Article Text

Abstract
Background Emerging evidence has questioned the role of high-density lipoprotein cholesterol (HDL-C) as an independent and modifiable risk factor for cardiovascular disease. We sought to understand the relationship between HDL-C levels and subsequent non-fatal clinical events.
Methods Individuals without prior cardiovascular disease or cancer were identified. Outcomes of interest were classified as non-fatal cardiovascular, cancer and infectious. Sex-stratified, multivariable, cause-specific Cox proportional hazards models were created. The reference level HDL-C for both women and men was 51–60 mg/dL.
Results Our cohort consisted of 631 762 individuals. For cardiovascular events, there was a consistent inverse relationship, with higher adjusted HRs for the lower HDL-C strata in both men and women. This relationship was also seen in the composite of non-cardiovascular outcomes. In women, the HR in the <30 mg/dL HDL-C category was 2.10 (95% CI 1.66 to 2.57) and 1.86 (95% CI 1.27 to 2.72) for cardiovascular and non-cardiovascular outcomes, respectively; in contrast, in the >90 mg/dL group, it was 0.87 (95% CI 0.74 to 1.02) and 0.81 (95% CI 0.63 to 1.06). For men, HRs were 2.02 (95% CI 1.79 to 2.28) and 1.84 (95% CI 1.47 to 2.31) in the <30 mg/dL HDL-C category for cardiovascular and non-cardiovascular outcomes, respectively, compared with 0.73 (95% CI 0.53 to 1.00) and 1.07 (95% CI 0.67 to 1.70) in the >90 mg/dL group.
Conclusions We found an inverse relationship between HDL-C and a wide spectrum of non-fatal outcomes, suggesting that HDL-C is a heavily confounded factor that may be a marker of poor overall health, rather than an independent and modifiable risk factor.
- high-density lipoprotein cholesterol
- non-fatal cardiovascular events
- non-fatal non-cardiovascular events
- competing risk models
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- high-density lipoprotein cholesterol
- non-fatal cardiovascular events
- non-fatal non-cardiovascular events
- competing risk models
Key questions
What is already known about this subject?
High-density lipoprotein cholesterol (HDL-C) levels have a heavily confounded relationship with cardiovascular disease, based on cardiovascular and non-cardiovascular mortality. Relationship between HDL-C levels and non-fatal clinical events is understudied.
What does this study add?
We observed an inverse relationship between HDL-C and wide spectrum of non-fatal outcomes was seen. These findings suggest higher HDL-C levels are a marker of poor overall health.
How might this impact on clinical practice?
This will reinforce the notion that HDL-C levels are not a target for intervention but rather a marker of health.
Introduction
There has been compelling high-quality and consistent epidemiological evidence suggesting a relationship between increased levels of high-density lipoprotein cholesterol (HDL-C) and a lower incidence of cardiovascular events such as myocardial infarction (MI) as well as cardiovascular mortality.1–11 This has laid the foundation for the hypothesis that HDL-C has a causative role in cardiovascular disease and that it is protective against atherosclerosis.12 13
The traditional view of HDL-C as an independent and modifiable cardiovascular risk factor has been challenged by emerging evidence from human genetic studies and randomised controlled trials of pharmacological agents which increase HDL-C as a therapeutic target.11 13 14 Mendelian randomised studies have found no clear association between extremely low levels of HDL-C cholesterol secondary to inherited mutations in lipoprotein metabolism and premature coronary disease.15–17 Trials of HDL-C raising drugs have, as a group, failed to show a relationship between increasing the concentrations of HDL-C cholesterol and improved cardiovascular outcomes.18–21 Moreover, HDL-C has been shown to be associated with other factors such as obesity, degree of glycaemic control, smoking, exercise and alcohol, further confounding its apparent independent relationship with cardiovascular disease.13 Previous work from our group has further reinforced this concept that HDL-C has a heavily confounded relationship with cardiovascular disease by examining the association with HDL-C cholesterol with cardiovascular and non-cardiovascular mortality.22
In addition to the previous literature examining the relationship of HDL-C with non-fatal cardiovascular disease,23 there are also data evaluating the relationship of HDL-C with incident non-cardiovascular events such as cancer24–32 or infections.33–38 However, to our knowledge, there has been no published literature evaluating the relationship of HDL-C to cardiovascular and non-cardiovascular non-fatal events in the same population. If a similar relationship of HDL-C to both cardiovascular and non-cardiovascular events was observed, this would further challenge the plausibility of HDL-C as an independent risk factor specific for cardiovascular disease and build upon our previous work which evaluated fatal outcomes. Unlike cause-specific mortality, which may be prone to misclassification, non-fatal cardiovascular versus non-cardiovascular events may be more accurate outcomes with which to understand if there is a differential association with HDL-C levels. Accordingly, to address this gap in knowledge, we made use of the Cardiovascular Health in Ambulatory Care Research Team (CANHEART) cohort, a large primary prevention ‘big data’ database in Ontario, Canada, to study the association between HDL-C and non-fatal cardiovascular and non-cardiovascular events.
