Article Text

Abstract
Objective To assess temporal trends of in-hospital mortality in patients with acute myocardial infarction (AMI) enrolled in the Swiss nationwide registry (AMIS Plus) over the last 20 years with regard to gender, age and in-hospital treatment.
Methods All patients with AMI from 1997 to 2016 were stratified according to ST-segment elevation myocardial infarction (STEMI) or non-STEMI (NSTEMI), and gender using logistic regression analyses.
Results Among 51 725 patients, 30 398 (59%) had STEMI and 21 327 (41%) had NSTEMI; 73% were men (63.9±12.8 years) and 27% were women (71.7±12.5 years). Over 20 years, crude in-hospital STEMI mortality decreased from 9.8% to 5.5% in men and from 18.3% to 6.9% in women. In patients with NSTEMI, it decreased from 7.1% to 2.1% in men and from 11.0% to 3.6% in women. After adjustment for age, mortality decreased per additional admission year by 3% in men with STEMI (OR 0.97, 95% CI 0.96 to 0.98, P<0.001), by 5% in women with STEMI (OR 0.95, 95% CI 0.93 to 0.96, P<0.001), by 6% in men with NSTEMI (OR 0.94, 95% CI 0.93 to 0.96, P<0.001) and by 5% in women with NSTEMI (OR 0.95, 95% CI 0.93 to 0.97, P<0.001). In patients <60 years, a decrease in mortality was seen in women with STEMI (OR 0.94, 95% CI 0.90 to 0.99, P=0.025) and NSTEMI (OR 0.87, 95% CI 0.80 to 0.94, P<0.001) but not in men with STEMI (OR 1.01, 95% CI 0.98 to 1.04, P=0.46) and NSTEMI (OR 0.98, 95% CI 0.94 to 1.03, P=0.41). The mortality decrease in patients with AMI was closely associated with the increase in reperfusion therapy.
Conclusion From 1997 to 2016, in-hospital mortality of patients with AMI in Switzerland has halved and was more pronounced in women, particularly in the age category <60 years.
Trial registration number NCT01305785; Results.
- STEMI
- NSTEMI
- gender
- coronary intervention (PCI)
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Women with acute myocardial infarction (AMI) have higher in-hospital mortality. However, an overall decrease in mortality has been reported in studies using administrative databases.
What does this study add?
These contemporary clinical data reveal that the gender gap in AMI mortality has been reduced over the past two decades, particularly in young women. AMI therapy has undergone substantial changes. The mortality decrease could in large be explained by the increase in reperfusion therapy.
How might this impact on clinical practice?
These results are important for cardiovascular epidemiology and cardiologists. The trends in treatment and in-hospital mortality of patients with AMI in Switzerland are positive. Trends should be closely monitored in general to enable a timely reaction if needed, particularly for certain patient subgroups.
Introduction
Cardiovascular disease continues to be the leading cause of death in the Western world in both women and men. Administrative data showed that mortality of patients with acute myocardial infarction (AMI) considerably decreased worldwide between the 1970s and the beginning of the new millennium.1–7
The lower risk of AMI in women cannot be explained by differences in established coronary heart disease risk factors.8 However, important differences in baseline characteristics between male and female patients with AMI have been published in our previous studies.9–11 Further reports showed that younger women with acute coronary syndrome (ACS) had worse outcomes than men of the same age.7 12–15
Although women with AMI have a higher mortality than men, a prominent decline has occurred since 2000, which could be the result of the application of evidence-based therapies and education to improve awareness of heart disease in women.16 Most of the published data only cover the time period up until 2008, and knowledge on mortality trends in hospital mortality of patients with AMI in Switzerland is sparse, revealing the need for a study that includes contemporary clinical data with a long-lasting observational period.
Therefore, the aims of this study were to assess gender differences in in-hospital mortality of patients with ST-segment elevation myocardial infarction (STEMI) and non-STEMI (NSTEMI) during the last 20 years in Switzerland and to evaluate these differences in patients below 60 years of age.
Methods
The AMIS Plus registry is an ongoing nationwide prospective cohort of patients admitted with ACS to hospitals in Switzerland, founded by the Swiss Societies of Cardiology, Internal Medicine and Intensive Care Medicine in 1997. Details of the registry have been described elsewhere.17–20 Since 1997, 83 hospitals ranging from community institutions to large tertiary facilities temporarily or continuously provide, on a voluntary basis, blinded data for each patient by the treating physician or a trained study nurse through standardised internet-based or paper-based questionnaires. All data are checked for completeness, plausibility and consistency by the AMIS Plus Data Center (Epidemiology, Biostatistics and Prevention Institute, University of Zurich, Switzerland). The data centre queries treating physicians or study nurses if data are incomplete, implausible or inconsistent. Since 2010, external monitoring is regularly performed in randomly selected hospitals using randomly selected cases.
