evaluate the impact of pharmacists’ interventions on main chronic diseases and try to identify specific areas of impact of collaborative practice. Intervention studies should be large enough, both in sample size and length of follow-up, controlled and randomised and should evaluate different types of outcomes in the studied population and be directed toward high-risk or complex patients, because the current evidence suggest that pharmacist’s interventions are more efficacious in these patients. Community pharmacists should be preferentially involved in these studies, given the accessibility and distribution of community pharmacies and the continuous relationship of such professional figures with patients and other healthcare managers.
Finally, the progressive introduction of health information technologies and in particular of telemedicine in pharmacies and primary practices may provide new ways for patients and their healthcare team to communicate and to electronically share information on medications, life style behaviours and patient’s health status. Use of telemedicine will facilitate the screening of subjects at risk for cardiovascular diseases and provide a quick and accurate feedback and adjustments of care plans in treated patients, by promoting a more close and optimised relationship between pharmacists and doctors in a collaborative agreement practice.39
Conclusion
Some sensitivity of pharmacist’s intervention on outcomes of patients with cardiovascular disease has been shown in case of hypertension, dyslipidaemia, diabetes or smoking cessation and in heart failure. A common finding of the systematic reviews on these studies is that a greater involvement of pharmacists in activities directed to the patients and collaboration with other healthcare professionals in a team may provide an enhanced effect on various outcomes and may ultimately positively affect public health. However, the clinical importance of pharmacist’s interventions remains not fully demonstrated, and further well-designed and well-conducted studies are required in this research field. In our opinion, such studies should particularly focus on the demonstration of a possible sensitivity to community pharmacist’s intervention. Since pharmacy services are easily accessible and widely distributed in the community setting, a maximum benefit should be expected from these interventions.
References
Footnotes
Contributors SO made the search of the literature and wrote the manuscript. MC critically revised the draft manuscript before its finalisation.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.