Article Text

Abstract
Objectives This study aimed to determine the prevalence of physical inactivity and perceived barriers to physical activity among individuals with hypertrophic cardiomyopathy (HCM), and to determine potential demographic, clinical and health-related factors influencing likelihood of meeting physical activity guidelines.
Methods This was a cross-sectional study of consecutive patients (n=198) with HCM attending a specialist HCM centre from July 2014 to November 2015. The primary outcome measure was physical activity (minutes per day), as measured by self-report (International Physical Activity Questionnaire (IPAQ)) and objective means (ActiGraph accelerometer). For both, participants were classified as meeting guidelines if they did at least 150 min per week of physical activity. Quality of life (Short Form-36 V.2, SF-36v2), barriers to exercise and clinical–demographic data were also collected.
Results In total, 54.8% of participants did not meet physical activity recommendations based on IPAQ, and 12.7% did not meet guidelines based on accelerometer data. The most commonly identified barriers to exercise were ‘pain interferes with my exercise’ (33%) and ‘I have an injury/disability that stops me’ (29%). Independent factors associated with meeting guidelines included older age (OR 0.66, 95% CI 0.51 to 0.85, p=0.002), higher education level (OR 2.31, 95% CI 1.08 to 4.93, p=0.03), better physical quality of life (OR 1.05, 95% CI 1.0 to 1.09, p=0.05) and more reported barriers (OR 0.71, 95% CI 0.56 to 0.91, p=0.01).
Conclusions More than half of the patients with HCM did not meet minimum physical activity recommendations. Several barriers to exercise among individuals with HCM exist, and provide the basis for targeted interventions to promote physical activity and improve overall health in patients with HCM.
- Physical Activity
- exercise
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Very little is known about the physical activity behaviours of individuals with hypertrophic cardiomyopathy (HCM), and the barriers which prevent them from doing sufficient physical activity.
What does this study add?
This study shows that many individuals with HCM engage in insufficient physical activity, and that there are particular barriers that should be addressed so that these individuals may also experience the benefits of regular physical activity.
How might this impact on clinical practice?
Individuals with HCM may be susceptible to low physical activity levels. Physical activity is vital for improving health and well-being for all individuals. For those with HCM, physical activity should be encouraged with an emphasis on what individuals can and should do, rather than the small number of activities that are not recommended. Personalised physical activity recommendations, taking into account clinical circumstances and identification of individual barriers, will ultimately improve the specialised care of patients with HCM.
Introduction
Hypertrophic cardiomyopathy (HCM) is a genetic heart disease with the hallmark feature of left ventricular hypertrophy, which confers an increased risk of arrhythmias and sudden cardiac death.1 HCM is the most common genetic heart disease with a prevalence of up to 1:200 in the general population.2 HCM is inherited as an autosomal dominant trait, with a 1 in 2 (50%) inheritance risk to children.1 Consensus guidelines recommend restricting individuals with HCM from participating in physical activity of high-intensity and/or a competitive nature,3 ,4 due to the increased risk of sudden cardiac arrest and death.5 Recommendations state that patients with a genetic cardiovascular disease, such as HCM, can safely participate in activities of a low-to-moderate intensity; however, no guidance is given as to the recommended amount of physical activity to be undertaken.3 With the focus often on what activities individuals with HCM should avoid, the need to undertake an appropriate level of physical activity may not be effectively communicated by clinicians, potentially leading to inactivity and associated poor general health.6
Physical activity has numerous health benefits, including prevention of non-communicable diseases such as type 2 diabetes and cardiovascular disease, improvement in mental health and well-being, and reductions in risk of developing certain cancers and all-cause mortality.7–9 Physical inactivity is associated with poor health outcomes, and is now the fourth leading cause of death worldwide.10 In order to combat high rates of physical inactivity, physical activity guidelines for adults (aged 18–64 years) have been developed in many countries, which generally recommend being active on most (if not all) days of the week and accumulating 150–300 min of moderate-intensity physical activity or 75–150 min of vigorous activity per week (or a combination of both).11–13 Moderate activities include cycling, slow jogging, doubles tennis and brisk walking.3 Individuals with HCM report a reduction in physical activity following diagnosis,14 and are known to report poor physical health-related quality of life.15 Little is known about the reasons for this reduction.
We hypothesised that individuals with HCM fail to undertake sufficient levels of physical activity, and therefore do not meet the minimum guideline recommendations. This study sought to establish the prevalence of physical inactivity in a HCM cohort, to elucidate the barriers to physical activity in this population and to determine potential demographic, clinical and health-related factors influencing the likelihood of meeting physical activity guidelines.
