Article Text

Abstract
We conducted a systematic review and meta-analysis to determine the effectiveness of healthcare provider-led (HCPs) interventions to support medication adherence in patients with acute coronary syndrome (ACS). A systematic search of Cochrane Library, Medline, EMBASE, PsycINFO, Web of Science, IPA, CINAHL, ASSIA, OpenGrey, EthOS, WorldCat and PQDT was undertaken. Interventions were deemed eligible if they included adult ACS patients, were HCP-led, measured medication adherence and randomised participants to parallel groups. Intervention content was coded using the Behaviour Change Technique (BCT) Taxonomy and data were pooled for analysis using random-effects models. Our search identified 8870 records, of which 27 were eligible (23 primary studies). A meta-analysis (n=9735) revealed HCP-led interventions increased the odds of medication adherence by 54% compared to control interventions (k=23, OR 1.54, 95% CI 1.26 to 1.88, I2=57.5%). After removing outliers, there was a 41% increase in the odds of medication adherence with moderate heterogeneity (k=21, OR 1.41, 95% CI 1.21 to 1.65, I2=35.3%). Interventions that included phone contact yielded (k=12, OR 1.63, 95% CI 1.25 to 2.12, I2=32.0%) a larger effect compared to those delivered exclusively in person. A total of 32/93 BCTs were identified across interventions (mean=4.7, SD=2.2) with ‘information about health consequences’ (BCT 5.1) (19/23) the most common. HCP-led interventions for ACS patients appear to have a small positive impact on medication adherence. While we were able to identify BCTs among interventions, data were insufficient to determine the impact of particular BCTs on study effectiveness.
PROSPERO registration number CRD42016037706.
- acute coronary syndrome
- medication adherence
- meta-analysis
- systematic review
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Pharmacological therapy is a key component of secondary prevention following acute coronary syndrome (ACS). Despite the effectiveness of such therapies, many patients do not follow their regimen as prescribed and are deemed non-adherent. It is estimated that approximately one-third of patients are non-adherent to cardiac medications following ACS.1 Non-adherence among cardiac patients presents a considerable clinical problem because of its association with poor outcomes that include mortality, morbidity and risk of rehospitalisation.2
Adherence is complex in nature and is driven by a myriad of patient-related (eg, beliefs about treatment), healthcare provider (HCP)-related (eg, communication) and healthcare system-wide factors (eg, treatment cost and access). A recent review of psychosocial factors found that depression and treatment beliefs were predictors of non-adherence following ACS.3 Identifying potentially modifiable factors is crucial for the design and implementation of evidence-based interventions to improve adherence.
There have been multiple attempts to synthesis the evidence base for adherence interventions in chronic disease,4 coronary artery disease (CAD)5 and cardiovascular disease.6 Moreover, there have been numerous reviews looking at interventions targeting adherence to specific medication classes including statins,7 antihypertensives8 and oral antiplatelet therapy.9 HCPs (ie, physicians, nurses, pharmacists) play a key role in supporting, promoting and monitoring adherence for chronic conditions. Previous reviews have reported the benefit of adherence interventions delivered by multiple HCPs,10 pharmacists11 and nurses.5 However, to date, the impact of these types of interventions for patients with ACS has yet to be systematically explored.
Interventions that target behaviours such as medication taking are often complex and comprise multiple components. In order to identify the specific strategies best suited to change specific behaviours, complex interventions need to be compartmentalised. Behaviour change frameworks such as the theoretical domains framework12 and behaviour change technique (BCT) taxonomy13 have been designed to aid this compartmentalisation process through specifying interventions into their ‘active content’. These types of models have been used across a range of health behaviours, and there is increasing application within medication adherence research.14
The primary objective of this systematic review and meta-analysis is to determine the effectiveness of HCP-led interventions to support medication adherence following ACS. Additionally, we aim to examine whether effectiveness is moderated by interventionist, delivery method and having a theory-based design. Finally, we aim use a behaviour change framework to identify the specific techniques used among adherence interventions.
Methodology
This review was conducted in accordance of the Preferred Reporting Items for Systematic reviews and Meta-Analysis guidelines15 and was registered with PROSPERO (http://www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42016037706).
Eligibility criteria
Studies were included if they met the following criteria:
Participants: adults (>18 years of age) with a confirmed diagnosis of ACS.
Intervention: delivered by HCPs.
Comparator: parallel group design where treatment group is compared with a clearly defined control group.
Outcome: include a measurement or medication adherence as a primary or secondary outcome.
Setting: study group allocation determined by randomisation.
We defined an intervention as being HCP led if the primary method of delivery involved HCPs working therapeutically with patients in person and/or via phone.
