Article Text

Abstract
Introduction Success rates of catheter ablation (CA) of persistent atrial fibrillation (AF) are very variable. Identifying patients in whom sinus rhythm maintenance cannot be achieved after CA is a critical issue.
Methods 2D speckle-tracking echocardiography was performed before the first CA procedure in consecutive patients with persistent AF. Left atrial (LA) strain was correlated with recurrence of atrial arrhythmias during the follow-up period of 15 months after one CA procedure with or without antiarrhythmic drugs (primary endpoint). In a secondary analysis, recurrences after two CA procedures were analysed.
Results 102 patients were included. Patients with recurrence of atrial arrhythmias after one CA procedure (n=55) had significantly lower LA strain than those without recurrence (LA strain 9.7±2.4% vs 16.2±3.0%; p<0.001). Recurrence rate was significantly higher in patients with LA strain <10% than in those with LA strain between 10% and 14.5% and >14.5% (97.7%, 42.1% and 10.3%, respectively; p<0.001). In Cox regression analysis including age, comorbidities, left ventricular dysfunction and LA enlargement, low LA strain (<10%) was the strongest factor associated with recurrence of AF (HR 6.4 (2.4–16.9), p<0.001). Even after inclusion of a second CA procedure, LA strain <10% maintained a high predictive value for recurrence of atrial arrhythmias (86.4% (95% CI 73.3% to 93.6%)).
Conclusion In patients with persistent AF, LA strain imaging could be very useful to select those patients who have a high risk of not benefiting from CA.
- atrial fibrillation
- catheter ablation
- left atrial strain
- atrial fibrillation recurrence
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
In previous studies, the normal range and the clinical relevance of the myocardial function of the left atrium using 2D speckle-tracking echocardiography (2DSTE) in patients with atrial fibrillation (AF) have been reported. In patients with paroxysmal AF, the assessment of diastolic and systolic left atrial (LA) myocardial function using 2DSTE can distinguish patients with high or low risk for recurrence of AF after catheter ablation (CA) therapy.
The clinical relevance of LA strain in patients with persistent AF is unknown and difficult to determine.
What does this study add?
In our study, LA strain could also be assessed in patients with persistent AF. During a follow-up period of 15 months, patients with low LA strain (<10%) had significantly worse results with CA in comparison with those without low LA strain. Low LA strain was the principal factor associated with recurrence of AF after CA. The predictive value of low LA strain for recurrences of atrial arrhythmias remained high even after redo procedures. Therefore, in patients with persistent AF, the analysis of LA strain could be of great usefulness to select those patients with a high risk of poor outcomes.
How might this impact on clinical practice?
LA strain analysis prior to ablation might help identifying patients with persistent AF with a high risk of recurrences of atrial arrhythmias even after two ablation procedures.
Introduction
The success rate of catheter ablation (CA) of persistent atrial fibrillation (AF) is very variable. Reported success rates range from 30% to 80%, often even despite several ablation attempts.1–8 Orthodox echocardiographic analyses of the left atrium (eg, left atrial (LA) diameter, LA area or LA volume) are frequently carried out prior to CA with the purpose of detecting LA myocardial alterations which could increase the risk of recurrence of AF after CA.9–12 Nonetheless, several investigations have recently demonstrated in diverse disorders that new myocardial techniques such as 2D speckle-tracking echocardiography (2DSTE) are able to detect myocardial alterations of the LA even when conventional echocardiographic analyses are normal.13 14 Hence, using 2DSTE before CA could significantly improve the management of patients with persistent AF, because these myocardial analyses, unlike conventional techniques could identify LA myocardial alterations linked to high risk of recurrence of AF as well as LA myocardial characteristics with low risk for AF recurrence.
Recent studies using 2DSTE have demonstrated the incremental clinical value of LA strain imaging over other clinical and echocardiographic factors to predict recurrence of AF after CA in patients with paroxysmal AF.14–17 However, the clinical relevance of LA strain imaging in patients with persistent AF remains poorly understood. Recently, just one small study suggested that a low value of LA strain could be an important factor linked to recurrence of AF after CA in patients with persistent AF.17 Nevertheless, that study was limited due to the small number of subjects with persistent AF (n=27), the short follow-up period (just 6 months, including the blanking period of the first 3 months) and because the determination of the cut-off of LA strain to predict recurrence of AF was determined by analysing only patients in sinus rhythm.17 Most patients with persistent AF, however, present with AF at the time of echocardiographic analysis. The purpose of this study was to validate the hypothesis, that in patients with persistent AF, analysis of the left atrium using LA strain imaging with the patient being in AF at the time of analysis could be of great usefulness to select those patients who have the highest risk of not benefiting from CA.
