Article Text

Statistics from Altmetric.com
Can supplemental calcium increase cardiovascular risk?
A meta-analyses of randomised controlled studies of calcium supplementation (some including concurrent modest intakes of vitamin D) has observed a modest increase in risk for vascular events in the calcium-supplemented subjects.1 Some recent observational epidemiology in prospective cohorts has also linked supplemental calcium to increased vascular risk.2–4 Yet, rather perplexingly, relatively high dietary intakes of calcium have been associated with cardiovascular protection, or a neutral outcome in this regard.2 3 5 6 Moreover, there are theoretical grounds for expecting that superior calcium nutrition could be protective for vascular health. High-calcium diets decrease secretion of parathyroid hormone; even mild secondary hyperparathyroidism, common in the elderly, is suspected to increase vascular risk.7 8 A high calcium intake also tends to suppress absorption of dietary phosphate by forming an insoluble complex with it; emerging data suggest that high phosphate intakes may increase cardiovascular risk, even in those with normal renal function.9 High calcium intakes have not been found to correlate with increased risk for vascular calcification.10 The acute vascular impact of the modest rise in serum calcium following a bolus oral dose of calcium citrate has been studied; relative to placebo, arterial stiffness declined and myocardial perfusion increased in the calcium group.11 However, the diurnal decline in blood pressure was not as high in calcium-supplemented subjects and a coagulation index (thromboelastography) increased.12
What could explain the increased risk for vascular events associated specifically with calcium supplementation in some controlled studies? Even if subsequent analyses fail to confirm a net negative impact of calcium supplementation on vascular health—this issue is hotly debated and cannot be considered resolved5 13–15—the fact that calcium could be expected to protect the vasculature for certain reasons suggests that it must be exerting some countervailing negative effect even if its impact on vascular health is neutral.
The acute impact of bolus calcium on coagulation mechanisms, as noted above, merits further study. Also, a high calcium intake might increase secretion of renin—which increases cardiovascular risk16 via the prohypertensive, pro-oxidative effects of angiotensin II—by suppressing renal synthesis of calcitriol.17 Only a few pertinent clinical studies are currently available in this regard,18 19 however, and this prediction requires more verification in clinical studies using realistic supplemental intakes of calcium. Moreover, this explanation leaves unexplained the seeming discrepancy between the apparent cardioprotection of dietary calcium versus the potential cardiotoxicity of supplemental calcium.
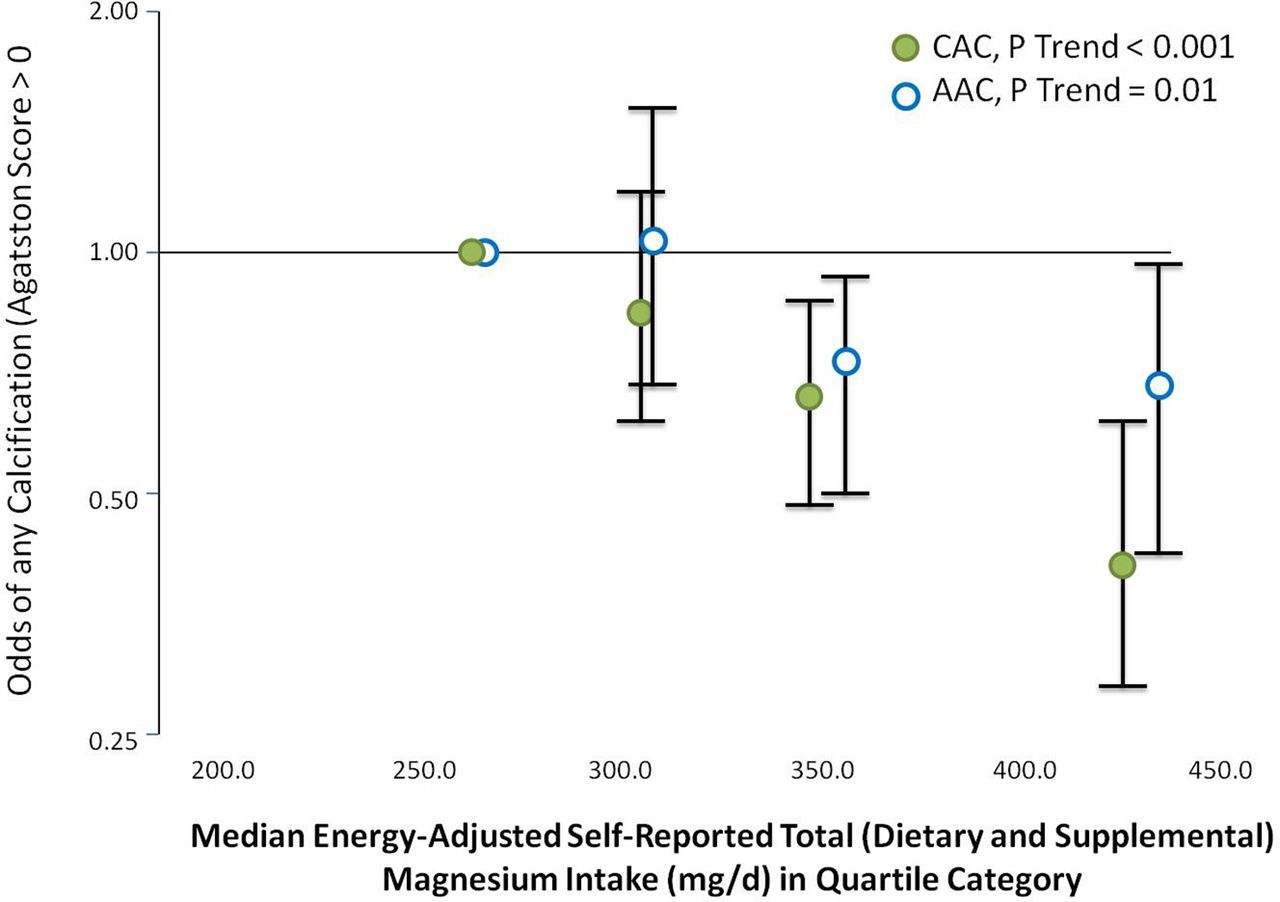
