Article Text

Abstract
Objective In adults with an interarterial and intramural course of an anomalous right coronary artery from the left sinus (AAORCA), surgical unroofing is recommended in the setting of myocardial ischaemia. However, data regarding functional testing are limited, and the management of adults without ischaemia is unclear. To evaluate these patients, we employed an exercise N13-ammonia positron emission tomography (PET) protocol. We hypothesised that patients with typical angina and exertional dyspnoea would be more likely to have ischaemia and that patients without ischaemia could be managed conservatively.
Methods Between July 2008 and December 2014, we retrospectively identified 27 consecutive patients >18 years old with an interarterial and intramural course of an AAORCA who had exercise N13-ammonia PET.
Results The majority of patients had anatomic delineation with cardiac CT (25, 93%), and most patients had chest pain (24, 89%). Myocardial ischaemia with PET was common (13, 48%), and ischaemia was more likely in patients with typical angina and exertional dyspnoea (p<0.05). Surgery was performed in 12 patients including 11 patients with ischaemia. At a median follow-up of 245 days, there were no deaths in patients with surgery or in patients managed conservatively.
Conclusions In patients with an interarterial and intramural course of an AAORCA, typical angina and exertional dyspnoea are associated with ischaemia on exercise N13-ammonia PET. Referral for surgical unroofing in symptomatic patients with ischaemia on exercise N13-ammonia PET and initial conservative management in patients without ischaemia seems appropriate, though larger studies with long-term follow-up are needed.
- CONGENITAL HEART DISEASE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Current guidelines endorse revascularisation for an anomalous right coronary artery with an interarterial and intramural course in the setting of ischaemia. However, the best method to assess for ischaemia, as well as the management of patients without ischaemia, is unknown.
What does this study add?
By using an exercise 13N-ammonia positron emission tomography (PET) protocol, we have demonstrated an association between typical angina and dyspnoea with myocardial ischaemia in patients with anomalous right coronary arteries. In the absence of myocardial ischaemia, conservative follow-up was without complication.
How might this impact on clinical practice?
In symptomatic adults, exercise 13N-ammonia PET can be used to detect perfusion defects related to intramural compression of an anomalous right coronary artery. Patients with ischaemia can be offered surgery to improve symptoms, and patients without ischaemia can be followed closely.
Introduction
An anomalous coronary artery from the opposite sinus of Valsalva (ACAOS) is a common congenital abnormality affecting between 0.1% and 1% of the population.1 ,2 This abnormality has no consequences in most people, though younger patients and patients with an interarterial anomalous left coronary artery from the right sinus are at increased risk for sudden cardiac death.3 ,4 However, an anomalous right coronary artery from the left aortic sinus (AAORCA) with an interarterial course is more common. Even though this abnormality is for the most part benign, AAORCA has been associated with sudden cardiac death, typically during or immediately after exercise.5 ,6 Therefore, despite limited data, surgical revascularisation is often recommended for patients with an interarterial course of an AAORCA and documented myocardial ischaemia.7
The management of patients with an AAORCA and no demonstrable ischaemia is more controversial.7 ,8 In part, this uncertainty stems from the limited sensitivity of functional testing in predicting the haemodynamic consequences of an AAORCA.9 ,10 Myocardial perfusion imaging (MPI) with positron emission tomography (PET) offers superior spatial resolution compared with standard single-photon emission CT (SPECT) imaging.11 In addition, patients with an AAORCA would be expected to have inferior wall ischaemia, an area prone to artefact with SPECT, especially without CT attenuation correction.
By performing cardiac PET with N13-ammonia, MPI can also be performed immediately after exercise,12 the at-risk period for patients with an AAORCA. In these patients, vasodilator stress may not be appropriate since the putative mechanism for ischaemia involves mechanical compression.2 Finally, previous investigations have typically focused on younger patients.13 In adults, optimal risk stratification and management is even less clear.
Given these uncertainties, we employed an exercise N13-ammonia protocol to risk stratify adults with an interarterial and intramural course of an AAORCA. We aimed to demonstrate that adults with typical angina and exertional dyspnoea would be more likely to have myocardial ischaemia and may therefore benefit from surgical unroofing. We also hypothesised that adults without myocardial ischaemia could be managed conservatively.
Methods
Study population and definitions
From the cardiac PET database at the Cleveland Clinic, we retrospectively identified 27 consecutive patients who were ≥18 years old and had exercise N13-ammonia PET between July 2008 and December 2014 to evaluate an AAORCA with an interarterial and intramural course. At the time of stress testing, patient demographics, symptoms, comorbidities and medications were prospectively entered into a stress database. These data were verified with review of the electronic health record, and manual extraction of data was also performed.