Methods
Study population
We included consecutive patients ≥18 years of age with persistent AF in whom the first CA of AF was performed at our centre between January 2010 and January 2013. Persistent AF was defined according to the diagnostic criteria of the guidelines on AF and CA of the Heart Rhythm Society (HRS).18 Only patients with AF at the time of the echocardiographic analysis which was performed in the week prior to CA were included. The indication for CA was symptomatic persistent AF refractory or intolerant to antiarrhythmic medication. Informed consent was obtained from all subjects.
To create a homogenous group of patients for this study, the following patients were excluded:
History of long-standing persistent AF (>12 months o f continuous AF)
LA diameter >55 mm
Left ventricular ejection fraction (LVEF) <50%
Significant valvular heart disease (mild, moderate or severe mitral or aortic stenosis, and moderate or severe mitral, tricuspid or aortic regurgitation)
Unstable coronary artery disease (unstable angina pectoris or acute myocardial infarction within the last 30 days, subjects waiting for coronary artery bypass graft or within 90 days postoperatively, subjects with chronic stable angina and patients with evidence of myocardial ischaemia assessed by stress echocardiography)
Severe pulmonary disease (requirement of supplemental oxygen or need of treatment with corticoids)
Severe kidney disease (glomerular filtration rate <30 mL/min/1.73 m2, history of renal transplantation and dialysis)
Severe chronic liver disease or history of liver transplantation
Congenital heart disease
Pericardial disease characterised by pericardial effusion (echo-free space in end-diastole ≥5 mm) or constrictive pericarditis
Hyperthyroidism or hypothyroidism.
Furthermore, to minimise underestimations of LA myocardial measurements, patients with poor 2D imaging quality in one or more myocardial segments of the LA (not suitable for analysis by 2DSTE in apical 4-chamber and 2-chamber views) were also excluded from this study.
Conventional and speckle-tracking echocardiography
All patients were examined by transthoracic echocardiography at rest using a Vivid 7 or Vivid E9 ultrasound system (GE-Healthcare) followed by an offline analysis using 2DSTE (Echo-Pac 113.0) in the week prior to CA. The echocardiographic measurements and analyses were performed within 7 days prior to CA and during an episode of persistent AF. Left ventricular (LV) diameters, LV volumes, LV mass, LV hypertrophy and LVEF (Simpson’s method), and LA diameter, area, volume and LA enlargement (ie, LA diameter >40 mm, LA area >20 cm², LA volume >58 mL and LA volume index (LAVI) >28 mL/m²) were assessed and defined as recommended by the American Society of Echocardiography (ASE).19 The measurement of LA strain was performed at each LA myocardial segment of the apical 4-chamber and 2-chamber views.14 20 The average value of LA positive strain peak during the entire cardiac cycle from all LA segments was used for the final value of LA strain (see figure 1a–c).

Myocardial Analysis of the Left Atrium Using 2D Speckle-Tracking Echocardiography. The fragmented white curve indicates the average of LA strain from all segments of the LA. Figure 1a corresponds to a patient with persistent AF with high risk for AF recurrence (i.e. LA strain < 10%), whereas Figure 1b and 1c correspond to patients with persistent AF with moderate and low risk for AF recurrence after CA.
Furthermore, longitudinal systolic and diastolic function of the LV by means of LV strain and LV early-diastolic strain rate (SRe) analysing all segments of the LV were analysed.14 20–22 On the basis of previous studies, we defined LV longitudinal systolic and diastolic dysfunction as LV strain > −16% and LV SRe <0.95 s–1.14 20–22 All echocardiographic measurements using 2DSTE (mean frame rates 68.4±4.2 frames/s) and conventional 2D echocardiography were calculated as the average of three measurements and at conditions of respiratory (<20 breaths/min), haemodynamic (90–180 mm Hg of systolic blood pressure) and electrical (60–100 beats/min) stability. All persons involved in obtaining and analysing echocardiographic data were blinded to the clinical information of the patients and ablation outcomes.