Patient selection
The present study included all patients with a definitive diagnosis of AMI defined according to the universal definitions of myocardial infarction (MI) by characteristic symptoms and/or ECG changes and/or cardiac marker elevation (either creatine kinase MB fraction at least two times the upper limit of normal or troponin I or T above individual hospital cut-off levels for MI).21 Patients included in this analysis were categorised as having STEMI or NSTEMI based on the initial ECG findings. Classification of STEMI included evidence of AMI as described above and ST segment elevation and/or new left bundle branch block (LBBB) on the initial ECG. NSTEMI included patients with ischaemic symptoms, ST segment depression or T-wave abnormalities in the absence of ST elevation on the initial ECG. All patients with a definitive diagnosis of AMI were included regardless of age, delay, inpatient onset or therapy received, and only patients with unstable angina were excluded.
Reperfusion therapy included thrombolysis or percutaneous coronary intervention (PCI). Immediate drug therapy was defined if administrated within 24 hours after presentation and was prescribed according to current practice and guideline recommendations at the time of the index presentations. The choice of intervention and medication was at the discretion of the treating physicians and hence reflects common practice in Switzerland.
Statistical analyses
The results are presented as percentages for categorical variables and were analysed using the Pearson χ2 test or Fisher’s exact test as appropriate. Continuous normally distributed variables are expressed as means±1 SD and were compared using the Student’s two-tailed unpaired t-test. Continuous non-normally distributed variables are expressed as medians and IQRs and were analysed using the Mann-Whitney U test.
Univariable and multivariable binary logistic regressions were used to analyse trends of mortality over admission years. The explanatory variables were gender, age and therapies. Admission year was included as a covariate. As the effect of age on mortality was non-linear, a quadratic dependence of age was used in multivariable regression. Model fit was assessed using the Hosmer-Lemeshow test. Adjusted ORs are reported with 95% CIs. The use of therapies changed non-linearly over time. Hence, gender differences in therapies were stratified by year of admission and analysed using the Mantel-Haenszel test. Interactions were assessed using the Breslow-Day test. A P value of less than 0.01 was considered significant. IBM SPSS Statistics software (V.23, IBM Corp. Armonk, NY, USA) was used for statistical analyses.
Results
From January 1997 to December 2016, 51 725 patients with AMI from 83 Swiss hospitals were enrolled in the AMIS Plus registry and included in this study. Among them, 30 398 (59%) had STEMI and 21 327 (41%) had NSTEMI; 73% were men (mean age 63.9±12.8 years) and 27% were women (71.7±12.5 years).
The probability of in-hospital mortality using logistic regression in patients with AMI aged 66 years according to admission year and gender is depicted in figure 1A,B.

The predicted probability of in-hospital mortality in patients with AMI aged 66 years according to admission year and gender. STEMI, ST-segment elevation myocardial infarction; NSTEMI, non-ST-segment elevation myocardial infarction.
ST-segment elevation myocardial infarction
Of the patients with STEMI, 26% were women aged 71.3±12.7 years compared with men aged 62.8±12.8 years (P<0.001). Over the study period, crude in-hospital mortality decreased from 9.8% to 5.5% in men and from 18.3% to 6.9% in women (both P<0.001) (figure 2). The quadratic model of logistic regression for mortality of patients with STEMI demonstrated a significance for non-linearity of age of P<0.001. After adjustment for gender and age, early mortality reduction was 4% per additional admission year for all patients with STEMI (OR 0.96, 95% CI 0.95 to 0.97, P<0.001). There was a weak interaction between admission year and gender (P=0.019). Age-adjusted mortality decreased in men with STEMI at a rate of 3% (OR 0.97, 95% CI 0.96 to 0.98, P<0.001) and in STEMI women at a rate of 5% per additional admission year (OR 0.95, 95% CI 0.93 to 0.96, P<0.001).

Crude in-hospital mortality of patients with STEMI according to admission year and gender from 1997 to 2016. STEMI, ST-segment elevation myocardial infarction.