Typical angina was defined as substernal chest discomfort provoked by stress or exertion and relieved with rest or nitroglycerin. Atypical angina was defined when two of these three characteristics were present, and non-anginal chest pain was defined when only one of these three characteristics was present. Exertional dyspnoea was defined as New York Heart Association class I and was assessed by standard criteria.14 Atherosclerotic coronary artery disease (CAD) was defined as a previous myocardial infarction, previous percutaneous intervention, a history of coronary artery bypass grafting or a >50% angiographic stenosis in a non-anomalous epicardial coronary artery. Hypertension was defined as self-reported history or use of antihypertensive medications. Hyperlipidaemia was defined as an abnormal fasting lipid panel according to adult treatment panel (ATP) III guidelines, self-reported history or use of lipid-lowering medications. Diabetes mellitus was defined as fasting blood glucose ≥126 mg/dL, self-reported history or use of glucose-lowering medications.
The anatomic delineation of the anomalous coronary artery was determined by cardiac CT angiography (CTA; n=25), cardiac MRI (n=1) or invasive coronary angiography with intravascular ultrasound (IVUS; n=1). An interarterial course was defined as a proximal course between the aorta and pulmonary trunk. An intramural course was defined by an acute angulation of the coronary origin from the aorta in conjunction with a narrow, ‘slit-like’ proximal cross-sectional area.
Stress testing and image acquisition
Patients had symptom-limited treadmill testing using a protocol designed to have the patient reach maximal exertion within 8–12 min.15 Heart rate targets were not used as an end point or to assess the adequacy of the test. The ST segment was measured 80 ms after the J point, and the magnitude of ST depression was recorded as the greatest horizontal or downsloping ST segment depression in any lead except aVR during the test or recovery. Peak estimated metabolic equivalents of task (METs) were calculated from treadmill speed and grade at peak exercise. Patients did not receive a walking recovery and were immediately placed supine for imaging.
MPI was performed with gated PET N13-ammonia images acquired on a hybrid PET/CT scanner (Siemens Biograph 40, Munich, Germany) with lutetium oxyorthosilicate crystals in a three-dimensional (3D) mode without septa. The nominal transaxial/axial spatial resolutions were 4.4 mm/4.7 mm. Images at rest were taken following intravenous injection of low-dose (6–8 mCi) N13-ammonia. Within 1 min of peak exercise, the patient was injected again with high-dose N13-ammonia (12–18 mCi), and gated stress tomographic imaging was performed. Depending on exercise duration, stress imaging was typically obtained between 30 and 40 min after resting imaging.
Data for attenuation correction were acquired with a low-dose CT protocol (120 kVp, 12 mAs, 0.3 mSv dose per scan) using a breath hold at normal end expiration. A CT scan was acquired immediately before the rest and stress PET scans. Data were reconstructed (3D ordered subset expectation maximisation algorithm) as static images (4 iterations, 8 subsets, 8 mm Gaussian filter) and as gated images (2 iterations, 8 subsets, 12 mm Gaussian filter). PET images were reoriented along the standard cardiac axes and displayed with INVIA Corridor 4DM software (Ann Arbor, Michigan, USA). Left ventricular volumes and ejection fraction were automatically computed from both rest and stress images.
A 17-segment model of the left ventricle was used to semiquantitatively score rest and stress images.16 The summed stress score (SSS) and summed rest score (SRS) were obtained by adding the scores on respective images. The summed difference score (SDS) was calculated by subtracting the SRS from the SSS. The percentage of ischaemic myocardium was calculated as the SDS divided by 68.17 All tests were reviewed by a nuclear medicine physician or cardiologist who was aware of patient data.
Outcomes
Patient management and follow-up was dichotomised according to the presence of myocardial ischaemia, defined as a SDS>0. Electronic health records were reviewed for additional information including the type of operation and postoperative complications. Administrative censoring was performed with follow-up determined from the time of stress testing to last known visit at the Cleveland Clinic. Our Institutional Review Board approved this study with a waiver of the requirement for informed consent.
Statistical analysis
Continuous variables are expressed as median (IQR), and categorical data are expressed as n (%). Intergroup comparisons were made with Wilcoxon rank-sum tests or Fisher's exact tests with Bayesian augmentation ((x+1)/(n+2)).18 All statistical analyses were performed with R (R CoreTeam 2016, http://www.R-project.org/). For all tests, a two-sided p<0.05 was considered statistically significant.