Studies infrequently distinguish between the different types of non-adherence; therefore, we used a definition of medication adherence that includes treatment initiation, actual dosing and treatment persistence.16
Search strategy
A systematic search of the following electronic databases was conducted: The Cochrane Library, Medline, EMBASE, PsycINFO, Web of Science, International Pharmaceutical Abstracts, Cumulative Index to Nursing and Allied Health Literature and Applied Social Sciences Index and Abstracts. An additional grey literature search was also undertaken: OpenGrey, EthOS, WorldCat—Thesis and Dissertations and ProQuest Dissertations & Theses. Searches were limited to articles written in English with no timespan limits. Reference lists of relevant papers were also searched to identify any additional records.
Our search strategy was informed by previous review studies4 5 and comprised four search themes: condition; therapy type; adherence; study design (see table 1) (for full search strategy, see online supplementary material 1).
Supplementary file 1
Search themes with example search terms
Data extraction
Records were imported into bibliographic software (EndNote X7) where duplicates were removed. All records were initially screened based on their title and abstract, and relevant articles were full-text screened using our eligibility criteria. All screening and data extraction was undertaken by a single researcher (JC) with experience conducting evidence syntheses. Two additional researchers (VA & JW) undertook partial screening using the eligibility criteria to validate the study selection and data extraction process. Any disagreements between raters (JC, VA and JW) were resolved by consensus. Data were extracted using a standardised data extraction form based on previous review studies4 5 17 (see table 2). Where necessary, study authors were contacted directly for additional information. We contacted 10 authors to clarify aspects of their methodology of which 80% responded.
Data extraction criteria
Risk of bias
Methodological quality was judged using A Cochrane Risk of Bias Assessment Tool (ACROBAT)18 where risk is rated as ‘high’, ‘unclear’ or ‘low’ among six domains of bias (Selection; Performance; Detection; Attrition; Reporting and Other Biases). ACROBAT has been used in previous systematic reviews looking at the effectiveness of adherence interventions.19 Risk of bias was assessed by a single researcher (JC).
Statistical analysis
Medication adherence was our target outcome, and the direction of effect was transformed for consistent reporting. Where studies reported adherence across multiple medications the data were pooled to provide an estimate of ‘overall adherence’. Effect size estimates are expressed in terms of ORs. Where data were originally expressed as means, standardised mean differences were calculated and then transformed to the OR metric using the probit method.20 These should be interpreted as standardised OR.
Random-effects models comparing HCP-led interventions with control interventions were used based on the assumption that there would be statistical heterogeneity from pooling primary study data. The I2 statistic was used to estimate statistical heterogeneity, and Cochrane guidelines were used for interpretation.21 Potential publication bias was determined using funnel plots and Egger’s test for small study effects. A critical value of. 1 was used for heterogeneity and small study effects significance testing. A study was deemed to be an outlier where the effect size was outside the pseudo 95% CI in the funnel plot as a means for detecting the potential impact of outliers on the pooled effect size.
Secondary studies (ie, primary study data with alternate end-points) were excluded from meta-analysis so as not to duplicate data. Prespecified subgroup analyses were conducted based on (1) type of interventionist, (2) delivery method and (3) theory-based design. Additional post hoc analyses were done based on adherence outcome and risk of bias. All analyses were done using Stata 14.1.
Coding intervention content
We used the BCT taxonomy13 to identify specific techniques used to change medication-taking behaviour among our intervention studies. The BCT taxonomy comprises 93 unique BCTs categorised into 16 clusters. A BCT is defined as an ‘active ingredient’ that can be used to alter or redirect behaviour. The BCT taxonomy includes a detailed description of each technique and provides specific examples (eg, ‘action planning’ (BCT 1.4): ‘prompt planning the performance of a particular physical activity at a particular time on certain days of the week’ (the numbers in parentheses refer to the BCT’s taxonomy cluster)). The BCT taxonomy has been used to code the content of interventions across a range of health behaviours including medication adherence.14
The BCT content of each intervention was rated by two researchers (JC and LA). Intervention data were sourced from each published manuscript and relevant supporting documents (ie, study protocols, intervention manuals). The researchers initially rated the interventions independently and then met to discuss. BCT content was scrutinised until consensus was met between researchers.
