Article Text

Abstract
Background The presence of mitral valve prolapse (MVP) in congenital heart disease (CHD) patients is not well described. Tetralogy of Fallot (TOF) is the most common cyanotic CHD associated with overall good long-term survival after palliation. Since MVP is more often identified in adults and TOF patients are now surviving longer, we thus sought to perform this cohort study with a case–control design to (1) determine the prevalence of MVP and systolic displacement of mitral leaflets (SDML) in adult TOF patients, and (2) describe their clinical and imaging characteristics.
Methods Retrospective interrogation of our echocardiography database identified 328 consecutive TOF patients ≥18 years from 1 January 2000 to 31 December 2014. All images were reviewed to identify patients with concomitant MVP (prolapse >2 mm beyond the long-axis annular plane) or SDML (<2 mm beyond the annular plane).
Results 26 (8%) TOF patients fulfilled criteria for systolic mitral valve abnormality (SMVA) (15 MVP; 11 SDML). 2 had moderate to severe mitral regurgitation requiring repair. When compared with 52 TOF patients without SMVA, those with SMVA were more likely to be females (60.7% vs 33.9%, p=0.03), less likely to have transannular patch (52% vs 97.4%, p<0.0001), had lower right ventricular ejection fraction (36.5% vs 43.8%, p=0.03) and a trend towards increased risk of atrial (44% vs 30.4%, p=0.5) and ventricular arrhythmias (32% vs 25.5%, p=0.6). On multivariate logistic regression, SMVA was independently associated with the absence of transannular patch (p=0.002) and atrial arrhythmias (p=0.04).
Conclusions In this series of adult TOF patients, we describe a novel finding of a high prevalence of systolic mitral valve abnormalities.
- CONGENITAL HEART DISEASE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Tetralogy of Fallot (TOF) is the most common cyanotic congenital heart disease (CHD) lesion associated with excellent long-term survival after repair. It is primarily a cono-truncal abnormality and thus, the majority of sequelae and residue in adult TOF survivors usually include the right ventricle and the right ventricular outflow tract. Left heart abnormalities like left ventricular dysfunction have been described in these patients, but its association with mitral valve abnormalities has not been described. Mitral valve prolapse (MVP) is recognised more commonly in adults than children, and is known to be associated with various other conditions but has not been described in CHD patients. As TOF patients are surviving longer, we postulate higher prevalence of MVP in TOF patients.
What does this study add?
The increasing population of adults with congenital heart disease (CHD) is facing new challenges of increased comorbidities. While these patients are being evaluated in adulthood, greater vigilance for the presence of certain comorbidities might become crucial. This study described a novel association of systolic mitral valve abnormalities (SMVA) in Tetralogy of Fallot (TOF) patients at a much higher prevalence than the general population. Thus, our observation of increased prevalence of SMVA in TOF patients generates some important discussions regarding the pathophysiological basis as well as clinical relevance of these coexistent conditions.
How might this impact on clinical practice?
In clinical practice, the association of systolic mitral valve abnormalities (SMVA) in Tetralogy of Fallot (TOF) patients could be considered as infrequent and an incidental finding. The present study showing a high 8% prevalence of this association emphasizes the need to recognize this combination and underscores that SMVA in TOF patients might serve as a marker of increased risks of arrhythmias and reoperation. In this study, the arrhythmia prevalence in the TOF+SMVA group was higher than those without SMVA and atrial arrhythmia was independently associated with SMVA, suggesting the need for increased vigilance to look for SMVA in the presence of atrial arrhythmias or vice-versa in TOF patients.
Introduction
Mitral valve prolapse (MVP) is a clinically heterogenous,1 common valvular abnormality, afflicting 2–3% of the general population,2 and although the most common cause of severe non-ischaemic mitral regurgitation (MR) in USA,3 it has a widely varying spectrum of clinical severity and prognosis.1 Whether MVP is congenital or acquired is still debatable,4 and it is seen in combination with a number of other conditions,5–8 but its presence in congenital heart disease (CHD) patients is not well described.