Results
Baseline characteristics and stress test results
The majority of our patients were middle-aged adults (46, 39–55 years), and the youngest patient was 24 years old (table 1). Chest pain was a presenting symptom in 24 patients (89%), and 12 (44%) reported typical angina. Exertional dyspnoea was common (16, 59%), and presyncope/syncope was also relatively frequent (8, 30%). There were no patients with a history of aborted sudden cardiac death. Regarding comorbidities, diabetes mellitus (3, 11%) and known atherosclerotic CAD (1, 4%) were uncommon. The sole patient with CAD had a coronary angiogram to evaluate atypical angina and was found to have a 50% stenosis in the mid left anterior descending artery and a 70% stenosis in an obtuse marginal branch. On exercise N13-ammonia PET, he had ischaemia only in the inferior wall, the territory subtended by the AAORCA. Regarding other cardiovascular risk factors, many patients had a history of hypertension (14, 52%) and hyperlipidaemia (14, 52%).
Baseline characteristics (n=27)
In general, patients had preserved exercise capacity (9.5 estimated METs, 8.0–11.0 estimate METs; table 2). Overall, 13 patients (48%) had ischaemia on PET MPI, and all patients had ischaemia in the territory of the right coronary artery (RCA). Chest pain during the exercise test was infrequent (5, 19%) as was ST depression (2, 7%). In these patients, two had ischaemia on MPI. Most patients with ischaemia had >5% ischaemic myocardium (10, 37%), and 6 patients had >10% ischaemic myocardium.
Exercise and MPI results (n=27)
Clinical associations with myocardial ischaemia
Patients with myocardial ischaemia on PET MPI were more likely to have typical angina and exertional dyspnoea (table 3). In this population, typical angina had a sensitivity of 77% and a specificity of 86% for myocardial ischaemia on PET MPI. Only three patients without a history of typical angina had ischaemia, and two of these patients reported exertional dyspnoea. Finally, men and older patients were more likely to have ischaemia, but these differences were not statistically significant.