Results
Selection process
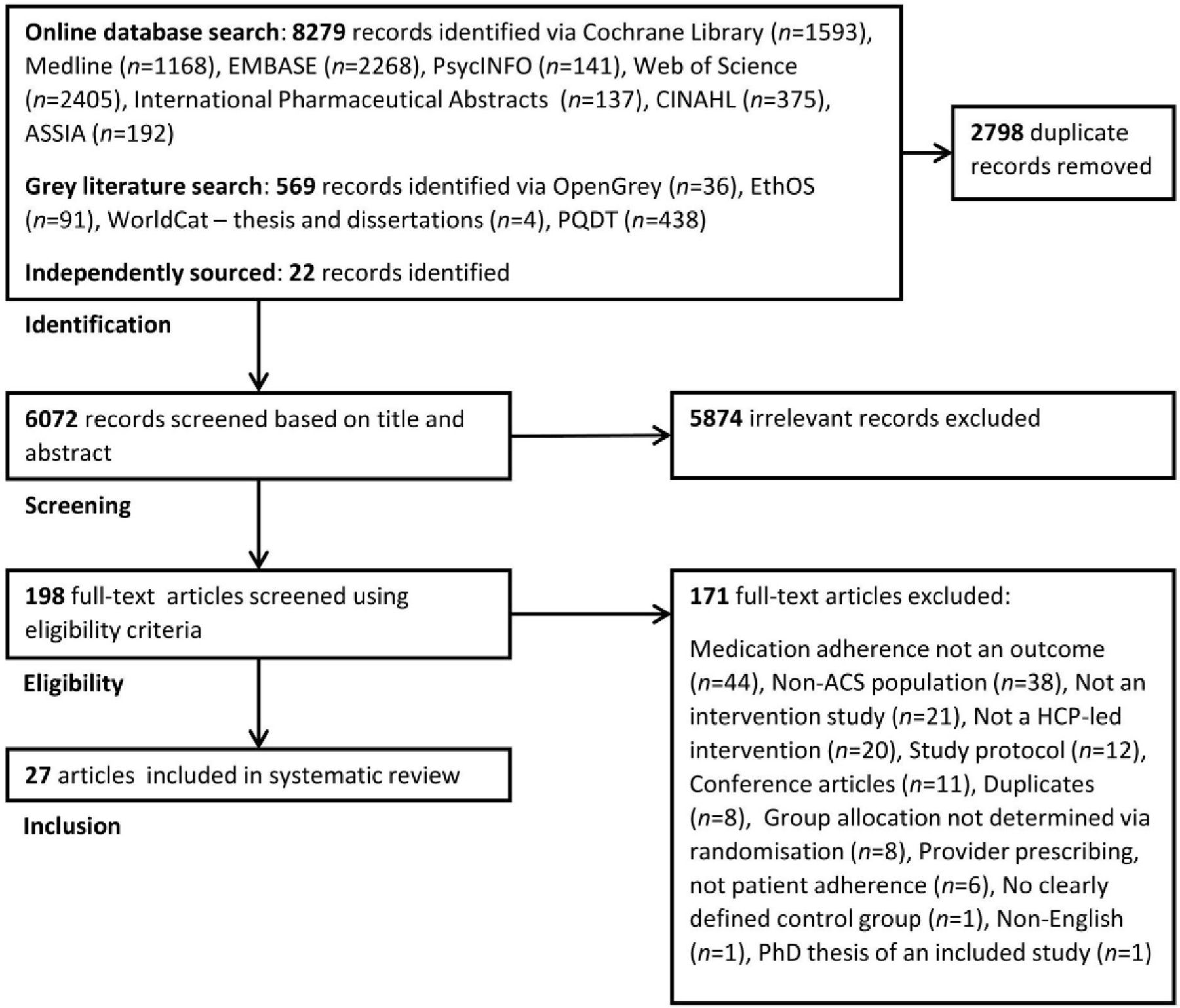
Our comprehensive search strategy identified 6072 records that were initially screened based on their title and abstract (see figure 1). A total of 5874 records were excluded, leaving 198 records to be full-text screened. Twenty-seven studies22–48 met our eligibility criteria, which comprised 23 primary studies (4 secondary studies37 38 43 47) (for full reason for exclusion list, see online supplementary material). Only primary study data (k=23, n=9735) will be discussed in the following sections.