The incidence of CHD is ∼1% or 40 000 births per year in the USA,9 and there are an estimated 1.3 million adults living with CHD; its prevalence in adults increasing by 5%/year.10 Tetralogy of Fallot (TOF) is the most common cyanotic CHD with a worldwide birth prevalence of 3.4%11 among CHD patients and excellent long-term survival after surgical repair.12 The basic anatomic abnormality in TOF is anterior and superior displacement of the conal septum, which results in a membranous ventricular septal defect, dextroposition of the aortic valve and root and narrowing of the right ventricular (RV) outflow tract. The precise cause of the development of TOF in humans is unknown. Cardiac development is a complex process including transcriptional/ signalling interactions between progenitor populations, including second heart field mesoderm, cardiac neural crest and two populations of endocardial cushions. Avian and murine models have shown that genetic or mechanical defects in each of these populations can result in phenotypes suggestive of TOF.13–15 The mitral valve leaflets are composed of endocardial cushion-derived mesenchyme, and clinical observations as well as data from the basic cardiac development literature suggest the possibility that a primary defect in endocardial cushion development may underlie a subset of the TOF phenotype.16 ,17 We reasoned that identification of subtle atrioventricular valvular abnormalities in TOF might shed light on the pathogenesis of both these common conditions.
Since MVP is more often identified in adults than children and TOF patients are now thriving well into their adult years, we sought to determine the prevalence of this most common adult valve abnormality in our adult TOF patients. Although the pathophysiological basis of this association remains unclear, we postulate that it may be due to primary defects in endocardial cushion maturation, haemodynamic changes or a combination of these as potential contributors.
Methods
Patients
Between 1 January 2000 and 31 December 2014, complete echocardiographic studies were obtained on 344 consecutive adult patients ≥18 years of age with TOF at University of California San Francisco. The echocardiographic images of all patients were reviewed to identify those who had any systolic mitral valve abnormalities (SMVA), primarily looking for minimal systolic displacement of the mitral leaflets (SDML) or MVP. Sixteen patients were excluded because the echocardiographic studies were judged to be technically suboptimal and four patients were excluded because they had concomitant atrioventricular septal defect. The remaining 324 patients comprise the present study group. Approval was obtained from our institutional review board.
Diagnostic criteria and assessment for systolic mitral abnormality
Echocardiographically, MVP was defined as single or bileaflet displacement at least 2 mm beyond the long-axis annular plane, with or without leaflet thickening, as viewed in the parasternal long-axis view or the long-axis and apical four-chamber views.18 If the displacement was <2 mm beyond the long-axis annular plane, then these patients were considered to have SDML.
We attempted to minimise the interobserver bias in the diagnosis of SMVA. One of the authors (AA) independently reviewed all images of every TOF patients with special emphasis given to the parasternal long-axis views and transoesophageal echocardiographic images, when available. If the patient had a pulmonary valve replacement (PVR), then pre-PVR and post-PVR images were also reviewed in detail to assess for any changes to the SMVA. All the echocardiographic studies of the patients with SMVA were reviewed retrospectively to identify the earliest age at which the mitral valve abnormality was first recognised. Two other authors (ISH and EF) then independently reviewed images of all the patients with any suspicion for SMVA, and classified them into either having no abnormality versus SDML versus MVP. Both of these authors were blinded to each other's observations, and only those patients for whom both the authors were in agreement about the SMVA classification were included in the TOF+SMVA group.
Data acquisition
For every SMVA patient, two age-matched TOF patients without SMVA were identified and formed the control group. Medical records were reviewed to document baseline demographics, presence of associated cardiac anomalies, genetic defects and personal and family histories. Information related to patients' clinical course, including details of their surgical and medical management and follow-up as well as imaging characteristics, was collected. Holter monitors and 12-lead ECG were examined for evidence of arrhythmia. Cardiac magnetic resonance (CMR) imaging if performed was reviewed in detail, especially to assess for the volumes and function of right and left ventricles, as well as the degree of pulmonary regurgitation (PR). The normal values for CMR-based left ventricular (LV) and RV dimensions were used as described previously.19 The most common reasons for not undergoing CMR was the presence of implantable defibrillator (ICD) or pacemaker followed by insurance denial or claustrophobia.