Non-ST-segment elevation myocardial infarction
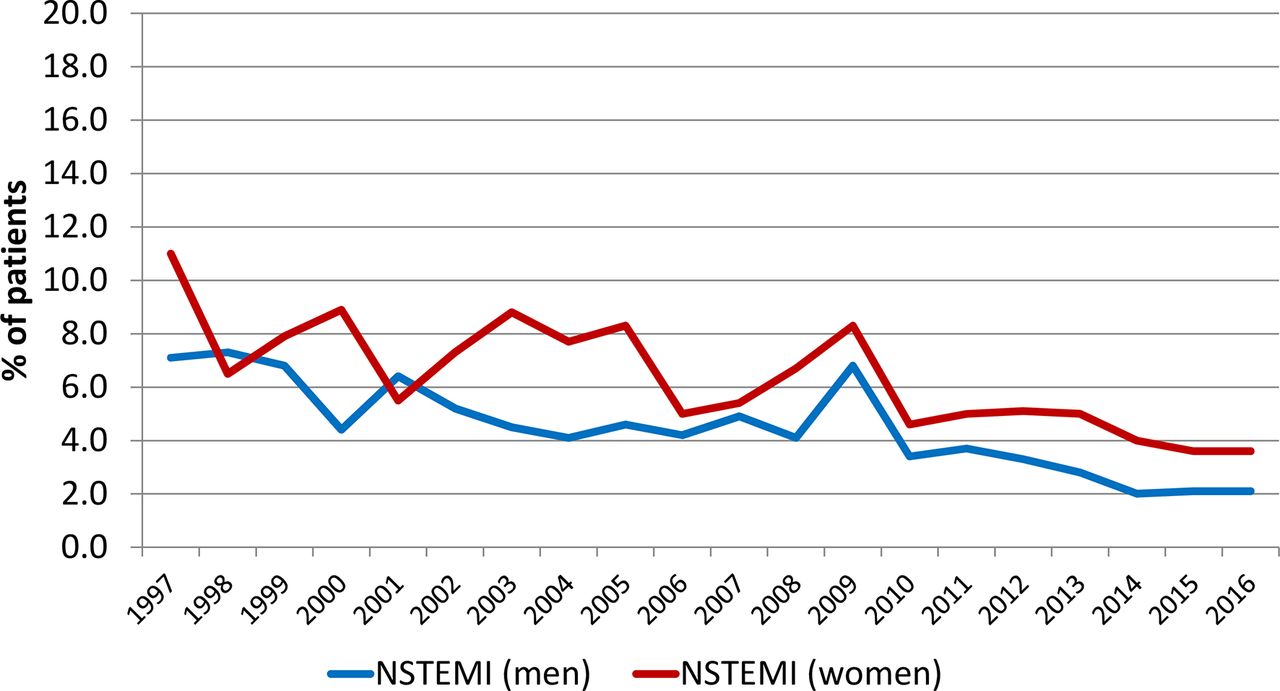
Among patients with NSTEMI, 27% were women and were older than men (72.2±12.2 years vs 65.6±12.6 years, P<0.001). From 1997 to 2016, crude in-hospital mortality decreased in men from 7.1% to 2.1% (P<0.001) and in women from 11.0% to 3.6% (P<0.001) (figure 3). The quadratic model of logistic regression for mortality of patients with NSTEMI also demonstrated a significance for non-linearity of age (P=0.001). After adjustment for gender and age, early mortality reduction was 6% for all patients with NSTEMI (OR 0.94, 95% CI 0.93 to 0.96, P<0.001) with no interaction between admission year and gender (P=0.75). The age-adjusted mortality decrease per additional admission year in patients with NSTEMI was even higher at 6% in men (OR 0.94, 95% CI 0.93 to 0.96, P<0.001) and 5% in women (OR 0.95, 95% CI 0.93 to 0.97, P<0.001).
{kind=link}
{kind=link}
{kind=link}
Crude in-hospital mortality of patients with NSTEMI according to admission year and gender from 1997 to 2016. NSTEMI, non-ST-segment elevation myocardial infarction.
Reperfusion
The use of reperfusion (thrombolysis or PCI) increased in male patients with STEMI from 60% to 93% (P<0.001) and in female patients with STEMI from 45% to 90% (P<0.001). Use of thrombolysis in patients with STEMI continuously decreased from 47% in 1997 down to 0.2% in 2016 (P<0.001), whereby the use of PCI increased from 8.3% to 91.8% (P<0.001). This increase between 1997 and 2016 was gender dependent (interaction between admission year and gender, P<0.001): in men from 9.1% to 92.5% (P<0.001) and in women from 6.0% to 89.5% (P<0.001).