Univariable associations with myocardial ischaemia on N13-ammonia PET
Patient management and outcomes
All patients had evidence of an interarterial and intramural course of the AAORCA. However, three patients had evidence of only a short intramural course, and two of these patients had myocardial ischaemia on PET with subsequent unroofing of the intramural segment (representative examples, figures 1⇓⇓–4). In patients with ischaemia on MPI, 11 of 13 had cardiac surgery (figure 5). The two patients managed conservatively had <5% ischaemic myocardium, and neither of these patients had typical angina. In the 14 patients without ischaemia on MPI, most were managed conservatively, though 1 patient did eventually have cardiac surgery for recurrent exertional symptoms.
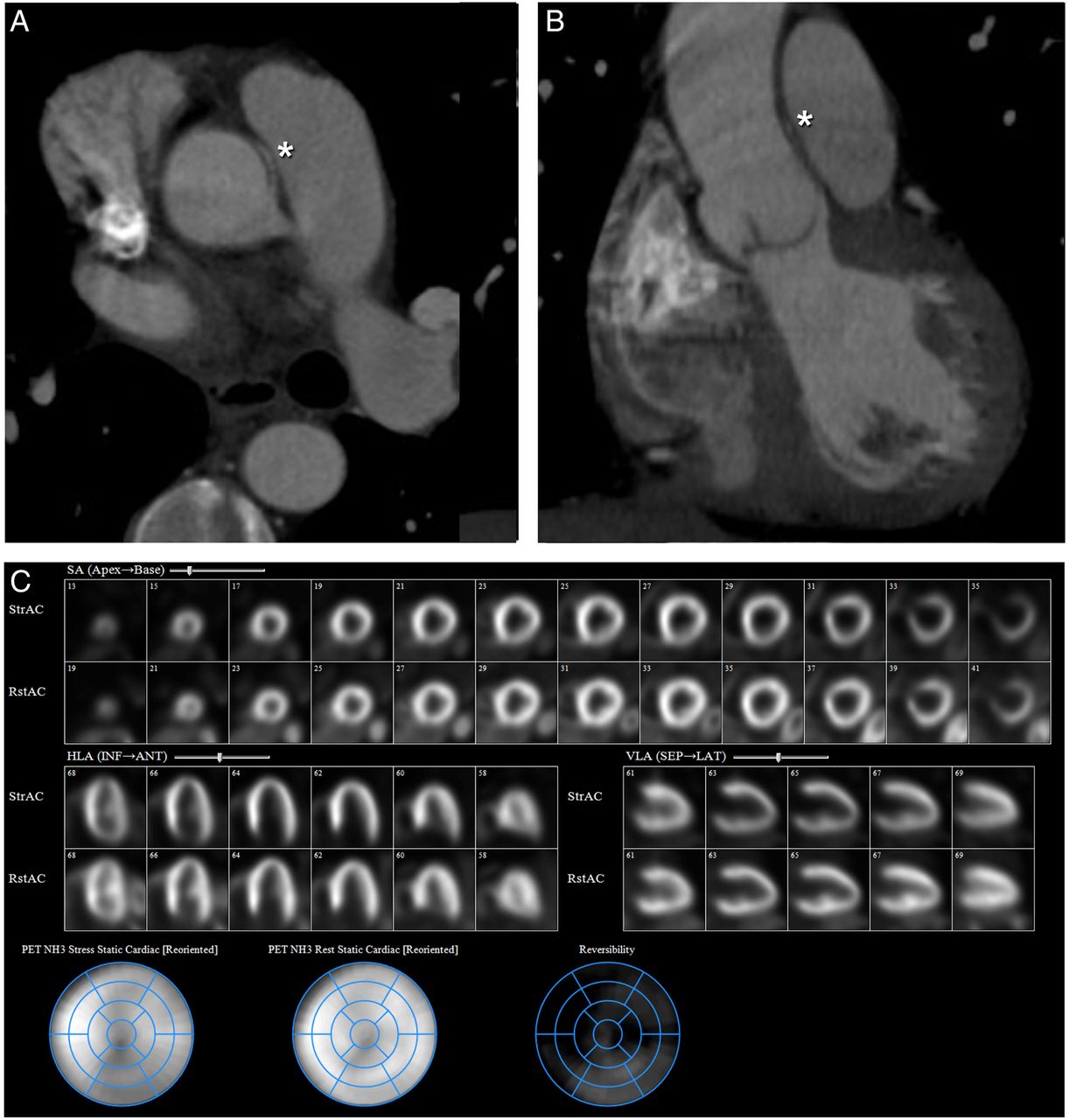
Intramural segment with moderate RCA territory ischaemia in a patient with an intramural course of an AAORCA that arises from the proximal tubular ascending aorta (A and B, asterix). There are reversible perfusion defects in the inferior segments (C). The patient had unroofing of the intramural artery. AAORCA, anomalous aortic origin of the right coronary artery; PET, positron emission tomography; RCA, right coronary artery.

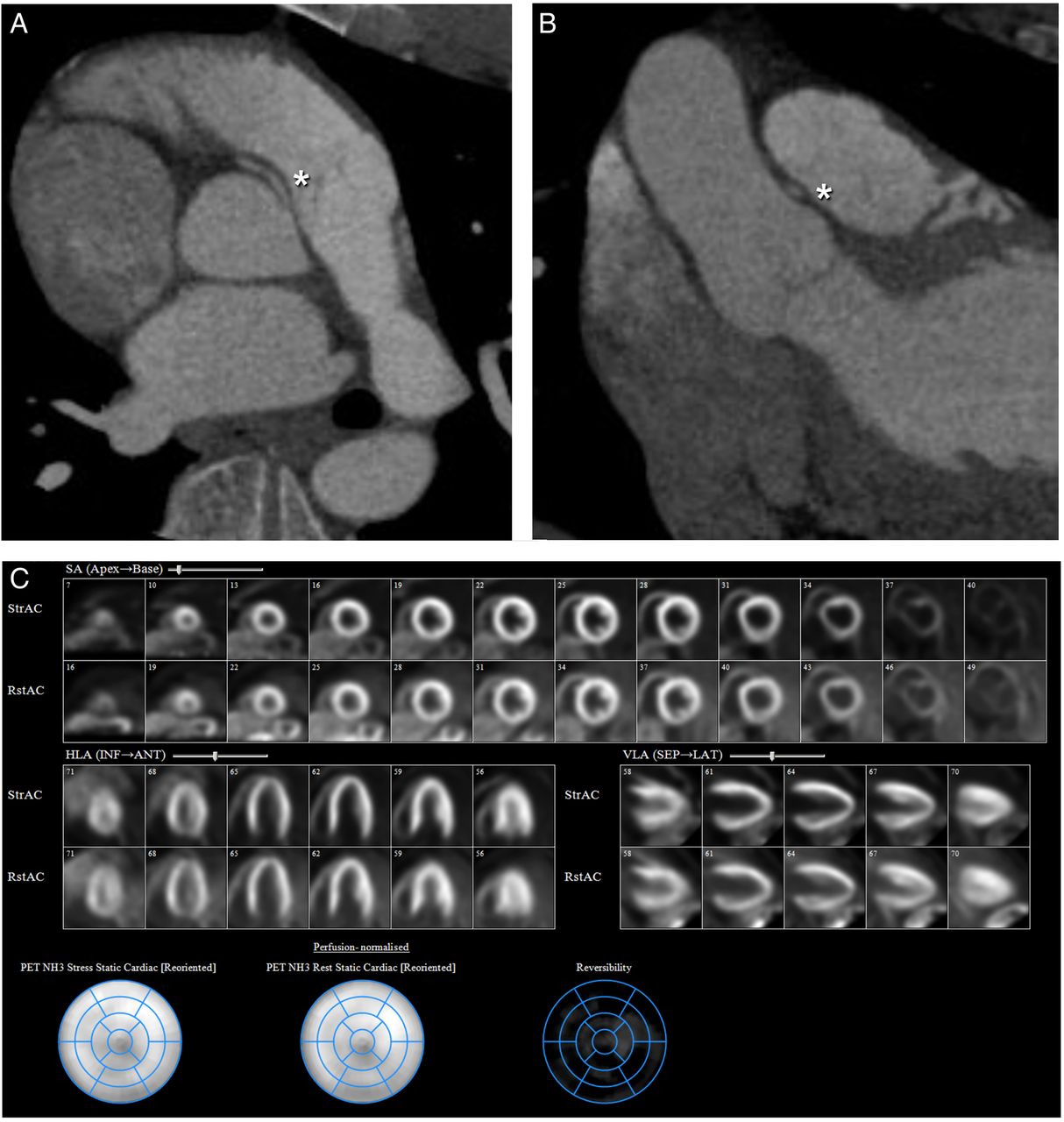
Short intramural segment with mild RCA territory ischaemia in a patient with a short intramural course of an AAORCA (A and B, asterix). There are reversible perfusion defects in the mid and distal inferior and distal septal segments (C). The patient had unroofing of the intramural artery. AAORCA, anomalous aortic origin of the right coronary artery; PET, positron emission tomography; RCA, right coronary artery.