Echocardiography
All patients underwent complete 2D and Doppler echocardiographic examinations according to American Society of Echocardiography/European Society of echocardiography recommendations.20 LV dimensions were measured, and the severity of any valvular stenosis or regurgitation was graded as mild, moderate or severe.20–23 Biplane LV ejection fraction (LVEF) was calculated, with normal LVEF defined as 55–70%. Left atrial dimensions as well as RV size and function were assessed as recommended.20 ,24 Any additional findings such as other valvular or congenital cardiac anomalies were documented.
Statistical analysis
Continuous variables are summarised as mean±SD, and discrete categorical variables are presented as frequencies and percentages. Comparisons of continuous variables are performed using Student's t-test and of categorical variables using Fisher's exact test. We conducted multivariate logistic analyses (stepwise regression model) to identify independent associations of SMVA. A test for linear trend was performed to analyse the association of SMVA with RV ejection fraction (RVEF) on CMR. All analyses were performed using STATA/SE statistical software (V.14, StataCorp LP, College Station, Texas, USA).
Results
Study population
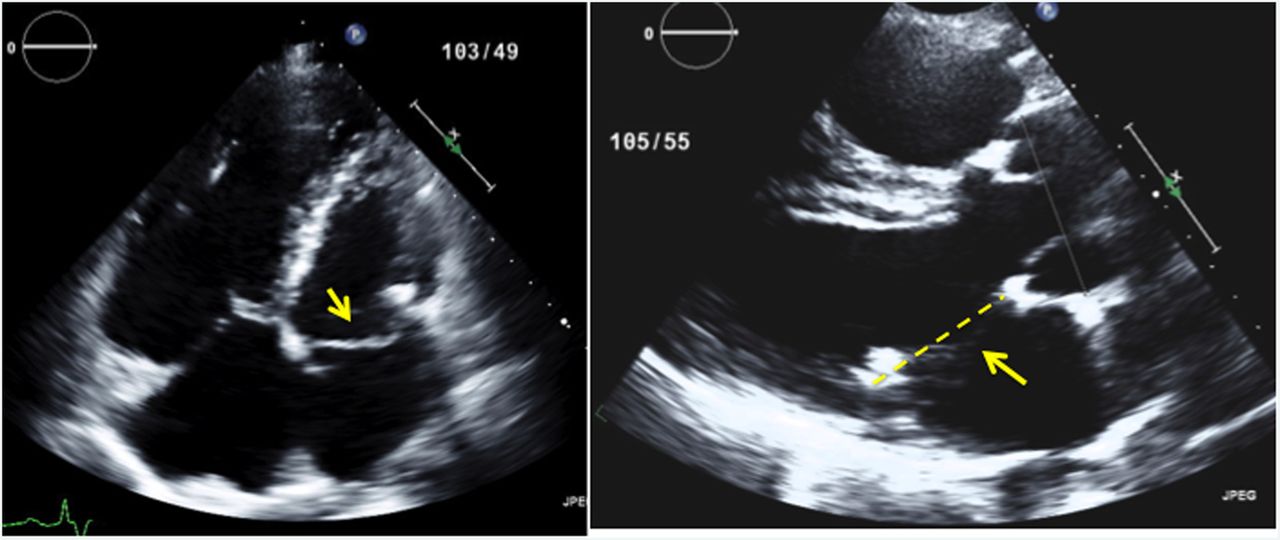
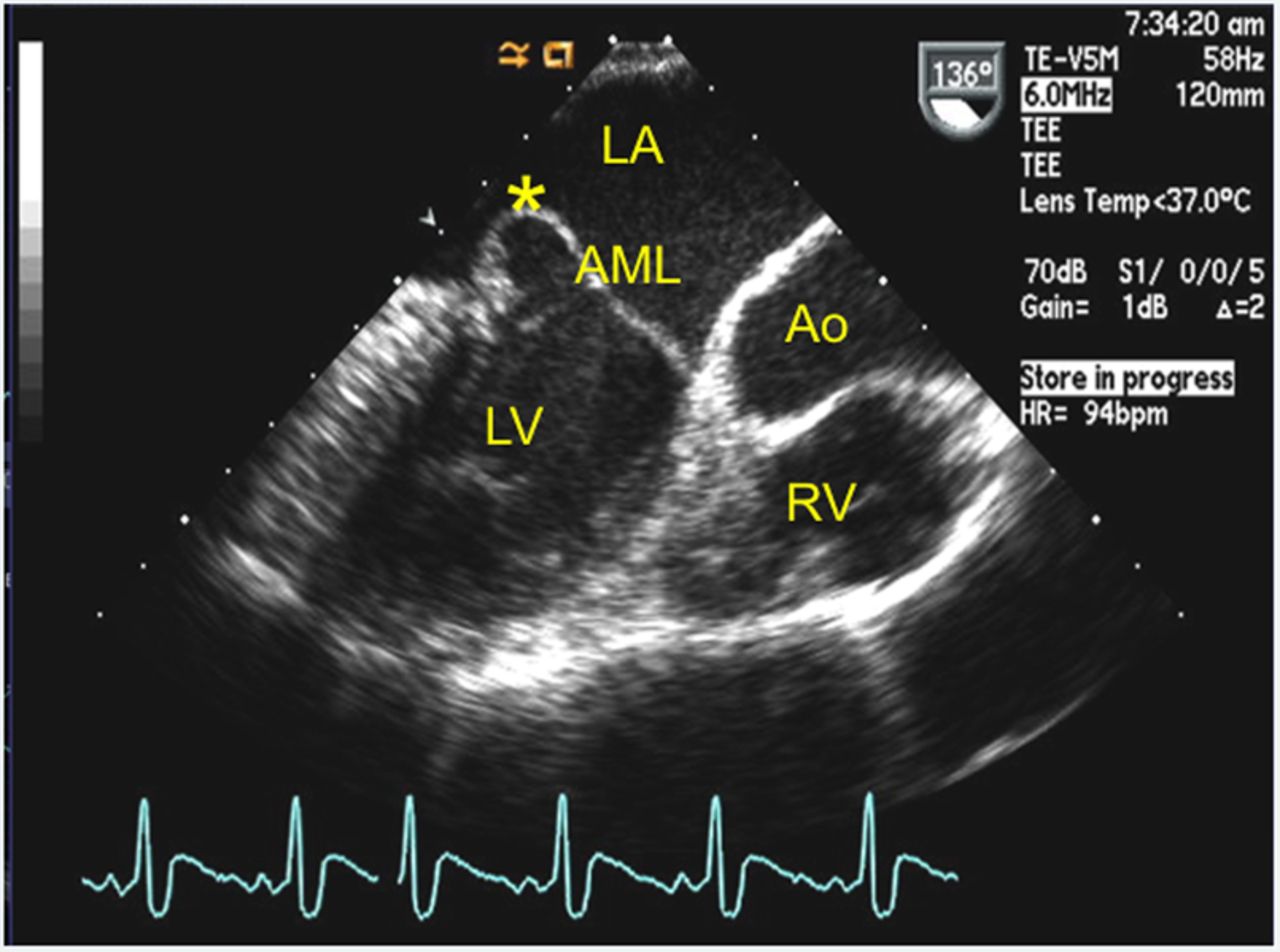
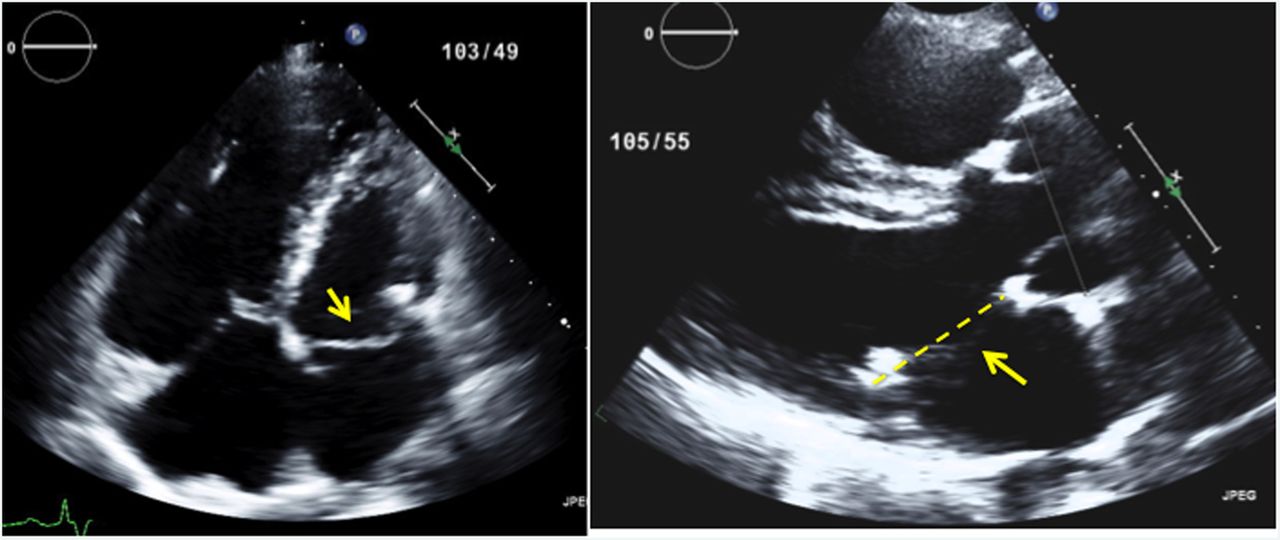
Of the 324 TOF patients ≥18 years, 26 (8%) patients fulfilled criteria for SMVA (15 (4.6%) MVP and 11 (3.4%) SDML). An illustrative image of a patient with MVP and a patient with SDML is shown in figures 1 and 2, respectively.

Illustrative transoesophageal echocardiographic image of a female aged 48 years with bileaflet prolapse and severe mitral regurgitation (LA, left atrium; AML, anterior mitral leaflet; Ao, aorta; LV, left ventricle; RV, right ventricle; *prolapsed AML).
{kind=link}
{kind=link}
Illustrative four-chamber (left) and parasternal long axis (right) echocardiographic image of a female aged 49 years with systolic displacement of anterior mitral leaflet (arrow: anterior leaflet, dotted line: mitral annular plane. Distance between the dotted line and arrow tip is <2 mm).
Clinical characteristics
The mean age of the patients with SMVA was 42.8±14.9 years (ranging from 19 to 64 years), while their mean age at the time of first recognition of the SMVA was 34.5±17.1 years. An SMVA was first recognised between 6 and 64 years of age on retrospective review of images. For patients with SDML, the mean age was 35±17.1 (median (25th, 75th) was 39 (18, 46)) years and for those with MVP, the mean age was 34±17.6 (median (25th, 75th) was 39 (21, 48)) years.
The most common TOF phenotype was severe pulmonary and infundibular stenosis in 60 patients, followed by pulmonary atresia in 12, and absent pulmonary valve in 4. The original TOF phenotype was unclear in 2. A central shunt had been placed in 22 patients. All patients had undergone TOF repair. Transannular patch repair was performed in 50 patients (13 with and 37 without SMVA, p<0.0001). Among the 60 patients (20 with and 40 without SMVA) who underwent PVR, the primary reason for PVR was severe regurgitation in 51, stenosis in 4 and mixed stenosis and regurgitation in 5. A PVR was performed surgically in 50 patients, percutaneouly in 6 and surgical followed by percutaneous technique in 3.