Methods
Study design and participants
From July 2014 to November 2015, individuals with a definite clinical diagnosis of HCM were recruited consecutively from the Hypertrophic Cardiomyopathy Clinic at Royal Prince Alfred Hospital, Sydney, Australia. Eligibility included a diagnosis prior to recruitment (ie, those with a new diagnosis were excluded), aged 18 years or older, not pregnant and with sufficient language skills to complete the survey in English. Diagnosis of HCM was made primarily based on presence of left ventricular hypertrophy on echocardiogram of 15 mm or greater (13–14 mm is considered borderline) in combination with ECG abnormalities and archetypal clinical features such as an apical systolic murmur.16
Individuals were invited to complete a written survey. A subgroup of participants attending the clinic consecutively from March 2015 to November 2015 were asked to also wear an accelerometer for a minimum of 7 days. The survey-only participants completed the survey at the clinics, where possible, with some participants returning their survey by post. Those participating in the accelerometer substudy completed the survey after wearing the accelerometer. The Sydney Local Health District Ethics Review Committee approved the study, and all participants gave informed written consent.
Clinical and demographic information
Clinical data were obtained from patient medical records and included basic demographics: age, gender, education and postcode (from which Socio-Economic Indexes for Areas (SEIFA17) was determined); clinical information including severity of left ventricular hypertrophy, New York Heart Association (NYHA) functional class, existing comorbidities, family history of sudden cardiac death and body mass index (BMI), and treatments such as medications and implantable cardioverter defibrillator (ICD) therapy.
Survey assessments
International Physical Activity Questionnaire
The International Physical Activity Questionnaire (IPAQ) is a widely used and validated measure for assessing physical activity among adults.18 This study used the self-administered long form of the past 7 days recall version of the IPAQ, which assesses frequency and duration of walking, cycling, and other moderate-intensity and vigorous-intensity physical activity across four activity domains (work, transport, home, recreation). The IPAQ guidelines for data management (http://www.ipaq.ki.se) were followed. This study focused on self-reported time spent in leisure-time physical activity (LTPA) only. Participants were classified as meeting guidelines if they engaged in ≥150 min/week of walking or other moderate or vigorous physical activity (with duration of vigorous activity multiplied by two), or ≥75 min or more per week vigorous physical activity. This approach has been used previously to examine physical activity behaviours during leisure time, which are generally considered more discretionary than other domains of activity.19
Medical Outcomes Survey Short Form-36 V.2
Quality of life was evaluated using the Short Form-36 V.2 (SF-36v2),15 ,20 ,21 a commonly used measure of health-related quality of life that has been validated in Australian populations.22 The survey provides scores across eight domains of physical health and mental health, including physical functioning, role limitations due to physical health, bodily pain, general health, vitality, social functioning, role limitations due to emotional health and mental health. These scores are combined to provide an overall estimate for physical health (physical component score, PCS) and mental health (mental component score, MCS). The survey was scored using the QualityMetric Health Outcomes Scoring Software (V.4.5, Lincoln, Rhode Island, USA). The subdomain scores were compared with age-matched Australian population norms (45–54 years).23 Weighted t-scores—standardised as per Australian population norms—of physical (PCSAT) and mental (MCSAT) health were also obtained.24
Barriers to exercise
Participants were asked to select reasons they were not being physically active from a list of 24 potential barriers identified previously (see online supplementary appendix 1).25 ,26 The total number of barriers identified was determined in addition to the frequency at which individual barriers were identified.