Methods
Our study was conducted in the province of Ontario, which is Canada’s largest province with a population of approximately 13.6 million, all of whom received publicly funded universal medical coverage, provided by a single third-party payer, the Ontario Ministry of Health and Long-Term Care.
Data sources
The cohort was derived from the CANHEART cohort which was constructed by linking multiple individual-level databases using encoded personal identifiers.39 Databases that were linked include Canadian Institute for Health Information Discharge Abstract Database, Same Day Surgery and National Ambulatory Care Reporting System to identify inpatient hospitalisations and emergency room visits, respectively; Registered Persons Database for death information; and Gamma-Dynacare Medical Laboratories for laboratory results including lipid panel analysis. HDL-C information was gathered from the Gamma-Dynacare Medical Laboratories which captures 25%–30% of all outpatient laboratory testing in Ontario. For additional information on the 17 data sources used to create the CANHEART cohort, please see www.canheart.ca.39
Individuals who were between 40 and 105 years old on 1 January 2008 and did not have prior cardiovascular conditions and comorbidities (acute MI, coronary heart failure, stroke, percutaneous coronary intervention, coronary artery bypass grafting, cancer, dementia, peripheral vascular disease, abdominal aortic aneurysm and venous thrombus) for the previous 20 years were included in our study cohort. Individuals who were long-term nursing home residents, had invalid postal code and did not have full cholesterol panel 1 year prior to 1 January 2008 were excluded. The end of follow-up period was 31 December 2012.
Exposure and outcomes
National guidelines in Canada recommend screening lipid profiles for men over the age of 40 and women over the age of 50, to be conducted every 1–3 years.40 If the individual had multiple HDL-C measures, the measurement closest to 1 January 2008 was used as the exposure measurement. HDL-C was divided into eight categories starting at less than or equal to 30 mg/dL, in increments of 10 mg/dL, to greater than 90 mg/dL.
The primary outcome of our study was non-fatal outcomes, defined using the International Classification of Diseases, 10th revision, ascertained using the administrative databases linked as part of the CANHEART cohort. Non-fatal outcomes that were included were the most common cardiovascular and non-cardiovascular events. Cardiovascular outcomes were MI or angina, stroke, cardiac arrest and the composite of the four conditions. For non-cardiovascular outcomes, we chose those that have had previous associations with HDL-C, specifically a composite of cancers, sepsis and pneumonia. We also reported each of the cancer outcomes separately, which included all cancer, breast, prostate, lung and colorectal cancer.
Statistical analysis
We stratified the analysis by sex, given that the relevant cancers for women and men are different and we hypothesised that there may be distinct relationships of HDL-C and outcomes for each sex. We computed the age-standardised morbidity rate for each HDL-C category using the 2006 Canadian population as the reference population. Cause-specific hazard models were used to estimate the effect of HDL-C cholesterol on the rate of non-fatal outcomes.41 42 Death was treated as a competing event in these models as occurrence of death precludes from observing the non-fatal readmissions. The model was adjusted for age, quintiles of median neighbourhood income, non-HDL-C cholesterol, log of triglycerides, smoking status, and Johns Hopkins’ Aggregated Diagnosis Groups (ADG) score. Smoking status was not available in all individuals, and therefore was imputed based on other baseline characteristics. Other lifestyle factors (alcohol, body mass index, diet and physical activity) were not included due to excessive missing data. The ADG score as a measure of comorbidity burden has been shown to be an accurate prognostic factor in a general ambulatory population.43 The reference level HDL-C for both women and men was 51–60 mg/dL and all analyses were stratified by sex. Analyses were performed with the use of SAS software, V.9.3 (SAS Institute).