Table 1 compares differences in the clinical and imaging characteristics of patients with and without SMVA as well as outlines the characteristics of MVP and SDML patients. Compared with those without SMVA, TOF+SMVA patients were more likely females (60.7% vs 33.9%, p=0.03), less likely to have transannular patch (52% vs 97.4%, p<0.0001) and had significantly lower RVEF on CMR (36.5% vs 43.8%, p=0.03). There were no significant differences in other variables, although there was a trend towards increased risk of atrial arrhythmias (44% vs 32.7%, p=0.5) and ventricular arrhythmias (32% vs 25.5%, p=0.6) among TOF+SMVA patients.
Baseline characteristics of adult Tetralogy of Fallot (TOF) patients with normal mitral valve and systolic mitral valve abnormality (SMVA), including those with mitral valve prolapse (MVP) and systolic displacement of mitral leaflets (SDML)
Echocardiographic and imaging data
The imaging characteristics of all patients groups are detailed in table 1. Among the 26 SMVA patients, mitral valve thickening was seen in 11. Anterior SMVA was present in 22, and bileaflet in 4. Two patients had moderate to severe MR requiring repair at the time of PVR. The rest had trace to mild regurgitation. Among those who underwent PVR, presurgical images were available in 24, postsurgical follow-up images in 19 and presurgical and postsurgical images were available in 15. The SMVA persisted on follow-up imaging in 12, resolved in 1 patient and 2 underwent mitral valve repair at the time of PVR for moderate to severe MR. Two patients also had tricuspid prolapse, one requiring repair. No haemodynamically significant aortic valve disorder was seen in any except for one SDML patient who had quadricuspid aortic valve requiring a Konno procedure and aortic valve replacement twice. The MVP patients had significantly larger LV end-systolic volume index (LVESVI) (25.3±7.9 vs 15.3±7.7 mL/m2, p=0.005) and decreased LVEF (58.3±8.7% vs 67.3±7.9%, p=0.01) when compared with those with SDML. No other significant clinical or echocardiographic differences were observed between the two groups.
Multivariate analysis
Multivariate logistic regression analysis revealed that the absence of transannular patch and atrial arrhythmias were independently associated with SMVA in TOF patients (table 2). Other variables including female gender, age of TOF repair, ventricular arrhythmias and RV size or function on echocardiogram was not independently associated with SMVA. Compared with those with RVEF >35%, the odd of SMVA among those with RVEF≤35% on CMR was 2.3 (p=0.018).
Multivariate logistic regression analysis of clinical characteristics associated with systolic mitral valve abnormality
Discussion
We report the first cohort of patients with a unique combination of SMVA and TOF described in the literature. To the best of our knowledge, the only other time this association was reported was in an unrepaired TOF patient aged 74 years in whom MVP was identified on autopsy.25 We found a strikingly higher prevalence of SMVA in adult TOF patients (total 8%; 4.6% MVP; 3.4% SDML) compared with the reported MVP prevalence of 2–3% in the general population.2 Univariate predictors for SMVA in our cohort were female gender, absence of transannular patch and lower RVEF on CMR, with trend towards increased risk of atrial and ventricular arrhythmias. The absence of transannular patch and atrial arrhythmias was independently associated with SMVA and the odds of SMVA increased significantly among those with RVEF≤35% on CMR. Thus, with this series, we highlight an important association between two common and apparently distinct entities.