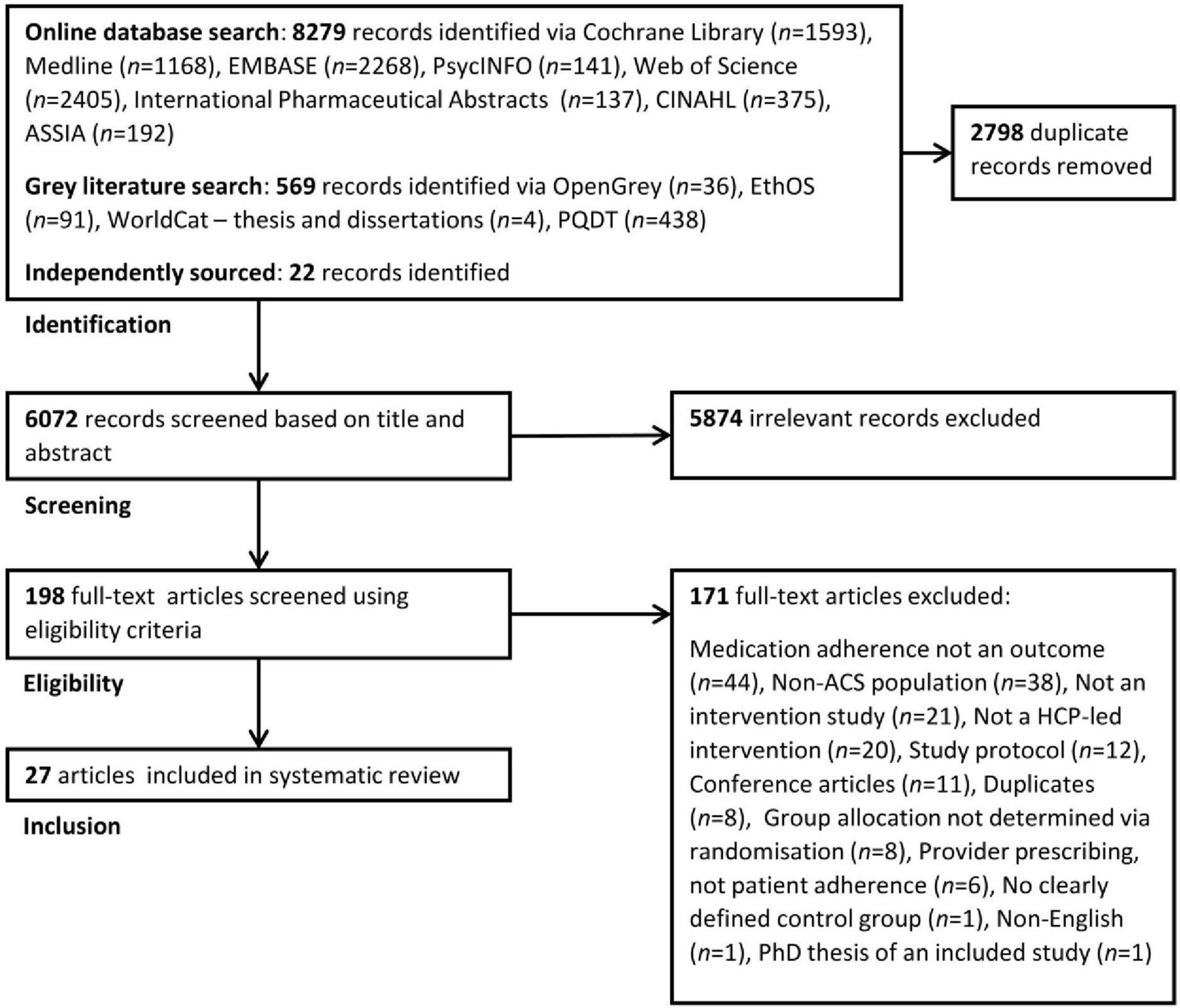
Preferred Reporting Items for Systematic reviews and Meta-Analysis flow diagram showing the study selection process. ACS, acute coronary syndrome; ASSIA, Applied Social Sciences Index and Abstracts; CINAHL, Cumulative Index to Nursing and Allied Health Literature; HCP, healthcare provider; PQDT, ProQuest Dissertations & Theses.
Study characteristics
Full details of the included studies can be found in table 3. The majority of interventions included nurses in their delivery (k=1323 24 26–28 31 33 35 36 40 42 45 48). Six interventions were led by pharmacists (k=622 29 30 32 41 48), and two were delivered by physicians (k=225 39). Physiotherapists,44 problem-solving therapists34 and community health workers46 acted as interventionists in singular trials. Nine studies were delivered exclusively in person (k=924 26 27 31 34 36 39 41 48), while 10 studies included both in person and phone contact (k=1022 23 29 30 32 33 42 44–46). Just four study interventions were delivered exclusively by phone (k=425 28 35 40), while six included a face-to-face predischarge component (k=622 23 28 30 39 41). The number of intervention sessions ranged from 128 32 48 to 2426 (k=21; median=4.0, SD=6.0). A total of 10 studies followed patients up for either 6 (k=522 24 32 34 39) or 12 months (k=529–31 46 48) (k=23; median=6.0 months, SD=10.3 months). Adherence to medication was a primary outcome in 14 studies (k=1422 24 28–30 32 34 36 39–42 45 46) and was measured exclusively by self-report in 16 studies (k=1623–28 31–34 36 39–41 44 45). Five studies used pharmacy data or pill counts (k=530 35 42 46 48), and just two studies used both self-report and pharmacy data to measure adherence (k=222 29).