Results
Cohort
The details of the cohort selection are found in online supplementary appendix efigure 1. The CANHEART cohort consisted of 6 372 670 residents. Of these, 5 501 941 represented a primary prevention cohort without prior cardiovascular disease. Within the primary prevention population, 631 762 (11.4%) had a cholesterol profile performed in the 1 year prior to 1 January 2008 and were included in the analysis cohort.
Supplementary file 1
Baseline characteristics
Within the cohort, 55.4% were women, and the mean age was 57.2 years, with a mean HDL-C level of 55.2 mg/dL. The baseline characteristics for women and men, by HDL-C strata, are found in tables 1 and 2. In both sexes, mean age increased with HDL-C concentration, raising from 56.1 and 55.2 years in the <30 mg/dL group for women and men, respectively, to 58.6 and 59.6 years in the >90 mg/dL group. For income, there was an inverse relationship with HDL-C, which was most pronounced in women, where 24.6% of the <30 mg/dL group was in the lowest income quintile compared with only 12.8% of the >90 mg/dL group. There was a strong inverse relationship between the prevalence of the traditional risk factors of hypertension, diabetes and smoking and HDL-C strata, which was consistent in both sexes.
Baseline characteristics by HDL-C levels in women
Baseline characteristics by HDL-C levels in men
Cardiovascular event rates
In table 3, age-standardised event rates for each of the cardiovascular outcomes are shown for both women and men for each of the HDL-C cholesterol strata. For both sexes, there was a consistent inverse relationship, with higher events for the lower HDL-C strata. For the composite of cardiovascular events in women, there were 8.4 events/100 000 person-years in the <30 mg/dL category, compared with 2.9 events/100 000 person-years for the >90 mg/dL category. For men, the corresponding rates were 9.0 events/100 000 person-years in the <30 mg/dL category, compared with 3.2 events/100 000 person-years for the >90 mg/dL category.