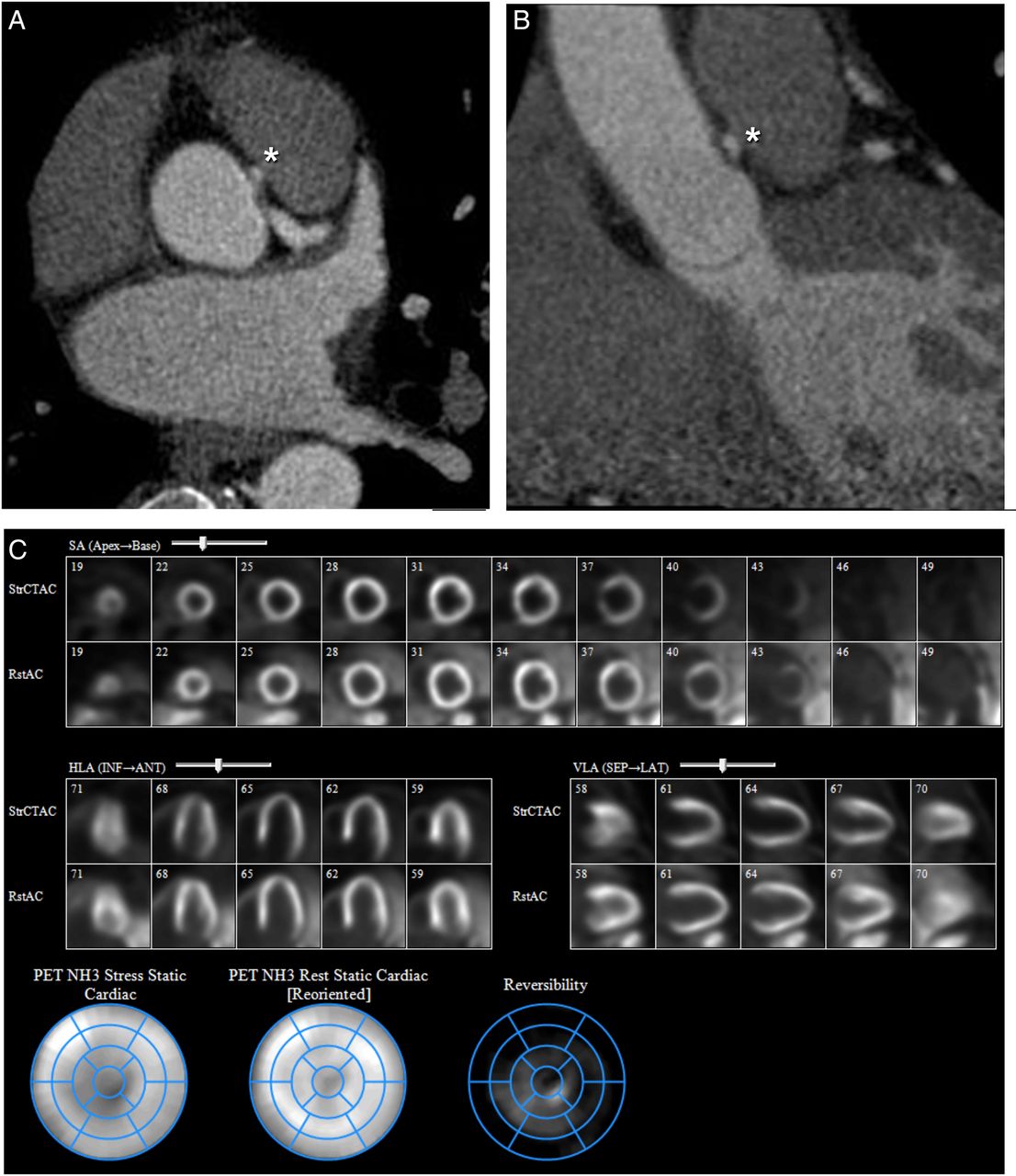
Intramural segment with no ischaemia in a patient with an intramural segment of an AAORCA (A and B, asterix), there is normal rest and stress perfusion (C). The patient has been managed conservatively. AAORCA, anomalous aortic origin of the right coronary artery; PET, positron emission tomography.