supplementary data
Physical activity accelerometer substudy
A subgroup of HCM individuals were also asked to wear a hip-mounted ActiGraph GT3X+ accelerometer (Pensacola, Florida, USA) on an elastic belt during all waking hours except during water-based activities, such as showering or swimming, for a period of 7 days. The ActiGraph monitor records physical activity intensity (activity counts per minute) which can be converted to frequency and duration, and provides an objective measure of overall physical activity in contrast to the subjective domain-focused IPAQ survey. Acceleration data were sampled by a 12-bit analogue-to-digital converter at a rate of 30 Hz, and stored in non-volatile flash memory.27
On receipt of the monitors, the data were downloaded and processed in 60 s epochs using the ActiLife software (V.6.11.5). A valid day was defined as a minimum of 10 hours recorded data (wear time), which excludes times during which the monitor recorded at least 60 consecutive minutes of zero counts/minute (periods of ‘non-wear’).28 To be included in the analyses, participants needed to have a minimum of 3 days of valid wear time.29 ,30 There was no significant difference in amount of moderate–vigorous physical activity performed on weekend and weekdays (mean weekend day=35.6 min/day, mean weekday=41.0 min/day, p=0.11); therefore, no restriction on the minimum number of weekend or weekdays was imposed in the criteria for inclusion in the analysis. Age-specific cut points that are commonly used in adult populations were selected to determine the time (minutes) spent in light-intensity (100–2020 counts/minute), moderate-intensity (2021–5999 counts/minute) and vigorous-intensity (≥6000 counts/minute) physical activity.31 Moderate–vigorous physical activity was calculated by summing time spent in moderate physical activity and vigorous physical activity. The durations of bouts of activity at ≥2020 counts/minute (ie, at least moderate activity) that spanned at least 10 consecutive minutes were also computed and summed as a measure of physical activity accumulated in sustained bouts.
Proportions of participants meeting the guideline recommendations of 150 min or more moderate–vigorous physical activity per week in sustained bouts of 10 min or more were calculated. For individuals with <7 days valid wear, the total physical activity in bouts of 10 min was calculated by dividing the minutes per day of physical activity (in bouts of 10 min or more) by the number of valid days, and multiplying by seven to obtain the estimated average per week.
Statistical analysis
Data were analysed using Stata V.14.1 (StataCorp). Descriptive statistics were used to examine sociodemographic and clinical characteristics, physical activity (at different intensities) for IPAQ and accelerometer data, mental and physical health scores, and to determine the most frequently identified barriers to exercise. Participants who completed the accelerometer study were compared with those who completed the survey only using χ2, t-tests or Mann-Whitney tests, as appropriate, to ensure that there were no significant differences between the two groups.
Logistic regression was used to identify factors associated with meeting physical activity guidelines based on IPAQ data (since these data were available for the whole sample). Age was divided by 10 to demonstrate the impact of a 10-year increase in age, rather than a single year increase. Significance was set at p≤0.05, corresponding to a 95% CI. Univariate analyses were performed to examine factors associated with the likelihood of participants meeting guidelines. Collinearity was tested through calculation of variance inflation factors (VIFs) between variables with p<0.1. All VIFs were <2; therefore, no variables required exclusion. Variables associated with meeting guidelines at p<0.1 in the univariate analysis were included in a multivariate model, with a stepwise backwards regression undertaken until only significant variables remained. The Bayesian Information Criterion (BIC) was calculated as a guide of model fit.
The individual barriers to exercise were assessed in separate analyses using the same principles outlined above.
Results
Cohort characteristics
A total of 264 individuals with HCM were seen at the clinics during the study period. Of these, 34 (12.9%) were excluded due to insufficient knowledge of English (n=17), genotype-positive phenotype-negative (n=7) and other reasons (eg, pregnancy, incorrect previous diagnosis; n=10). Of the 230 remaining eligible participants, 8 declined to participate, 23 withdrew from the study, and one accelerometer and survey was lost in the post leaving a total cohort of 198 individuals (figure 1). There were no significant age or gender differences between the study cohort and those who declined to participate or withdrew from the study.

Study recruitment flow chart. HCM, hypertrophic cardiomyopathy.
The characteristics of the final cohort of 198 HCM participants are shown in table 1, with comparison between the survey only (n=126) and accelerometer subset (n=72). A significant gender imbalance was observed between groups (57.1% male survey participants vs 73.6% male accelerometer participants, p=0.02). Additionally, a small difference in maximal wall thickness was observed between survey and accelerometer participants (p=0.04). The mean age was 48.8±15.3 years. In the total HCM cohort, 39.4% had an ICD in situ, 50.0% were on β-blocker medication, 60.1% had comorbidities and 24.0% were symptomatic based on the NYHA class (>1). Comorbidities included respiratory (eg, asthma and sleep apnoea), endocrine (eg, hyperthyroidism/hypothyroidism), cancer, muscular/skeletal (eg, arthritis, joint replacement) and mental health conditions. The most prevalent comorbidity was hypertension (n=41/196, 21%). Approximately a quarter (24.5%) had documented non-sustained ventricular tachycardia and 23% a history of syncope. A total of 32.8% had a history of obstructive disease with a mean maximum recorded gradient across the cohort of 40 mm Hg. Seventeen individuals had had a surgical intervention (alcohol septal ablation or myectomy) and atrial fibrillation was reported in 21.2% of patients. Sixty-seven per cent were classified as overweight or obese based on BMI, and 55.1% came from an area of high socioeconomic status (SEIFA decile >8), with 34.6% having tertiary education.