Age-standardised cause-specific non-fatal cardiovascular (per 1000 persons-years) by HDL-C levels*
In figure 1, the adjusted cause-specific HRs for each of the cardiovascular non-fatal outcomes are reported. The HR for each HDL-C stratum was compared with the reference of 51–60 mg/dL for both women and men. A consistent, inverse relationship was observed for both groups with the HR increased in the lower HDL-C categories, which then plateaued in the higher HDL-C strata.
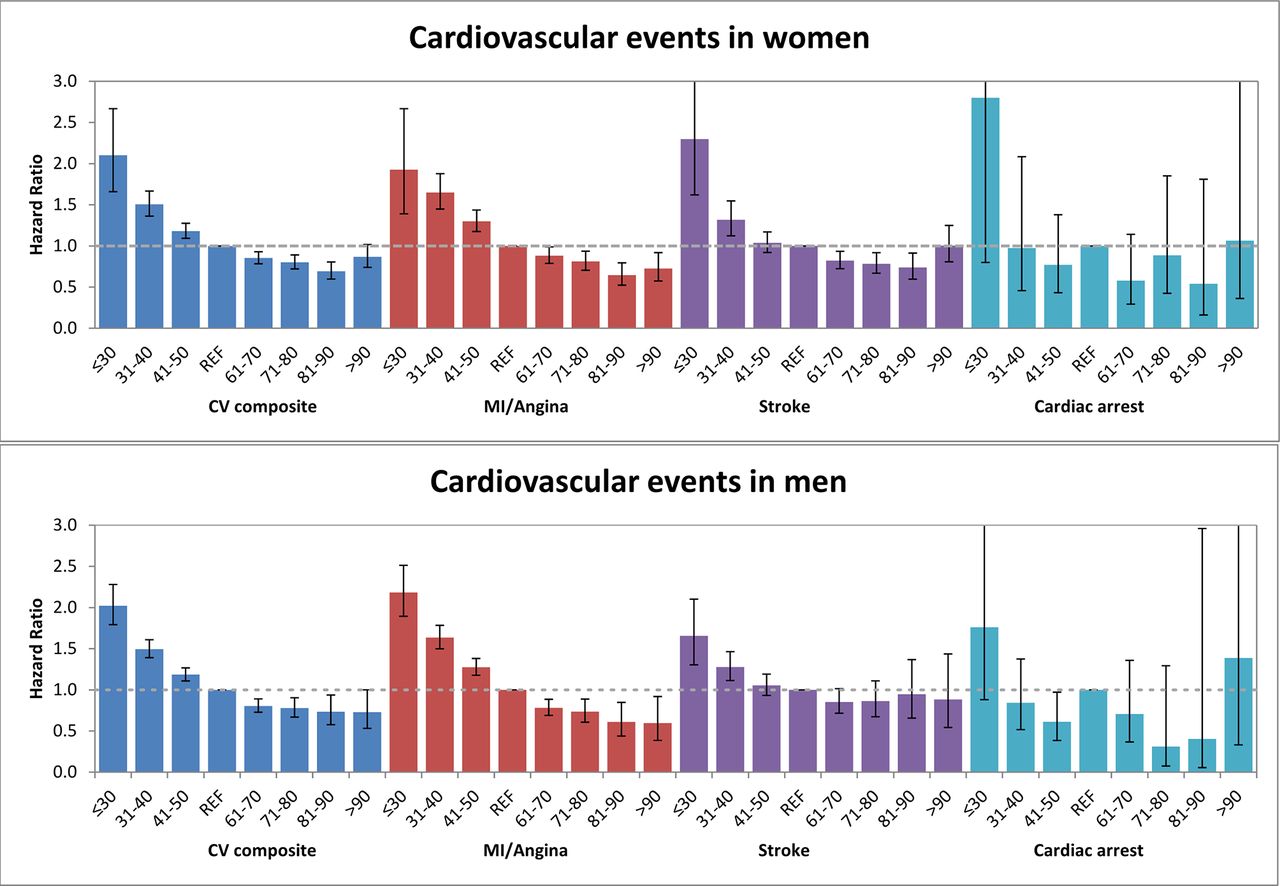
Non-fatal cardiovascular outcomes by high-density lipoprotein cholesterol (HDL-C) level. Adjusted cause-specific HRs for each outcome are reported, compared with reference category 51–60 mg/dL. CV, cardiovascular; MI, myocardial infarction.
Non-cardiovascular event rates
In table 4, in women, a similar inverse relationship was seen for the cancer and sepsis/pneumonia outcomes as was observed for the cardiovascular events. For the composite of all non-cardiovascular outcomes, the event rate was 17 events/100 000 person-years in the <30 mg/dL category, and 7.3 events/100 000 person-years in the >90 mg/dL category. However, in men, a more complex relationship was observed with cancer outcomes, where a ‘U’ shape was observed in all cancer, as well as lung and colorectal cancer with higher event rates in both the lowest and highest HDL-C categories. A similar, but less pronounced ‘U’ shape relationship was seen in the composite of all non-cardiovascular events, with an event rate of 15/100 000 person-years in the <30 mg/dL HDL-C category and 10.8/100 000 person-years in the >90 mg/dL HDL-C group.
Age-standardised cause-specific non-cardiovascular events (per 1000 persons-years) by HDL-C levels*
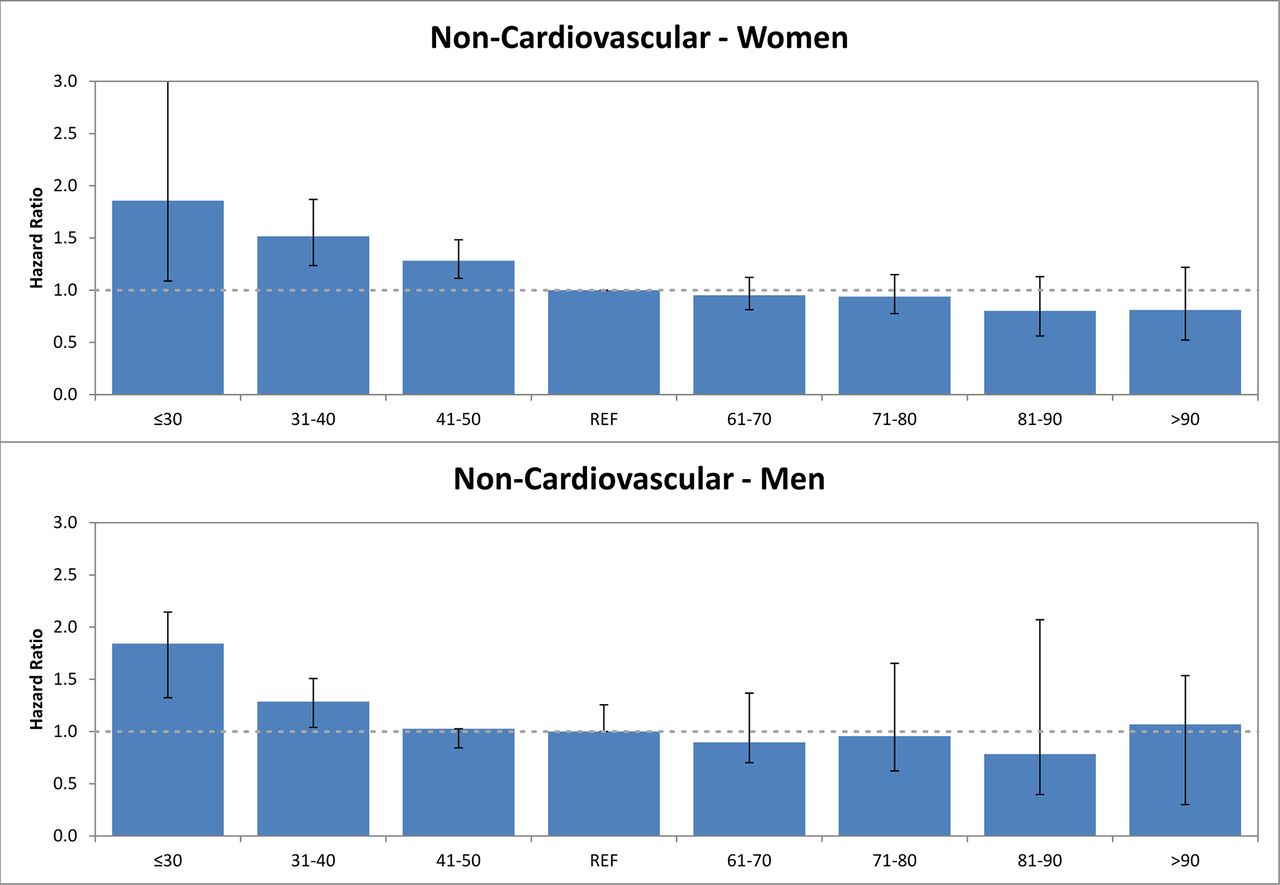