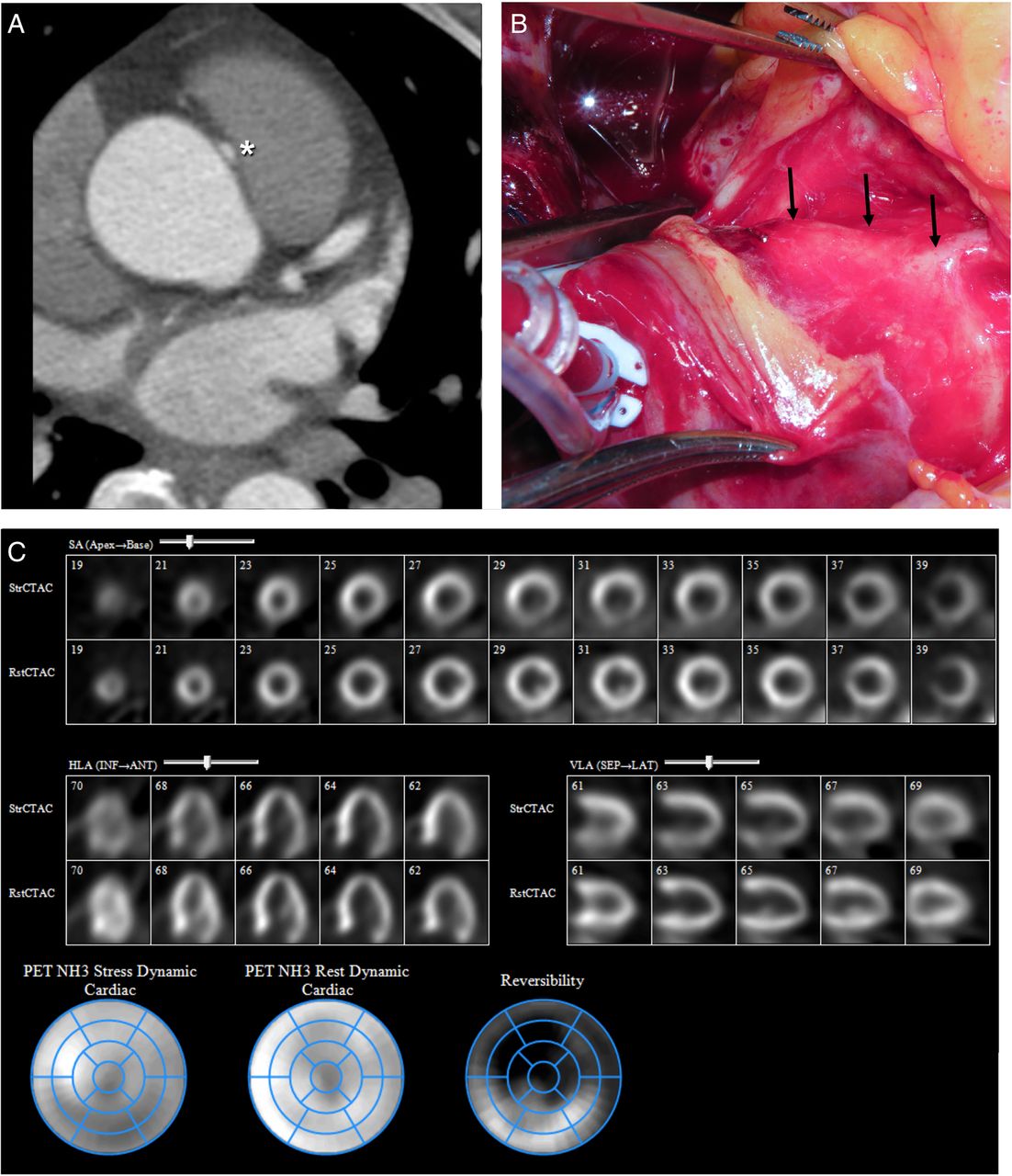
Surgical findings with an intramural segment and severe RCA territory ischaemia in a patient with an intramural segment of an AAORCA (A and B, asterix and arrows). There are reversible perfusion defects in the inferior, inferoseptum and inferolateral segments (A). The intramural artery was unroofed. AAORCA, anomalous aortic origin of the right coronary artery; PET, positron emission tomography; RCA, right coronary artery.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
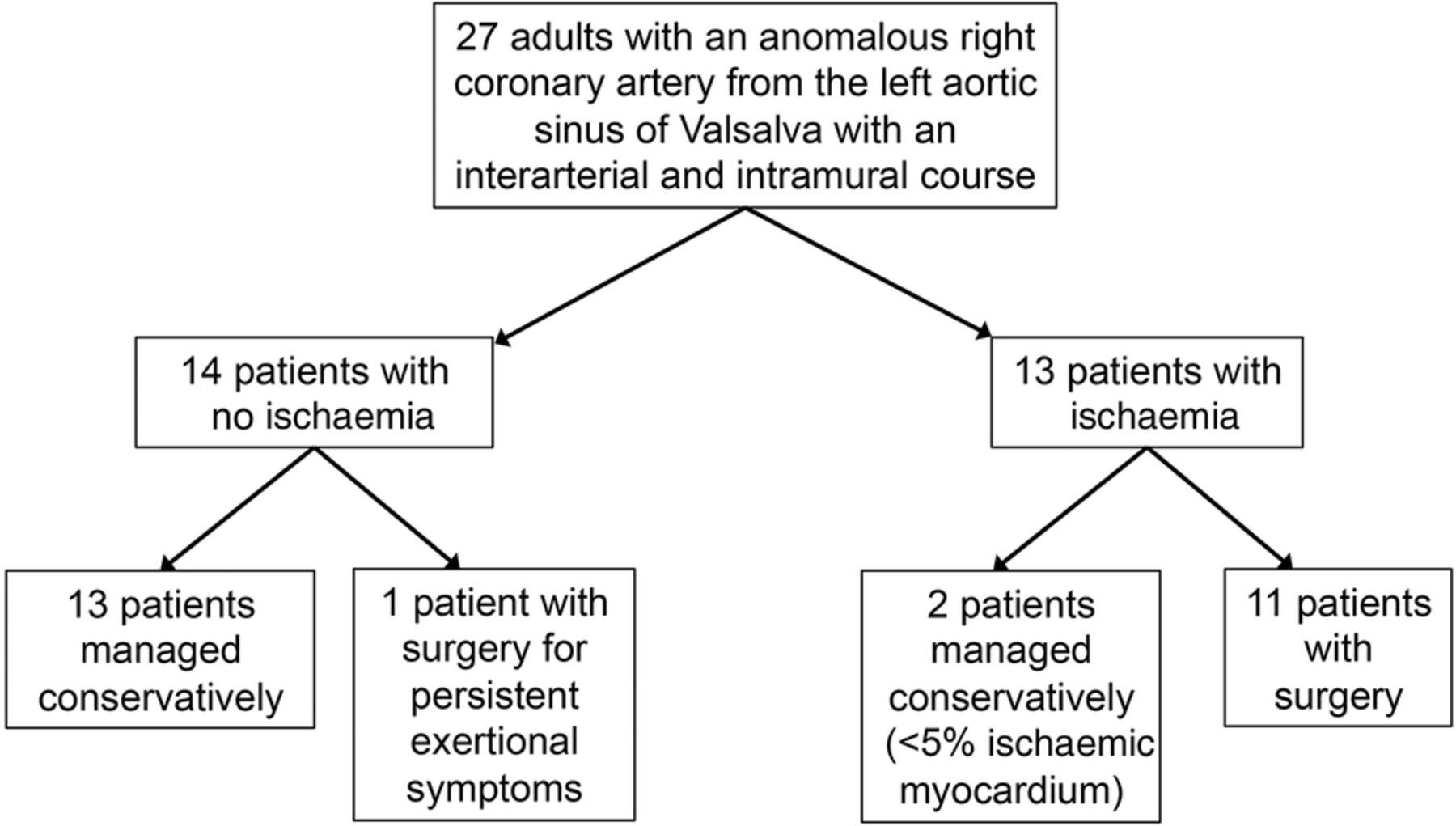
Flow diagram for patient management according to the presence of myocardial ischaemia on exercise N13-ammonia PET. PET, positron emission tomography.
Surgical unroofing of the intramural segment was performed in 11 patients, and 1 patient had reimplantation of the RCA. Surgery was safe with no perioperative deaths, and the median length of hospital stay was 5 days (4–9 days). Transient paroxysmal atrial fibrillation occurred in three patients. At postoperative follow-up, one patient had a moderate pericardial effusion that was managed conservatively and resolved.