CA procedure
CA was performed using an open irrigated-tip ablation catheter (IBI Therapy Cool Path Duo or IBI Therapy Cool Flex) and a circular mapping catheter (IBI Inquiry Optima), which were positioned in the left atriumafter double trans-septal puncture under fluoroscopic guidance. A steerable sheath (Agilis, St. Jude Medical) was used in all procedures to support manipulation and stability of the ablation catheter. The geometry of the left atrium was reconstructed using a 3D mapping system (Ensite NavX, St. Jude Medical). Wide area circumferential pulmonary vein isolation was carried out with the irrigated-tip catheter with a maximal power of 35 W and a maximal temperature of 43°C. The course of the oesophagus was identified using a SensiTherm (St. Jude Medical) thermal probe. Radio frequency (RF) delivery was terminated and continued with decreased power whenever the oesophageal temperature exceeded 39°C. Complete isolation of all pulmonary veins was thoroughly verified by the circular catheter. Besides pulmonary vein isolation, additional ablation lesions such as LA linear lesion (LA roof line and mitral isthmus line) and ablation of regions with complex fractionated electrograms were placed in case AF could not be electrically cardioverted after pulmonary vein isolation.
Primary endpoint and follow-up period
The primary endpoint was the rate of recurrence of AF, atrial flutter (AFL) or atrial tachycardia (AT) (referred to as recurrence of atrial arrhythmias) after the first CA during a follow-up period of 15 months with or without antiarrhythmic drugs. We analysed the first recurrence of AF (defined as any documented episode >30 s) without taking into account early recurrences corresponding to the blanking period of the first 3 months after the initial CA. The patients were followed up in our outpatient clinic after 3 months and then after each 6 months. During these visits, we verified the maintenance of sinus rhythm using Holter monitoring. In addition, all patients were instructed to contact our department in case of any symptoms suggestive of arrhythmia with the purpose of obtaining an ECG or Holter to confirm or exclude recurrence of atrial arrhythmias.
Secondary endpoint
The secondary endpoint was the rate of recurrence of atrial arrhythmias after two CA procedures with or without antiarrhythmic drugs.
Statistical analysis
Continuous data were presented as mean ± SD and dichotomous data in percentage. Differences in continuous variables between groups were analysed using Student’s t-test. Categorical variables were compared by χ2 test and Fisher’s exact test as appropriate. Comparisons between three or more groups were analysed using a one-way analysis of variance. Based on previous findings in patients with paroxysmal AF,14 we estimated a rate of recurrence of AF to 15 months after CA at 70% in patients with low LA strain and at 15% in those without low LA strain. Thus, in order to detect a possible difference of 55% in the primary outcome between patients with and without low LA strain, a minimal sample size of 15 subjects in each group was estimated, with the purpose of having a statistical power of 80% with a confidence level of 0.05. Accordingly, assuming a probable rate of excluded subjects at 10–20%, a possible dropout rate at 15–20% and a possible prevalence of low LA strain at about 40%, we targeted to include a total of 100 patients with persistent AF.
To determine the reproducibility of LA strain using speckle-tracking echocardiography in patients with AF, we analysed intraobserver and interobserver variability. Intraobserver variability had a mean absolute difference of 0.9%±0.5% (maximum 2.1%). Interobserver variability had a mean absolute difference of 0.8%±0.6% (maximum 1.0%).
Receiver operating characteristic curves were calculated to evaluate the association of LA strain with the primary endpoint. An optimal cut-off value was chosen as one with optimal specificity (>90%) and sensitivity (>70%). In addition, we tested the relation of those cut-off points of LA strain to determine the primary endpoint and secondary endpoint. In this regard, a Cox regression analysis was performed. HRs with corresponding 95% CIs were then described. In order to determine the factors related to low LA strain, a logistic regression analysis was performed.
Differences were considered statistically significant when p < 0.05. All statistical analyses were performed with StatView V.5.0 (SAS Institute) and SPSS Statistics V.22.0 (IBM).
Results
Study population and outcomes
A total of 108 patients with persistent AF met the eligibility criteria during the inclusion period. However, sixpatients could not be enrolled because of poor 2D imaging quality in one or more segments of the. Thus, 102 patients were finally included and followed up during a period of 15 months. Although nine patients (9%) missed one of the scheduled outpatient follow-up visits between months 3 and months 15, AF recurrence status at the final follow-up visit at 15 months could be obtained for all patients.