Owing to the milestone surgical successes in CHD management over the past few decades, most TOF patients now thrive well into their adult years, thus generating new challenges, the most crucial one being increasing prevalence of adult comorbidities. LV systolic dysfunction is found in 21% of adult TOF patients and is associated with shunt duration, RV dysfunction and arrhythmia.26 Thus, it is well known that TOF is not only a disease of outflow tract and right heart but also involves abnormalities affecting the left heart. Higher vigilance about other left-sided abnormalities could guide physicians managing these patients.
MVP and systolic displacement
After Levine and colleagues described the 3D anatomy of the mitral leaflets, stringent echocardiographic definition of MVP has been used to estimate its prevalence of 2–3% in the general population,2 ,18 and it is considered to be a clinically heterogeneous condition.1 We included patients with borderline degrees of displacement ≤2 mm beyond the long axis as having ‘minimal systolic displacement’ in order to take into account the possibility that in some instances, SDML may represent a mild form of expression as opposed to a physiological variant of leaflet position.27 Prior studies have shown that the spectrum of valvular abnormalities including SDML may represent, in the familial context, early disease expression in gene carriers, a stage of progression or the result of disease-modifying factors. In this study, given no significant difference in the RV volumes between MVP and SDML patients, the SDML group may not represent a physiological variant of leaflet position but in fact a true intrinsic abnormality of the mitral leaflets. Recognising early forms of MVP may be important, so that earlier interventions to reduce haemodynamic stresses on the mitral leaflets in genetically susceptible individuals may potentially prevent the progression of MVP and severe MR requiring surgery, although this premise remains to be tested. Since it is unknown whether early, non-diagnostic MVP morphologies progress within or outside the familial context and whether some risk factors more than others contribute to progression, we felt it was important to include these group of patients in determining the prevalence of SMVA.
Associations of MVP
Although MVP is usually an isolated defect, it has also been described in other conditions like connective tissue disorders such as Marfan, Loeys-Dietz syndrome, Ehlers-Danlos syndrome, etc,5–7 as well as observed in association with hypertrophic cardiomyopathy.8 It has been described in response to the geometrical changes of the heart, especially of the left atrium and ventricle secondary to the deformities of the thoracic spine.28 However, there is a lack of literature on a clear association of MVP with CHD. The increasing population of adults with CHD is facing new challenges of increased health resource utilisation and hospitalisations, possibly due to associated comorbidites.29 Thus, our observation of increased prevalence of SMVA in TOF patients generates some important discussions regarding the pathophysiological basis as well as clinical relevance of these coexistent conditions.
Possible pathophysiological explanations
The present study was largely aimed to determine the frequency of SMVA in adults with TOF; however, we postulate the following pathophysiological possibilities for this association.
Haemodynamic factors
MVP has been described in patients with small and geometrically distorted LV cavities, and is thought generally to exist merely as a consequence of reduced or abnormal ventricular dimensions, thus resulting in a physiological appearance of prolapse.8 ,30 Significantly increased RV volume due to severe PR in adult TOF patients can result in a small LV cavity that could lead to the similar appearance of physiological prolapse. However, the LV and RV dimensions on echocardiogram and CMR were measured to be within the normal range, as well as the per cent patients who underwent PVR and the age at which PVR was performed were not different between those with and without SMVA. This demonstrates that both the groups had similar haemodynamic burden for a similar period of time. Thus, dwarfing of the LV from an enlarged RV resulting in physiological prolapse was probably not the primary aetiology of SMVA in this study, although this cannot be entirely ruled out as a possible pathophysiology. In this study, TOF patients with SMVA were less likely to have transannular patch, independent of the age of their TOF repair or abnormality of RV size and function, and had significantly lower RVEF on CMR. The pathophysiological explanation of these findings is unclear, although some RV deformation resulting in poor RV function could contribute to the SMVA. Further, larger scale, preferably multicenter studies could be helpful to understand this better.