Data extraction for all intervention studies identified in the systematic review process (k=27)
Risk of bias
A summary of the risk of bias assessment can be seen in figure 2. All but one of the studies31 were rated as having ‘unclear’ risk of performance bias due to the impracticality of blinding participants and personnel to group allocation during behavioural studies. ‘High’ risk of detection bias was judged in nine studies that did not adopt end-point blinding (k=924 26 28 36 39 40 44 45 48). After excluding performance bias ratings, six studies were judged to have ‘low’ risk of bias across all other domains (k=622 27 30 34 41 44). Three of these ‘low-risk’ studies were delivered by pharmacists (k=322 30 41), and the rest were led by nurses,27 physiotherapists44 or problem-solving therapists.34 Trials with the smallest41 and largest sample sizes27 were among the ‘low risk’-rated studies, and all six were either delivered exclusively in person (k=327 34 41) or in person with phone contact (k=322 30 44) (for complete risk of bias assessment, see online supplementary material).
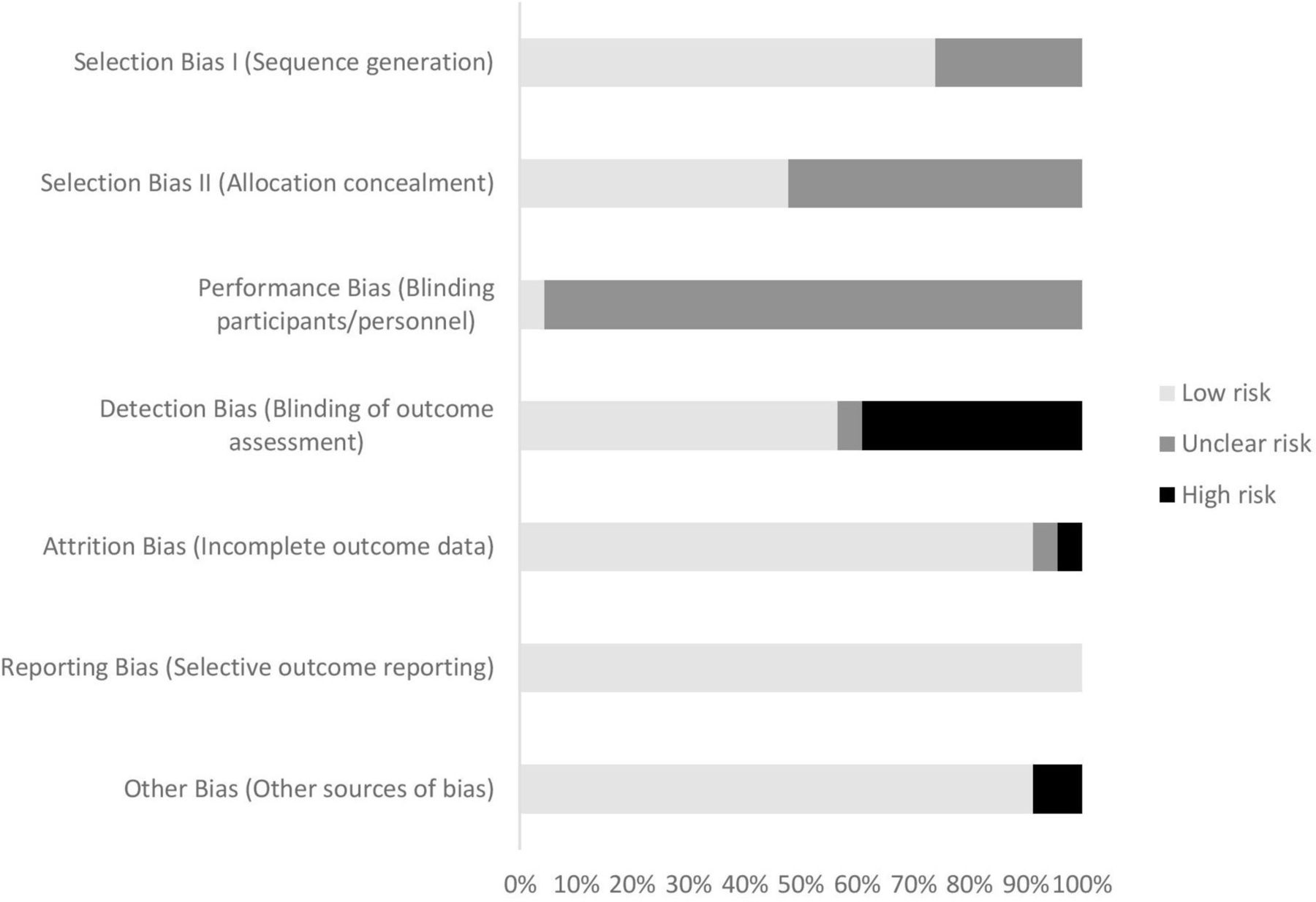
Risk of bias assessment.