Consideration should, therefore, be given to the possibility that, in some individuals, high supplemental intakes of calcium may disturb magnesium balance.20 A great deal of recent epidemiology, including meta-analyses, points to higher dietary magnesium intakes, and/or higher serum magnesium levels, as associated with reduced risk for vascular events, arrhythmias, diabetes, hypertension, metabolic syndrome, vascular calcification and mortality.21–41 Although to some degree these observations likely reflect the benefits of consuming nutrient-rich whole foods, rather than just magnesium per se, magnesium still often emerges as protective after multiple regression analyses which try to adjust for this effect. Moreover, short-term studies of magnesium supplementation in persons at high cardiovascular risk have often found protective effects, particularly in those with low baseline magnesium status. Notably, in patients with coronary disease, magnesium supplementation has been found to decrease ex vivo platelet-dependent thrombosis, increase flow-mediated vasodilation of the brachial artery and during exercise, increase exercise tolerance, VO2max and left ventricular ejection fraction.42–46 A meta-analysis of placebo-controlled studies evaluating the impact of supplemental magnesium on treated hypertensives with baseline systolic pressure >155 mm Hg, found a mean reduction of 18.7 and 10.9 mm Hg in systolic and diastolic pressures, respectively, with high statistical significance.47 The mechanism of the apparent benefits conferred by good magnesium status requires further study, but it is suspected that magnesium antagonises some of the proinflammatory effects of increased cytoplasmic calcium.20 48–52 Indeed, magnesium has sometimes been referred to as ‘nature’s physiological calcium blocker’.53–55 For example, in physiological intracellular concentrations, magnesium competes with calcium for binding to calmodulin and other ‘EF-hand’ calcium-binding proteins, such that magnesium-bound proteins assume an ‘off’ configuration.50 52 The apparent ability of good magnesium status to diminish risk for vascular calcification is intriguing in light of recent epidemiology pointing to increased risk of coronary calcification in people using calcium supplements.4 40 41 56 Figure 1 depicts the inverse association between total dietary magnesium intake and risk for arterial calcification.56
{kind=link}
Adjusted odds of prevalent or high CAC and AAC according to self-reported total (dietary and supplemental) magnesium intake. Data from Hruby et al.56
Dietary calcium as a determinant of magnesium balance
In a series of magnesium balance studies conducted by Seelig about 50 years ago, she found that, in men with recommended dietary allowance (RDA)-level magnesium intakes (6 mg/kg/day or above), increasing dietary calcium to high levels did not impair magnesium balance— consistent with more recent reports.20 57 58 However, in men with relatively low intakes, a high calcium intake did indeed decrease magnesium balance. Somewhat paradoxically, a low calcium intake also impaired magnesium availability in this group. If these observations are confirmed in women, they imply that a high supplemental intake of calcium might impair magnesium balance in the rather high proportion of the population who have relatively low magnesium intakes, reflecting high intakes of ‘empty calorie’ foods. However, an increased intake of calcium-rich natural foods would not necessarily have a negative impact on magnesium balance because these foods also would supply magnesium. A cup of milk can provide up to 10% of the dietary magnesium requirement, for example.