In the primary endpoint analysis (recurrence of documented atrial arrhythmia after one CA procedure, with or without antiarrhythmic drugs), 55 patients (54%) had a recurrence during the follow-up period. In 31% of the patients with a recurrence, the recurring arrhythmia was paroxysmal AF, in 51% persistent AF and in 18% AFL/AT.
In the secondary endpoint analysis (recurrence of documented atrial arrhythmia after two CA procedures, with or without antiarrhythmic drugs), 42 patients (41%) had a recurrence during the follow-up period.
No patient suffered a sudden death, ventricular tachycardia or acute coronary syndrome during the follow-up time. Baseline characteristics of the patients are shown in table 1.
Study population
Characteristics of patients with recurrence of AF after one CA procedure (primary endpoint)
Patients with recurrence of AF after one CA procedure were principally characterised by a lower LA strain in comparison with those without AF recurrence (LA strain 9.7±2.4% vs 16.2±3.0%; p<0.001; see table 2). In contrast, LA volumetric characteristics (analysed by conventional echocardiography) were similar in patients with and without recurrence of AF (see table 2). Furthermore, it is important to note that there were no significant differences in the duration of AF or in the type of CA between patients with and without AF recurrence (see table 2).
Characteristics of patients with recurrence of AF after one catheter ablation procedure (primary endpoint)
Association of LA strain with recurrence of AF after one CA procedure (primary endpoint)
LA strain showed a significant association with both recurrence and non-recurrence of AF (area under the curve: 0.941; p<0.001) (see figure 2a and b). The best cut-off point related to recurrence of AF was a value of LA strain at 10% (specificity 97.9% and sensitivity 78.2%), whereas the best cut-off point linked to non-recurrence of AF was a value of LA strain at 14.5% (specificity 92.7% and sensitivity 74.5%) (see figure 2a and b). Thus, a value of LA strain between 10% and 14.5% was determined as moderate risk regarding the risk of AF recurrence. There was no association of LA strain with the type of arrhythmia recurrence (eg, paroxysmal or persistent AF or AT).
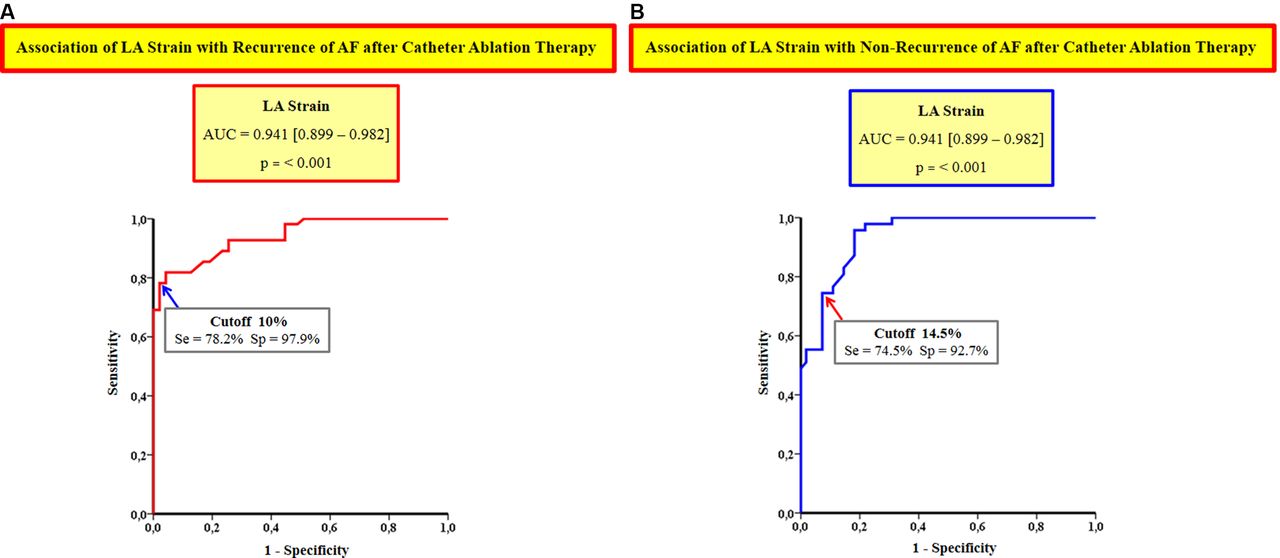
AF, atrial fibrillation; AUC, area under the curve; Se, sensitivity; Sp, specificity.