The use of PCI increased in patients with NSTEMI from 3.8% to 75.8% (P<0.001). This increase between 1997 and 2016 was not gender dependent (interaction between admission year and gender, P=0.42): in men from 4.7% to 76.5% (P<0.001) and in women from 1.4% to 74.5% (P<0.001).
The mortality decrease in patients with AMI could in large be explained by the increase in reperfusion therapy: after adjustment for reperfusion use, a reduction in mortality of 1% per year remained (OR 0.99, 95% CI 0.98 to 1.00, P=0.007), whereas the gender difference disappeared (OR 0.99, 95% CI 0.90 to 1.09, P=0.85).
Drug therapies
Throughout the entire observational period, women with AMI (STEMI and NSTEMI) were overall less likely to receive guideline-recommended drugs than men with AMI. Among women, 94.0% received aspirin versus 95.6% of men (OR 0.72, 95% CI 0.66 to 0.78, P<0.001) with no evidence of OR changes for gender over time (Breslow-Day P=0.80). Overall P2Y12 inhibitors (clopidogrel, prasugrel or ticagrelor) were given to 63.8% of women compared with 72.3% of men (OR 0.61, 95% CI 0.58 to 0.65, P<0.001) with significant OR changes during the observation period (Breslow-Day P=0.009). Statins were given to 69.2% of women compared with 76.5% of men (OR 0.69, 95% CI 0.66 to 0.73, P<0.001) with no OR changes over time (Breslow-Day P=0.24). Beta blockers were given to 61.4% of female patients with AMI versus 64.6% of male patients (OR 0.86, 95% CI 0.82 to 0.90, P<0.001) with OR changes over time (Breslow-Day P<0.001) and angiotensin-converting enzyme inhibitors/angiotensin II receptor antagonists to 49.3% of women versus 50.8% of men (OR 0.95, 95% CI 0.92 to 0.98, P=0.021) without significant OR changes during the observational years (Breslow-Day P=0.021).
Younger patients with AMI
In patients aged below 60 years, a decrease in early mortality per additional admission year of STEMI was seen in women (OR 0.94, 95% CI 0.90 to 0.99, P=0.025) but not in men (OR 1.01, 95% CI 0.98 to 1.04, P=0.46) (interaction between gender and admission year P=0.019). Even greater differences were seen in patients with NSTEMI. Mortality per year dramatically decreased in NSTEMI women (OR 0.87, 95% CI 0.80 to 0.94, P<0.001) but was not significant in men (OR 0.98, 95% CI 0.94 to 1.03, P=0.41) (interaction between gender and admission year, P=0.006).
Discussion
The results of this study show that over the last 20 years, in-hospital mortality of patients with AMI in Switzerland has halved and the gender gap reduced. Although in-hospital mortality was consistently higher in women, overall age-adjusted mortality has decreased more prominently in women compared with men. In this contemporary cohort of 51 725 patients, a reduction in mortality was seen in patients with STEMI and NSTEMI of both genders. However, in patients aged below 60 years, a significant decrease in in-hospital mortality was observed in women but not in men.
The gender differences in the baseline characteristics of patients with AMI are well known and repeatedly described in the literature: women are older, have a higher burden of risk factors, have more comorbidities and are less likely to receive evidence-based therapies.16 22–25 Previously published works of ours have also shown this.9 26
However, gender differences in short-term and long-term crude mortality of patients with AMI have been described in several studies with contradictory results. Studies mainly reported on gender differences in crude mortality, but the differences no longer existed if mortality was adjusted for age, risk factors or comorbidities.12 24 27 28 Analyses of 78 254 patients from 2001 to 2006 in the ‘Get with the Guidelines’ database showed no differences in in-hospital mortality of all patients with AMI, but it was higher in women with STEMI.25 Women with ACS had worse in-hospital outcomes than men,22 and age-adjusted in-hospital mortality was higher for women.29 Analysis of temporal trends in in-hospital mortality of 916 380 patients with AMI from 1994 to 2006 in the National Registry of Myocardial Infarction showed that women experienced larger improvements than men.30 This is in line with our current results.