BCT inclusion
Figure 3 shows the frequency of BCTs coded across studies. None of the studies referenced the BCT taxonomy in their intervention design. A total of 32 (34%) of the 93 BCTs listed in the taxonomy were identified among studies, ranging between 128 33 and 1044 (mean=4.7, SD=2.2). ‘Information about health consequences’ (BCT 5.1) was the most commonly identified BCT, coded in 19 of the 23 studies. ‘Social support (unspecified)’ (BCT 3.1) was coded in seven studies, and ‘action planning’ (BCT 1.4) was identified in just two studies.32 44 There were six instances of ‘goal setting (outcome)’ (BCT 1.3), ‘monitoring of behaviour by others without feedback’ (BCT 2.1), ‘feedback on outcome(s) of behaviour’ (BCT 2.7) and ‘instruction on how to perform the behaviour’ (BCT 4.1) across studies. Around two-thirds (67%) of the total number of BCTs coded were from just three taxonomy clusters: goals and planning (cluster 1, n=26 (24%)), natural consequences (cluster 5, n=25 (23%)) and feedback and monitoring (cluster 2, n=21 (20%)). There were no BCTs coded from three taxonomy clusters: reward and threat (cluster 10), scheduled consequences (cluster 14) and covert learning (cluster 16). There were no instances where every BCT in a cluster was coded (goals and planning: cluster 1, 8/9 BCTs coded; feedback and monitoring: cluster 2, 6/7 BCTs coded).

Frequency of BCTs identified among interventions. BCT, behaviour change technique.
Meta-analysis
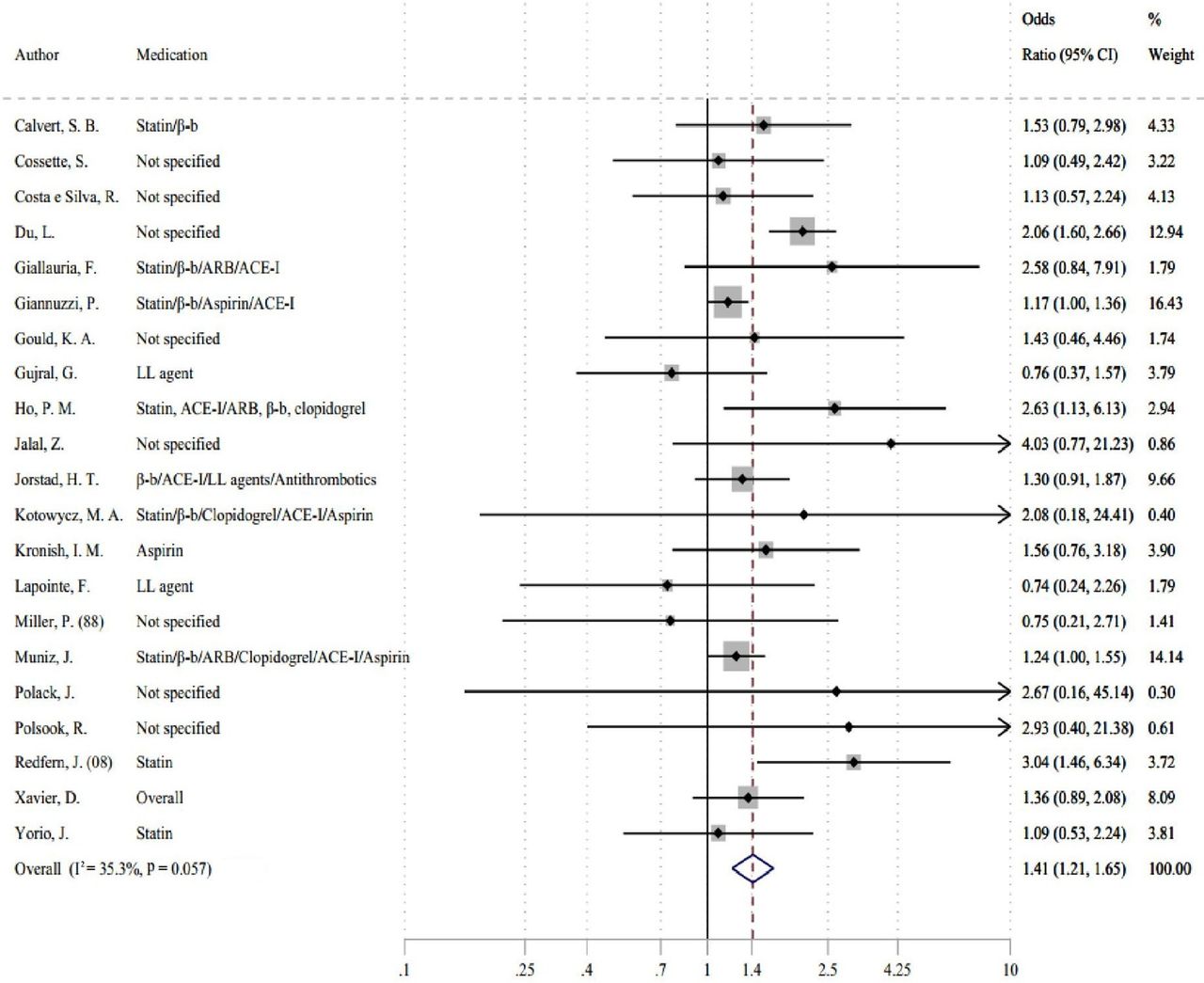
A random-effects meta-analysis of 23 primary studies (n=9735) revealed that HCP-led interventions increased the odds of medication adherence by 54% compared with control interventions with moderate to high statistical heterogeneity (k=23, OR 1.54, 95% CI 1.26 to 1.88 (I2=57.5%, P=0.001)) (see figure 4). After removing two outliers,40 45 a meta-analysis of 9545 patients indicated that HCP-led interventions increased the odds of medication adherence by 41% compared with control interventions with moderate statistical heterogeneity (k=21, OR 1.41, 95% CI 1.21 to 1.65 (I2=35.3%, P=0.057)) (see figure 5). While Egger’s test was non-significant (P=0.286), visual inspection of the funnel plot suggests a potential bias even after discounting outliers (for funnel plot, see online supplementary material).