Further balance studies are needed to confirm Seelig’s57observation that a high calcium intake can decrease magnesium balance when magnesium intakes are relatively low. Calcium and magnesium are not thought to share common transport proteins in the intestinal mucosa or renal tubular epithelium;59 60 it is, therefore, not clear what the mechanistic basis for such an antagonism might be. Inhibition of magnesium absorption by high dietary calcium is a well-established phenomenon in rats.61 Brink and colleagues have presented evidence that this phenomenon is contingent on a concurrent sufficiently high intake of phosphate.62 These researchers show in rats that an increased intake of calcium can decrease the ileal solubility of dietary magnesium by promoting the formation of insoluble calcium/magnesium/phosphate complexes. This phenomenon is most meaningful when the ratio of dietary phosphate to magnesium is relatively high, and Brink et al 62 suggest that the fact that this ratio is higher in rat diets than it tends to be in humans may account for the failure of high calcium intakes to suppress magnesium balance in most clinical studies. Nonetheless, many people who consume over-refined low magnesium diets also take in a high amount of bioavailable phosphate from animal products and phosphate additives63; this could be a subset of people in whom a high supplemental intake of calcium further compromises magnesium status.
Alternatively, it has been suggested that the suppression of parathyroid hormone and/or calcitriol associated with high intakes of calcium might downregulate the efficiency of magnesium absorption.64 Although intestinal magnesium absorption is primarily paracellular, active cellular transport via TRPM6 is likely to become more physiologically important as magnesium intakes decline.59 65 Several studies in humans, as well as in rats, conclude that calcitriol administration can enhance intestinal absorption of magnesium; jejunal absorption of magnesium was increased in the human studies.61 66–71 The possibility that vitamin D receptor activation might increase expression of TRPM6 in epithelial cells derived from jejunal mucosa does not appear to have been studied to date; such a mechanism could rationalise evidence that high calcium intakes only suppress magnesium balance when magnesium intake is low and hence more dependent on active cellular transport. Homeostatically, it would make sense that calcitriol, a signal to boost calcium uptake, would concurrently boost magnesium absorption, as maintaining a balance between calcium and magnesium levels is physiologically appropriate.
Balanced supplemental intakes of calcium and magnesium may be advisable
If high calcium intakes in humans can indeed impair magnesium balance when magnesium intakes are low, the clear implication is that calcium, when supplemented, should be given in conjunction with a balanced dose of magnesium; some authorities recommend a 2:1 ratio of calcium to magnesium (by weight) as most appropriate, both for supplementation and the total daily intake.72 73 This seems appropriate considering that good magnesium status also appears to favourably impact bone structure.74–76 The concept of ‘balancing’ calcium and magnesium in supplements has, in fact, been the accepted wisdom in ‘health food’ circles for decades, owing to Seelig’s research and its promulgation by popular health food pundits. However, the calcium supplements featured in pharmacies and supermarkets—where most people shop—typically feature only calcium and vitamin D. Research and promotional efforts sponsored by the dairy industry have insured that calcium is highly valued by the general public, whereas magnesium, no less crucial to health, is essentially an ‘orphan nutrient’, lacking the advocacy of commercial interests.
It should be noted that calcium/magnesium balance may cut both ways. In China, where the use of dairy products is low, dietary calcium/magnesium ratios tend to be much lower than in the West (1.7 vs 3). A recent analysis of prospective cohort studies in Shanghai has observed that, among people with a calcium/magnesium ratio under 1.7, an increasing intake of magnesium correlates with increased total mortality, whereas in those with a calcium/magnesium ratio above 1.7, increases in intake of magnesium and/or calcium correlated with reduced mortality risk.77 Hence, a high supplemental intake of magnesium may be inadvisable when calcium intakes are low.
Thus, more clinical studies examining the impact of varying calcium intakes on magnesium balance in subjects with low-normal magnesium intakes are clearly needed, as is a better understanding of the molecular mechanisms, whereby calcium can both positively and negatively influence magnesium absorption and retention. Future epidemiological studies should make an effort to differentiate calcium supplementers into those who either do or do not use supplemental magnesium concurrently, and also take into consideration dietary magnesium intake. In the mean time, people (especially those consuming a relatively refined diet) who wish to supplement with calcium might be well advised to take a supplement that also includes highly bioavailable magnesium, targeting a 2:1 calcium to magnesium ratio in the overall diet.
References
Footnotes
Contributors JJD, MFM, and JHO contributed to the final manuscript.
Funding This manuscript received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests JHO: Chief Medical Officer and Founder of CardioTabs, a nutraceutical company, have a major ownership interest in the company. CardioTabs does sell products that contain Omega-3. MFM: owner and science director of NutriGuard Research, a nutraceutical company. A few of NutriGuard’s products contain calcium and/or magnesium.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available for this paper.
Author note An earlier version of this article was previously published online at on February 2016.