AMI therapy has undergone substantial changes over the 20-year period, and the use of reperfusion therapies has continually increased away from thrombolysis towards PCI, but there was a significant underuse in women.9 10 31 Although interventional strategies are equally effective in biomarker-positive men and women32 and the potential benefit on survival after 5 years appears to be similar in both genders, invasive therapy remains less frequently used in women than in men with AMI.33 In our study, PCI treatment continuously increased in both genders but was age dependent. Therefore, the age-adjusted mortality decrease in patients with AMI could in large be explained by the increase in reperfusion therapy with no differences between men and women. In a meta-analysis of 35 randomised controlled trials and observational studies of patients with STEMI who underwent PCI, the gender differences in short-term and long-term mortality remained significant even after adjustment.23 However, a study from the Mayo Clinic, which included 19 239 patients who underwent PCI from 1979 to 2004, showed a decrease in mortality during this period with no differences between men and women.34
Younger women with AMI had a higher mortality than men of similar age.7 12–15 Our study showed that the decrease in in-hospital mortality of the patients below 60 years was not significant in male patients but markedly reduced in female patients over the last 20 years. A study on young patients with AMI (30 to 54 years) from the National Inpatients Sample database showed that in-hospital mortality decreased between 2001 and 2010 in women although they had more comorbidities than young men.35 We have not seen similar differences in the Swiss population. Further studies are therefore needed in order to be able to explain these differences.
Throughout the entire observational period in our study, women were overall less likely to received guideline-recommended drugs, which is in line with other publications.36 This is in contrast to the findings of the ‘Acute Coronary Treatment and Intervention Outcomes Network Registry—Get with the Guidelines’ study of 75 370 patients with STEMI and NSTEMI enrolled from July 2008 to March 2011 where acute and discharge medical therapies were similar by race in any gender category.37 In patients with NSTEMI, gender-based differences in adverse outcomes persisted even with an increased rate of early invasive therapy.38 As the strategy of an early invasive approach for women with NSTEMI was considered controversial in the 2000s, we decided against analysing this particular point.
Limitations of the study
The limitations of the study are those common to all observational studies, particularly long-lasting studies over decades. The diagnosis of AMI has been repeatedly updated during the last 20 years, and the introduction of new biomarkers has resulted in more patients being diagnosed with AMI, particularly patients with NSTEMI, which is a non-calculated bias. Furthermore, the choice of intervention and medication was at the discretion of the treating physicians or internal hospital guidelines, which could also cause an unknown bias. However, data from ‘real-life’ routine clinical practice, which includes patients who were polymorbid, who were late comers or who were treated palliative only, contribute to a better estimation of the overall burden of AMI.
Conclusions
From 1997 to 2016, in-hospital mortality of patients with AMI in Switzerland has halved and the gender gap was further reduced. Accordingly, the mortality reduction was more pronounced in women, especially those in the age category below 60 years. The mortality decrease could in large be explained by the increase in the use of reperfusion therapy, in particular PCI, whereby the gender difference disappeared.
Acknowledgments
We would like to thank Jenny Piket for proof reading this manuscript.
References
Footnotes
Contributors DR: conception and design, analysis and interpretation of data, drafting of the article. BS: analysis and interpretation of data, critical revision of manuscript and final approval of the manuscript. MR, PU, HR and GP: acquisition of data, critical revision of manuscript for intellectual content and final approval of the manuscript. PE: acquisition of data, conception and design, critical revision of manuscript for intellectual content and final approval of the manuscript.
Funding The AMIS Plus registry is funded by unrestricted grants from the Swiss Heart Foundation and from Abbot AG, Amgen AG, AstraZeneca AG, Bayer (Schweiz) AG, B. Braun Medical AG, Biotronik AG, Boston Scientific AG, Cordis-Cardinal Health, Daiichi-Sankyo/Eli Lilly AG, GE Healthcare, Medtronic AG, A Menarini AG, Mepha Pharma AG, Merck Sharp & Dohme-Chibret AG, Novartis Pharma Schweiz AG, Pfizer AG, Servier (Suisse) AG, St. Jude Medical and Vascular Medical AG, all in Switzerland.
Disclaimer The sponsors did not play any role in the design, data collection, analysis or interpretation of the registry.
Competing interests None declared.
Ethics approval Swiss Supra-Regional Ethics Committee for Clinical Studies, the Swiss Board for Data Security and the Cantonal Ethics Commissions.
Provenance and peer review Not commissioned; internally peer reviewed.
Data sharing statement According to the AMIS Plus regulations, there are access restrictions to the individual data used as these are the property of the hospitals participating in the AMIS Plus registry and may only be made available by each hospital principal investigator and the AMIS Plus Steering Committee. This also applies to any analysis files or parts thereof used in this study.