In figure 2, the adjusted HRs associated with HDL-C are shown for the non-cardiovascular events. For women, in the overall composite of non-cardiovascular events (figure 2, upper panel), the <30 mg/dL HDL-C category had an HR of 1.86 (95% CI 1.27 to 2.72), while the >90 mg/dL HDL-C category had an HR of 0.81 (95% CI 0.63 to 1.06) compared with the reference group. However, the overall inverse relationship was somewhat attenuated in cancer events in women, specifically for breast and lung cancer (online supplementary appendix efigure 2, panel a). As with the women, an attenuated but consistent relationship was seen in the composite of non-cardiovascular events for men, with a plateau in the higher HDL-C categories (figure 2, lower panel). Cancer in men (online supplementary appendix efigure 2, panel c) also had a relatively flat relationship.
{kind=link}
{kind=link}
Non-fatal non-cardiovascular outcomes by high-density lipoprotein cholesterol (HDL-C) level. Adjusted cause-specific HRs for each outcome are reported, compared with reference category 51–60 mg/dL.
Discussion
Using a large, primary prevention cohort of over 600 000 individuals, we found an inverse relationship with both cardiovascular and non-cardiovascular outcomes, reinforcing the hypothesis that HDL-C levels may be a marker of poor overall health, rather than a causative factor in either cardiovascular or non-cardiovascular disease.
Lipoprotein metabolism has been a major focus of research in cardiovascular disease for decades, and indeed the causative association of low-density lipoprotein (LDL) with atherosclerosis is irrefutable, with consistent epidemiological and randomised trial data showing that lowering LDL levels are associated with a marked reduction in cardiovascular morbidity and mortality.3 5 13 44 45 In contrast, the relationship between HDL-C cholesterol and cardiovascular outcomes has conflicted data from epidemiological studies, which have consistently suggested a strong inverse relationship, and clinical trial data which show no association between HDL-C raising and improved outcomes.