Forest plot showing pooled effects size for healthcare-provider-led interventions on medication adherence (k=23, includes outliers).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot showing pooled effects size for healthcare-provider-led interventions on medication adherence (k=21, outliers removed).
Subgroup analyses
Table 4 shows the results of our prespecified (ie, interventionist, delivery method, theoretical basis) and post hoc (ie, adherence outcome, risk of bias) subgroup analyses. The largest effect sizes were for interventions that included phone contact (k=12, OR 1.63, 95% CI 1.25 to 2.12), and there was a trend for better-quality studies (ie, ‘low’ risk of bias) to increase the odds of adherence (k=6, OR 1.69, 95% CI 1.15 to 2.47). A negligible positive effect was found for interventions delivered by nurses (k=11, OR 1.19, 95% CI 1.04 to 1.36), and pharmacist-led interventions had a small though non-significant effect on medication adherence (k=6, OR 1.44, 95% CI 0.92 to 2.26). Studies led by HCPs other than nurses and pharmacists (ie, physicians,25 39 physiotherapists,44 problem-solving therapists,34 community health workers46) yielded a small positive effect on medication adherence (k=5, OR 1.66, 95% CI 1.22 to 2.24). We found no discernible differences in effect size between studies that included adherence as a primary or secondary outcome, and a small number of theoretically informed studies had a non-significant trend towards a negative effect on adherence (k=4, OR 0.94, 95% CI 0.60 to 1.49).
Overall effects and subgroup analyses for medication adherence interventions
Discussion
The primary objective of this study was to identify interventions led by HCPs to improve medication adherence following ACS. Meta-analysis revealed a small effect of HCP-led interventions on medication adherence. Our results are consistent with previous meta-analysis studies that have looked at the effectiveness of adherence interventions in other cardiac patient populations.5 17
In line with recent adherence literature,49 the majority of intervention studies identified were delivered by nurses or pharmacists. However, we found no indication that study effectiveness was moderated by the HCP delivering the intervention. Studies that included nurses in their delivery had a negligible effect towards better medication adherence, which does not correspond to findings from another meta-analysis that found that nurse-led interventions had a small to medium effect on adherence in patients with CAD.5 Six pharmacist-led interventions had a small but non-significant effect on medication adherence, which is congruous with previous reviews across cardiac-related diseases.5 17 Objectively, pharmacists should be ideal candidates to deliver adherence interventions due to the necessary knowledge and skills they possess to promote and support medication-taking behaviour.50 A meta-analysis of 771 medication adherence intervention trials found that the most effective interventions were delivered by pharmacists,49 which suggests that pharmacists may be better utilsied in other patient populations. Our findings should, however, be interpreted with caution due to the small number of pharmacist-led studies included in our analyses.
In terms of delivery method, interventions that included phone contact had higher odds of medication adherence compared with interventions delivered exclusively in person. Phone-delivered interventions may be a more convenient method to reach patients after discharge to monitor and encourage good medication adherence over time. Half of the interventions that included phone contact also contained a face-to-face predischarge component. Cutrona et al 51 found that two-thirds of interventions delivered at discharge were effective at improving adherence to cardiovascular medicines. Periods of care transition such as during hospital discharge are ideal opportunities to discuss treatment to pre-empt potential barriers to regimen adherence. Moreover, the dynamic nature of adherence dictates that monitoring of medication-taking behaviour over time by both patients and/or HCPs is crucial to ensure therapy maintenance for long-term conditions such as ACS.