Collaborators The authors would like to express their gratitude to the teams of the following hospitals (listed in alphabetical order with the names of the local principal investigators): Aarau, Kantonsspital (P Lessing); Affoltern am Albis, Spital (F Hess); Altdorf, Kantonsspital Uri (RSimon); Altstätten, Spital (P J Hangartner); Baden, Kantonsspital (UHufschmid); Basel, St. Claraspital (B Hornig/L Altwegg); Basel, Universitätsspital (R Jeger); Bern, Beau-Site Klinik (S Trummler); Bern, Inselspital (S Windecker, T Pilgrim); Bern, HirslandenSalem-Spital (T Rueff); Bern, Tiefenauspital (P Loretan); Biel, Spitalzentrum (C Roethlisberger); Brig-Glis, Oberwalliser Kreisspital (D Evéquoz); Bülach, Spital (G Mang); Burgdorf, RegionalspitalEmmental (D Ryser); Chur, Rätisches Kantons- und Regionalspital (PMüller); Chur, Kreuzspital (R Jecker); Davos, Spital (W Kistler); Dornach, Spital (T Hongler); Einsiedeln, Regionalspital (S Stäuble); Flawil, Spital (G Freiwald); Frauenfeld Kantonsspital (HP Schmid); Fribourg, Hôpital cantonal (JC Stauffer/S Cook); Frutigen, Spital (KBietenhard); Genève, Hôpitaux universitaires (M Roffi); Glarus, Kantonsspital (W. Wojtyna); Grenchen, Spital (R.Schönenberger); Grosshöchstetten, Bezirksspital (C Simonin); Heiden, KantonalesSpital (R Waldburger); Herisau, Kantonales Spital (M Schmidli); Horgen, See Spital (B Federspiel); Interlaken, Spital (EM Weiss); Jegenstorf, Spital (H Marty); Kreuzlingen, Herzzentrum Bodensee (KWeber); La Chaux-de-Fonds, Hôpital (H Zender); Lachen, Regionalspital (I Poepping); Langnau im Emmental, Regionalspital (AHugi); Laufenburg, Gesundheitszentrum Fricktal (E Koltai); Lausanne, Centre Hospitalier Universitaire Vaudois (JF Iglesias); Lugano, Cardiocentro Ticino (G Pedrazzini); Luzern, Luzerner Kantonsspital (PErne, F. Cuculi); Luzern Klinik St. Anna (P Erne); Männedorf,Kreisspital (T Heimes); Martigny, Hôpital régional (B Jordan); Mendrisio, Ospedale regionale (A Pagnamenta); Meyrin, Hôpital de laTour (P Urban); Monthey, Hôpital du Chablais (P Feraud); Montreux, Hôpital de Zone (E Beretta); Moutier, Hôpital du Jura bernois (CStettler); Münsingen, Spital (F Repond); Münsterlingen,Kantonsspital (F Widmer); Muri, Kreisspital für das Freiamt (CHeimgartner); Nyon, Group. Hosp. Ouest lémanique (R Polikar); Olten,Kantonsspital (S Bassetti); Rheinfelden, Gesundheitszentrum Fricktal(HU Iselin); Rorschach, Spital (M Giger); Samedan, Spital Oberengadin(P Egger); Sarnen, Kantonsspital Obwalden (T Kaeslin); Schaffhausen,Kantonsspital (A Fischer); Schlieren, Spital Limmattal (T Herren); Schwyz, Spital (P Eichhorn); Scuol, Ospidal d’Engiadina Bassa (CNeumeier/G Flury); Sion, Hôpital du Valais (G Girod); Solothurn, Bürgerspital (R Vogel); Stans, Kantonsspital Nidwalden (B Niggli); St. Gallen, Kantonsspital (H Rickli); Sursee, Luzerner Kantonsspital (S Yoon, J Nossen); Thun, Spital (U Stoller); Thusis, Krankenhaus (UPVeragut); Uster, Spital (E Bächli); Uznach, Spital Linth (A Weber); Walenstadt, Kantonales Spital (D Schmidt/J Hellermann); Wetzikon, GZOSpital (U Eriksson); Winterthur, Kantonsspital (T Fischer); Wolhusen,Luzener Kantonsspital (M Peter); Zofingen, Spital (S Gasser); Zollikerberg, Spital (R Fatio); Zug, Kantonsspital (M Vogt/D Ramsay); Zürich, Hirslanden Klinik (C Wyss); Zürich, Hirslanden Klinik imPark (O Bertel); Zürich, Universitätsspital (M Maggiorini); Zürich, Stadtspital Triemli (F Eberli); Zürich, Stadtspital Waid (SChristen).