Incremental clinical value of LA strain over conventional LA measurements and comorbidities to predict recurrence of AF after one CA procedure (primary endpoint)
With the purpose of evaluating clinical and echocardiographic factors linked to recurrence of AF after CA, a univariate and multivariate Cox regression analysis was performed. Standard measurements of the left atrium such as LA diameter >40 mm, LA area >20 cm², LA volume >58 mL and LAVI >28 mL/m² (ie, LA enlargement) were only weakly associated with recurrence of AF. Analysing the effect of age, comorbidities and LV characteristics on the recurrence of AF, there was also only a poor link between these clinical factors and recurrence of AF after CA. The CHADS2 index and the CHA2DS2-VASc index with a score ≥2 were also only weakly associated with recurrence of AF. In addition, LV characteristics such as LV diastolic and systolic dysfunction and LV hypertrophy were also feeble predictors of AF recurrence after CA (table 3).
Clinical and echocardiographic predictors of recurrence of AF after one catheter ablation (CA) procedure (primary endpoint)
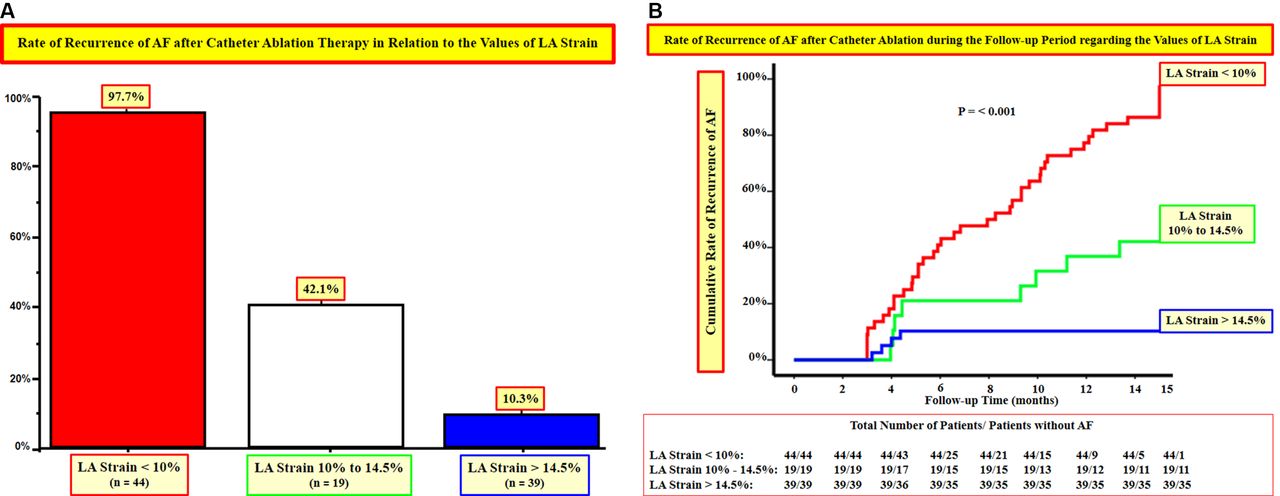
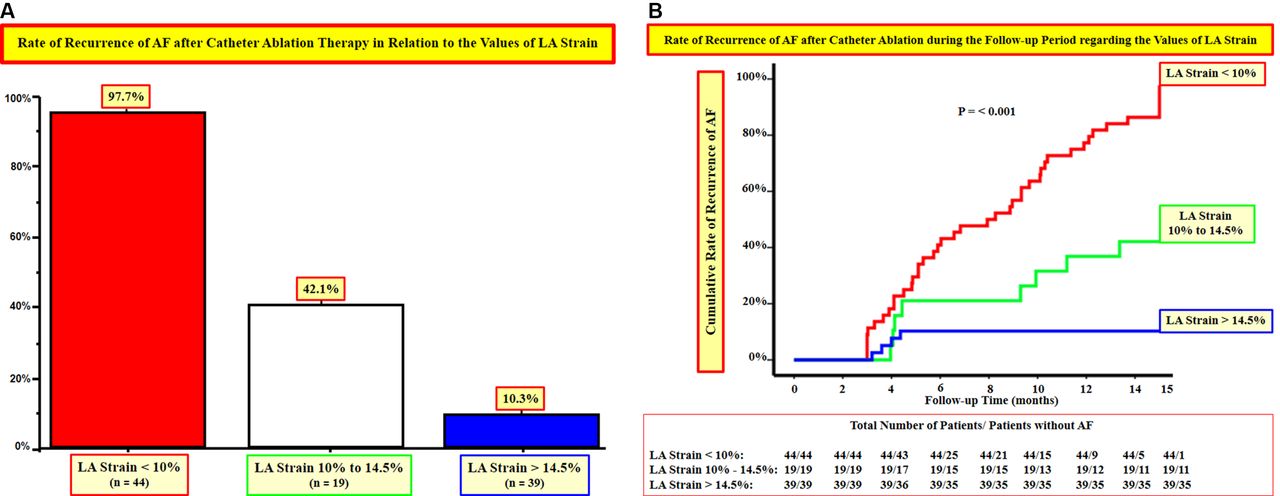
An LA strain showed a strong association with recurrence of AF after CA. An LA strain <10% was a strong predictor of AF recurrence (HR 6.4 (2.4–16.9), p<0.001; table 3), whereas an LA strain between 10% and 14.5% and >14.5% presented moderate and low risk for AF recurrence (HR 0.7 (0.3–1.4), p = 0.305 and HR 0.2 (0.05–0.7), p<0.001; respectively). In relation to these findings, the rate of recurrence of AF during the entire follow-up period was significantly higher in patients with LA strain <10% than in those with LA strain between 10% and 14.5% and LA strain >14.5% (15 months AF recurrence rate: 97.7%, 42.1% and 10.3%, respectively; p<0.001; see figure 3a and b).
{kind=link}
{kind=link}
{kind=link}
AF, atrial fibrillation.