At intermediate-term follow-up (245, 70–842 days), there have been no deaths in patients with or without surgery. In patients with conservative management, the duration of follow-up is similar to patients with surgery (median 352 vs 219 days, p=0.92).
Discussion
In adults with an interarterial and intramural course of an AAORCA, we have shown that an exercise N13-ammonia PET protocol is feasible. Patients with typical angina and exertional dyspnoea were more likely to have myocardial ischaemia. Surgery was safe with no perioperative deaths or deaths during follow-up. In patients without myocardial ischaemia, there have been no deaths with conservative management during intermediate-term follow-up.
Stress testing in patients with an AAORCA
Even though guidelines endorse an assessment for myocardial ischaemia in the risk stratification of patients with an AAORCA,7 the data to support this recommendation are limited, and the best method for a non-invasive functional assessment is unclear. In patients with an AAORCA, exercise treadmill testing appears to have limited sensitivity and is often unremarkable, even in the setting of serious cardiac symptoms or subsequent sudden cardiac death.5 ,19 ,20 In our patients, only 1 of 13 with ischaemia on MPI had ST depression with exercise.
The sensitivity of SPECT and stress echocardiography might also be inadequate. In our study, 21 patients had an exercise SPECT or echocardiogram within 6 months of their PET MPI. Only two of these patients demonstrated ischaemia, but both of these patients had normal PET MPI. In the 19 patients with negative exercise SPECT or echocardiogram, 8 had ischaemia on PET MPI. These observations are consistent with a recent study including 26 patients with an interarterial ACAOS: perfusion defects on SPECT were noted only in territories subtended by a coronary artery with obstructive CAD and were not related to the ACAOS.21
However, many of the patients in that study had vasodilator MPI.21 As noted, most adverse events and symptoms occur with exertion and may be related to haemodynamic compression of the intramural segment of the anomalous artery. A functional study with exercise may therefore be best in these patients. Finally, even though cardiac PET with N13-ammonia has been performed previously in adults12 and in paediatric patients with coronary abnormalities,22 to the best of our knowledge, our study is the first to assess for exercise-induced perfusion defects in adults with an AAORCA.
Considerations for the adult patient with an interarterial and intramural AAORCA
A major risk factor for sudden cardiac death is age at presentation with most adverse events occurring in patients under 30.3 ,4 Of note, in our cohort of adults, myocardial ischaemia was more common in older patients, though not statistically detectable. A putative mechanism for ischaemia in adult patients is related to exertional asymmetric compression of the intramural segment which may worsen as the aortic wall stiffens with age.23 Consequently, patients may not develop symptoms until middle age when the compliance of the aortic wall has decreased, though this hypothesis warrants further study.
Nonetheless, observational data suggest that older patients, especially those with an AAORCA, have a benign prognosis, and a survival advantage with surgery has not been demonstrated.24 In these patients, surgical unroofing is therefore performed to improve symptoms and seems best reserved for those with significant functional impairment related to myocardial ischaemia. Conversely, for most patients without myocardial ischaemia, even when an intramural course is suggested on imaging, close conservative management may be appropriate. However, these patients should be followed for worsening symptoms.
Limitations
Our study has several limitations. First, this study is retrospective from a single-center and is subject to selection bias. Even though our study is the largest to date with functional testing in adults with an interarterial and intramural course of an AAORCA, multicentre investigations or a national registry are needed in these patients, similar to ongoing collaborative efforts in younger patients with an ACAOS.13 ,25 Second, because we injected patients while they were on the treadmill, we could not perform dynamic imaging with measurement of absolute myocardial blood flow. However, given the putative hypothesis that ischaemia develops from compression of the intramural segment, we assert that the response to exercise is clinically more important than measurement of blood flow after administration of a vasodilator. In addition, our follow-up was limited, though as we note, continued clinical assessment of these patients is essential. Finally, we were interested in non-invasive functional testing and did not evaluate invasive risk stratification, which has been successfully performed with IVUS.26 We speculate that similar information is obtained with CTA as with IVUS, though direct comparisons have not been performed.
Conclusion
In patients with an interarterial and intramural course of an AAORCA, exercise N13-ammonia PET is feasible, and myocardial ischaemia is more common in patients with typical angina and exertional dyspnoea. Surgical unroofing in this population was free from significant complications, and initial conservative management of patients without myocardial ischaemia seems reasonable.
References
Footnotes
Contributors PCC was involved in conception and design of analysis, interpretation of data, and drafting of manuscript. AM was involved in interpretation of data and drafting of manuscript. SK, PS, DM, RL, SDF, REH and GP were involved in interpretation of data and critical revision of manuscript. WAJ was involved in conception and design of analysis, interpretation of data, critical revision of manuscript, and is the corresponding author.
Competing interests None declared.
Ethics approval Institutional Review Board at the Cleveland Clinic.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.