We expected to find a greater proportion of interventions that used theoretical approaches to change medication-taking behaviour. There were only four studies that reported a theoretical basis, of which just one was based on a model of medication-taking behaviour (necessity–concerns framework52). A review by Conn et al 53 found that theory-driven interventions had a significant but modest effect on medication adherence. Our findings suggest that theory-driven adherence interventions for ACS are lacking, thus highlighting an important avenue for future research.
Coding intervention content
To our knowledge, this review is the first to use the BCT taxonomy to code interventions that targeted adherence across all cardiac medications following ACS. The BCT taxonomy provided a useful tool to analyse the content of adherence interventions, and we found that one-third of all BCTs detailed in the taxonomy were identified in at least one intervention. This relatively small number of total BCTs identified was unsurprising as many were not applicable to medication-taking behaviour. It is likely that additional strategies may have been used among interventions but were not identified due to a lack of detail in the description of the intervention. A lack of transparency in study reporting is an issue that limits the usability and replicability of interventional research. Checklists such as TIDieR54 are becoming commonplace to improve the quality of intervention reporting.
Written, verbal or visual information provision about the consequences of adherence (BCT 5.1) was by far the most frequently used BCT among HCP-led interventions. Discussing the consequences of non-adherence may help to strengthen patients’ beliefs in the necessity of their medications, which have been shown to predict non-adherence.55 While information is necessary to improve patients’ knowledge, it is not sufficient as a standalone strategy to change behaviour. Information-only strategies have been found to be generally ineffective at changing complex behaviours such as adherence.56
Clinical and research implications
Medication taking is a complex behaviour that can be difficult to change. Targeting patients identified with an adherence issue rather than all medication-takers may be one strategy to improve the effectiveness of adherence interventions. Cutrona et al 57 reported that ‘broad’ interventions (target all medication-takers) were less effective than ‘focused’ (target non-adherers only). None of the studies identified in this review targeted non-adherers; therefore, it is not yet known whether ‘focused’ interventions would be more appropriate for patients with ACS.
There were a variety of adherence measures used among included interventions, most of which were non-validated self-report tools. While an approach that combines self-reporting with an objective measure (eg, prescription refill records) is considered best practice, just two interventions followed this guidance. No studies used electronic monitors (eg, Medication Event Monitoring System) that provide real-time data on medication-taking behaviour58 and have been used to good effect in studies with patients with hypertension,59 heart failure60 and CAD.61 There is potential for objective measures to be used in conjunction with self-report tools to provide a more reliable and accurate representation of medication-taking behaviour of patients with ACS.
Strengths and limitations
The strengths of this study include the adoption of a comprehensive search strategy that comprised eight online databases and a supplementary grey literature search. Additionally, we applied an existing behaviour change framework to identify specific techniques used among HCP-led adherence interventions, which we believe is a novel approach for trials with patients with ACS. Our study does also include certain limitations. First, while we were successful in BCT identification, there were insufficient data to determine the effectiveness of particular BCTs. A larger data set would be required to undertake the type of meta-regression analyses that have recently been reported within the adherence literature.62 Second, we found relatively high levels of statistical heterogeneity in our random-effects models, which is inherent when comparing methodologically diverse behavioural interventions. We accounted for this variability by removing outliers, which resulted in our final model having moderate statistical heterogeneity. Third, only one researcher was involved in all aspects of the identification, screening, data extraction and risk of bias assessments, although dual-raters coded interventions independently using the BCT taxonomy. Best practice would be to include multiple independent raters in all stages of the review to ensure methodological rigour. Fourth, we decided not to exclude studies based on how medication adherence was measured, which was often done using unreliable self-report methods. A previous review by Santo et al 63 circumvented this issue somewhat by including stricter adherence measurement eligibility criteria. Ultimately, all methods of adherence measurement are limited in terms of practicality, reliability and cost, which represents a wider issue across the adherence literature.
Conclusion
This study suggests that HCP-led interventions have a small positive effect on medication adherence following ACS. An existing BCT taxonomy was used successfully to identify common techniques within adherence interventions. However, data were insufficient to draw firm conclusions regarding the impact of BCTs on intervention effectiveness. Information provision remains the basis of most adherence interventions. Further work is required to understand how intervention design and delivery determines the effectiveness of adherence interventions following ACS.
References
Footnotes
Contributors Concept design was undertaken by JC, VA and JW. JC undertook the literature search with VA and JW involved in eligibility screening. LA and SN contributed to behaviour change technique coding and statistical analyses, respectively. JC wrote the first draft, with all authors contributing to the critical revision of the manuscript.
Funding The authors report that this study was supported by a King’s College London-University of California, San Francisco PhD Studentship (for JC).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.