Molecular/developmental basis
Some clues to the association of MVP in TOF can be gleaned from our understanding of normal heart development. The heart begins in the mammalian embryo as a linear tube composed of myocardial and endocardial cells derived from two separate mesodermal populations.31 The valves and membranous septae that divide the postnatal heart into four chambers are derived from two regional swellings of the extracellular matrix, known as endocardial cushions.32 Reciprocal signalling between the endocardial and myocardial cell layers in the cardiac cushion induces a transformation of the endothelial cells into interstitial or mesenchymal cells.33 Complex CHD like TOF frequently have variable expressivity attributable to multiple gene mutations in key transcription factors like Bone morphogenetic protein (BMP), GATA-4, SMAD, transforming growth factor, etc, required for compartmentalisation and proper communication between the four chambers. Several signalling and transcriptional pathways have been shown to play pivotal roles in the formation of the heart valves and some specifically in clinical MVP specimens, including Wnt/β-catenin signalling, the homeobox gene Sox4, SMAD6, BMP, etc.34–36 There is significant overlap in the molecular mechanisms that lead to the formation of valves and outflow tract abnormalities, and mutations in any of these might result in TOF and SMVA in the same patient.
Multifactorial
A combination of the above factors including haemodynamic changes in patients with genetic predisposition to MVP may be responsible for development of SMVA in some of the TOF patients. Overall, our findings suggest that the coexistence of TOF+SMVA is less likely due to the haemodynamic consequences of dilated RV and small LV, although the contribution of RV dysfunction seems plausible. At least in some patients, it may reflect the coexistence of two separate but primary disease entities versus a common genetic or embryological linkage.
Clinical relevance
It is unclear whether there is a synergistic effect that hastens the potential for adverse clinical outcomes in patients with TOF+SMVA. However, the known adverse sequelae associated with these entities individually including RV enlargement and dysfunction, PR, heart failure, arrhythmias, thromboembolic events, reoperation and sudden death mandate careful surveillance.37 Indeed, in our series, 44% patients with TOF+SMVA had history of atrial arrhythmia, 32% had ventricular arrhythmia and 21% required a pacemaker or ICD. This arrhythmia could not be explained solely on the basis of mitral abnormality since only 2 of 17 patients with prolapse had severe insufficiency requiring surgery. Furthermore, the arrhythmia prevalence in the TOF+SMVA group was higher than those without SMVA and greatly exceeded that previously reported for adults with TOF.38 In fact, atrial arrhythmia was independently associated with SMVA, suggesting the need for increased vigilance to look for SMVA in the presence of atrial arrhythmias or vice-versa in TOF patients. Moreover, TOF+SMVA patients had significantly poor RVEF on CMR.
Limitations
The higher prevalence of SMVA in TOF patients in this study could be reflective of the tertiary centre referral bias as well as the retrospective nature of the study. Also given the fact that all the echocardiograms were reviewed retrospectively, a detailed evaluation of the mitral valve morphology was not available for most of the patients. Thus, larger multicentre studies are needed to identify the true incidence of this association in the population and to help understand the basis for their correlation. Since we were unable to obtain all the echocardiograms of our patients since birth, the approximate timing of development of the SMVA could not be determined.
Conclusions
In this series of patients, we describe a novel association of SMVA in TOF patients with a prevalence of 8%. In clinical practice, this could be considered as infrequent and an incidental finding. The present findings emphasise the need to recognise this association and underscore that SMVA in TOF patients might serve as a marker of increased risks of arrhythmias and reoperation. Collaborative efforts across institutions are needed to study a large TOF population to understand their genetic and pathophysiological correlations of the associations, so that we can better define its clinical course and the optimum management strategies.
References
Footnotes
Contributors AA, ISH and EF were involved in the study conception and design. AA, ISH and EF were involved in echocardiographic image interpretation. AA, ISH, EF and VSM were involved in the results interpretation. AA drafted the article, while ISH, EF and VSM were involved in the critical revisions of the paper. All the authors approved the final manuscript.
Competing interests None declared.
Ethics approval Institutional Review Board at University of California San Francisco.
Provenance and peer review Not commissioned; internally peer reviewed.
Data sharing statement No additional data are available.