In contrast, concerning conventional LA measurements, there were no important differences in the rate of recurrence of AF between patients with or without LA enlargement (LA diameter >40 mm vs ≤40 mm = recurrence of AF 58.8% vs 49%, p 0.325; LA area >20 cm² vs ≤20 cm² = recurrence of AF 63.6% vs 46.6%, p 0.088; LA volume >58 mL vs ≤58 mL = recurrence of AF 59.6% vs 49.1%, p 0.294 and LAVI >28 mL/m² vs ≤28 mL/m² = recurrence of AF 64.7% vs 43.1%, p 0.029).
Accuracy of LA strain to predict recurrence and non-recurrence of AF after one CA procedure (primary endpoint)
An LA strain <10% had a high positive predictive value (PPV) to determine recurrence of AF after CA (97.7% (95% CI 88.2% to 99.6%)) (see table 4). Likewise, an LA strain >14.5% had a high PPV to determine non-recurrence of AF (89.7% (95% CI 76.4% to 95.9%)) (table 4).
Accuracy of LA strain to predict outcomes after one catheter ablation (CA) procedure (primary endpoint)
Association of LA strain with recurrence of AF after two CA procedures (secondary endpoint)
An LA strain was also significantly associated with recurrence of atrial arrhythmias in the secondary outcome analysis (recurrence of atrial arrhythmias after two CA procedures, with or without antiarrhythmic drugs). The rate of recurrence of atrial arrhythmias after two CA procedures in patients with LA strain <10% was significantly higher than in those with LA strain between 10% and 14.5% and LA strain >14.5% (AF recurrence rate: 86%, 11% and 5%, respectively; p<0.001).
Accuracy of LA strain to predict recurrence and non-recurrence of AF after two CA procedures (secondary endpoint)
Even after two CA procedures, an LA strain <10% had a high PPV for recurrence of atrial arrhythmias (86.4% (95% CI 73.3% to 93.6%)). Likewise, an LA strain >14.5% had a high PPV to determine non-recurrence of atrial arrhythmias after two CA procedures (94.9% (95% CI 83.1% to 98.6%)).
Clinical factors associated with low LA strain
With reference to the factors that could be linked to low LA strain, the combination of comorbidities (determined by CHA2DS2-VASc index ≥2) and the longitudinal function of the LV were the principal variables associated with low LA strain (table 5). In addition, but to a lesser extent, LA enlargement was also linked to low LA strain (table 5).