Concurrently, there have been a number of studies evaluating the relationship between lipoprotein metabolism and other outcomes, such as cancer and sepsis.24–38 The underlying physiological rationale for a possible relationship is the role that HDL-C may play in inflammation. In sepsis and infections such as pneumonia, the studies have been generally small, and the results inconsistent and inconclusive.35–38 Although a larger literature exists studying the relationship between HDL-C and various forms of cancers, these too have been mostly small cross-sectional studies or meta-analysis with inconsistent results. The largest of these was a cohort study of 23 centres evaluating colorectal cancer in 521 448 patients, which found a relatively weak inverse relationship between HDL-C levels and the incidence of proximal or distal colon cancer.31 A meta-analysis of observational trials in breast cancer by Touvier and colleagues examined 234 606 patients and found a modest but statistically significant inverse association between HDL-C levels and breast cancer, with a reduction of 14% in cancer incidence per 1 mmol/L increment in HDL-C concentration.29
Our study adds to this growing literature by studying both cardiovascular and non-cardiovascular outcomes in a single, large, primary prevention population. We found a similar dose–response relationship between HDL-C and both types of outcomes. There are a number of potential explanations for our observations. The first is that both cardiovascular and non-cardiovascular outcomes share a common pathophysiological pathway on which HDL-C acts. The diverse nature of our outcomes, ranging from prostate cancer to pneumonia, makes this explanation less likely. That said, given the observational nature of our study, we cannot discount this possibility. An alternative explanation is that HDL-C is a confounded covariate, related to multiple clinical and lifestyle factors, and indeed a low HDL-C is a marker of poor overall health, rather a cardiovascular risk factor. We hypothesise that this is the case, and may explain why interventions to increase HDL-C have not translated into improved outcomes.
Our study must be interpreted in the context of several limitations that merit discussion. First, we did not have information on HDL-C levels for the full CANHEART population, but rather only a subset of whom a lipid profile was ordered. Nevertheless, this was a large population of over 600 000 individuals. Second, we did not account for possible lipid-modifying treatments in our models. This is not feasible, as prescription information is only available for individuals over the age of 65 years in Ontario. Third, outcomes were ascertained by administrative codes which required a hospital admission, which may result in under-reporting of event rates. However, this would be consistent across HDL-C categories and should not be expected to bias our results in any particular direction. Finally, given the observational nature of our study, we cannot fully discount the potential role of HDL-C in cardiovascular disease. Specifically, HDL-C values which we evaluated have different information from HDL-C function and the latter may have different relationships with non-fatal outcome that our study cannot comment on. As such, our results should be considered hypothesis generating.
In conclusion, in a large primary prevention population of >600 000 individuals, we found an inverse relationship between HDL-C levels and both non-fatal cardiovascular and non-cardiovascular outcomes. This reinforces the hypothesis that HDL-C is a heavily confounded factor that may be a marker of poor overall health, rather than an independent and modifiable risk factor.
References
Footnotes
Contributors HCW developed the concept, interpreted the results and drafted the manuscript. MK performed the analyses, interpreted the results and provided critical revision of the manuscript. DAA, PCA, CAJ and JVT interpreted the results and provided critical revision of the manuscript. DTK developed the concept, interpreted the results and provided critical revision of the manuscript. HCW had full access to all data in the study and takes responsibility for the integrity of the data and accuracy of the data analysis.
Funding The study was supported by the Institute for Clinical Evaluative Sciences (ICES), an operating grant from the Institute of Circulatory and Respiratory Health, Canadian Institutes of Health Research (ICRH–CIHR) Chronic Diseases Team (grant no. TCA 118349), a CIHR Foundation Grant (grant no. FDN-143313), a CIHR Operating Grant (grant no. MOP-111035) and a Canadian Vascular Network (CVN) seed grant. The CVN is supported by grants from the CIHR–ICRH, and the Institute of Aging in partnership with and supported by Hypertension Canada. ICES is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care (MOHLTC). JVT is supported by a Tier 1 Canada Research Chair in Health Services Research and by an Eaton Scholar Award. HCW is supported by a Distinguished Clinical Scientist Award from the Heart and Stroke Foundation of Canada. DTK is supported by a Mid-Career Personnel Award from the Heart and Stroke Foundation, Ontario Provincial Office. PCA is supported by a Career Investigator Award from the Heart and Stroke Foundation, Ontario Provincial Office.
Disclaimer The opinions, results and conclusions reported in this paper are those of the authors and are independent of the funding sources. No endorsement by ICES or the Ontario MOHLTC is intended or should be inferred. Parts of this material are based on data and information compiled and provided by the Canadian Institute for Health Information. However, the analyses, conclusions, opinions and statements expressed herein are those of the authors, and not necessarily those of the Canadian Institute for Health Information.
Competing interests None declared.
Ethics approval The retrospective cohort study was approved by the Institutional Research Ethics Board at Sunnybrook Health Sciences Centre, Toronto, Ontario.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There are no additional unpublished data from this study.