Clinical and echocardiographic variables linked to low LA strain
Discussion
CA is an established method for the treatment of patients with paroxysmal AF.8 18 However, in patients with persistent AF, the results of CA are very variable. While some patients considerably benefit from this procedure, in others, sinus rhythm cannot be maintained for a reasonable amount of time, sometimes even despite several extensive ablation attempts.1 8 18 In the present study, we performed a comprehensive analysis of the factors associated with the results of CA in a large group of patients with persistent AF, in whom CA was performed with state-of-the-art technology.18 During a follow-up period of 15 months, we found that patients with low LA strain (<10%) had significantly worse results with CA in comparison with those without low LA strain. In a multivariate Cox regression analysis including clinical and echocardiographic factors, we found that a low LA strain was the principal factor associated with recurrence of AF after CA.
Patients with persistent AF included in previous studies that validated CA were pseudo-characterised as ‘without structural LA alterations’ using conventional echocardiographic measurements such as LA diameter or LA volume.7 8 18 These orthodox analyses were carried out with the purpose of excluding LA myocardial alterations which could generate recurrence of AF after CA.9–12 However, recent studies have demonstrated in diverse disorders that with the use of 2DSTE it is possible to detect myocardial alterations of the LA even when conventional echocardiographic analyses are normal.13 14 In line, the guidelines on AF and CA highlighted that volumetric LA measurements should be considered with caution because complex LA myocardial alterations linked to recurrence of AF could not be detected by conventional analyses of the LA.18
Recent investigations using LA strain imaging evidenced LA myocardial abnormalities linked to recurrence of AF after CA in patients with paroxysmal AF, which were not detectable by volumetric measurements of the left atrium.14 In addition, several studies showed the superiority of LA strain over conventional LA measurements and comorbidities to predict recurrence of AF after CA in subjects with paroxysmal AF.14–17 However, the clinical relevance of LA strain imaging exclusively in patients with persistent AF, especially those who present with AF at the time of LA strain analysis is so far unknown. In the present study, we found that a low LA strain (<10%) was strongly linked to recurrence of AF after CA in patients with persistent AF even after two CA procedures. On the contrary, we evidenced that in these patients conventional LA measurements as well as comorbidities were not predictive for recurrence of AF. Therefore, we consider that the analysis of the left atrium using LA strain imaging could be of great importance in the management of patients with persistent AF.
Since patients with persistent AF are often admitted with AF for counselling regarding therapeutic options, performing LA ‘functional’ analyses in sinus rhythm in these patients is often difficult and inconsistent.23–27 On the other hand, when LA analyses are performed during AF, LA myocardial measurements such as LA strain may be able to indirectly indicate the grade of LA fibrosis.28–30 In this regard, recent findings have proven the strong correlation of the grade of LA fibrosis as detected by cardiac MRI using dedicated software algorithms with LA strain in patients with persistent AF.28 29 In agreement, recent studies have demonstrated a significant link between the severity of LA fibrosis and the recurrence of AF after CA.30–34
Limitations
Some considerations should be taken into account on this study. Recent studies evidenced that 2DSTE values of the LV vary between different software packages such as GE, Philips and Toshiba.35 Thus, while there are no data showing a variability between different ultrasound software packages regarding LA analyses, LA strain values should be considered according to the ultrasound software package used (namely, the GE software was used in this study, which so far is the most extensively validated software to analyse the LA with 2DSTE).13 14 20 23 30 Furthermore, we did not compare the echocardiographic analyses of the left atrium with those performed by MRI, which recently has shown that it might have an interesting role in patients with persistent AF because it could detect LA fibrosis.31–34 Notwithstanding, recent findings evidenced a significant inverse relationship between the grade of LA fibrosis and the values of LA strain.28–30 Additionally, it is worth mentioning that the cut-off of LA strain to predict recurrence of AF after CA could only be applied to patients with the characteristics of inclusion of this study. Hence, patients with continuous AF >12 months or subjects in sinus rhythm might present different values of LA strain to determine recurrence of AF after CA.
Conclusions
Low LA strain (<10%) during AF is highly predictive for recurrence of atrial arrhythmias after one or two CA procedures in patients with persistent AF. Our findings suggest that analysis of LA strain could be of great usefulness to stratify patients with persistent AF prior to CA. These results should be further evaluated in multicentre trials.
References
Footnotes
Competing interests None declared.
Patient consent Patients included in this study had signed the patient consent form of our department approved by the ethics committee of Charité.
Ethics approval Charité – Universitätsmedizin Berlin ethics committee. The institutional review board approved this study (clinical research project EA211513).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There are no additional unpublished data from the study.