Clinical characteristics of study groups
Levels of physical activity
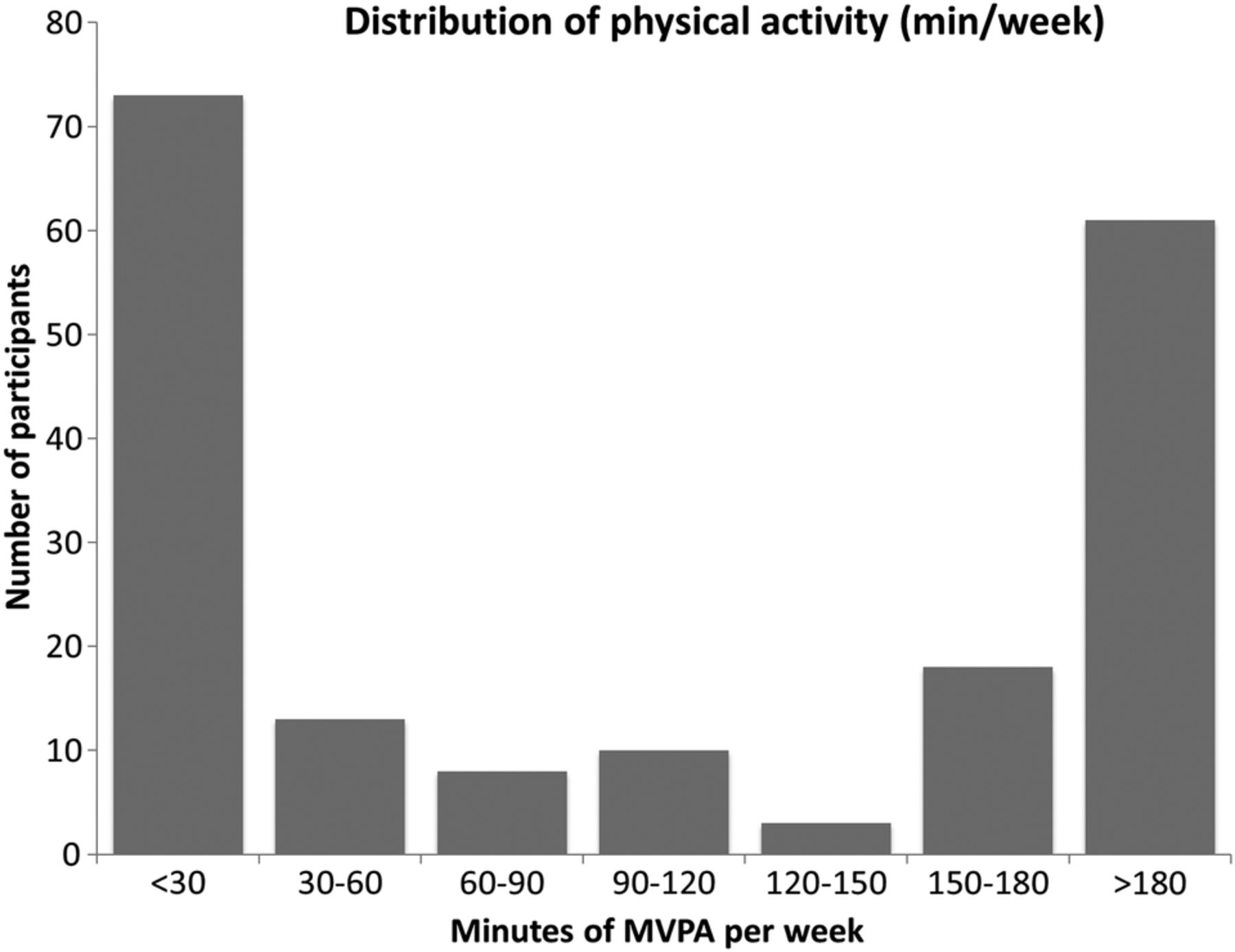
A total of 186 participants (93.9%) had complete IPAQ data for LTPA. The mean durations of activity at each intensity are shown in table 2. The total mean time spent in walking, moderate and vigorous LTPA was ∼3 hours/week. However, the median was 90.0 min/week, and only 45.2% of the cohort met the minimum Australian guidelines for physical activity with a bimodal distribution observed (figure 2).
Physical activity per week and proportion meeting guidelines
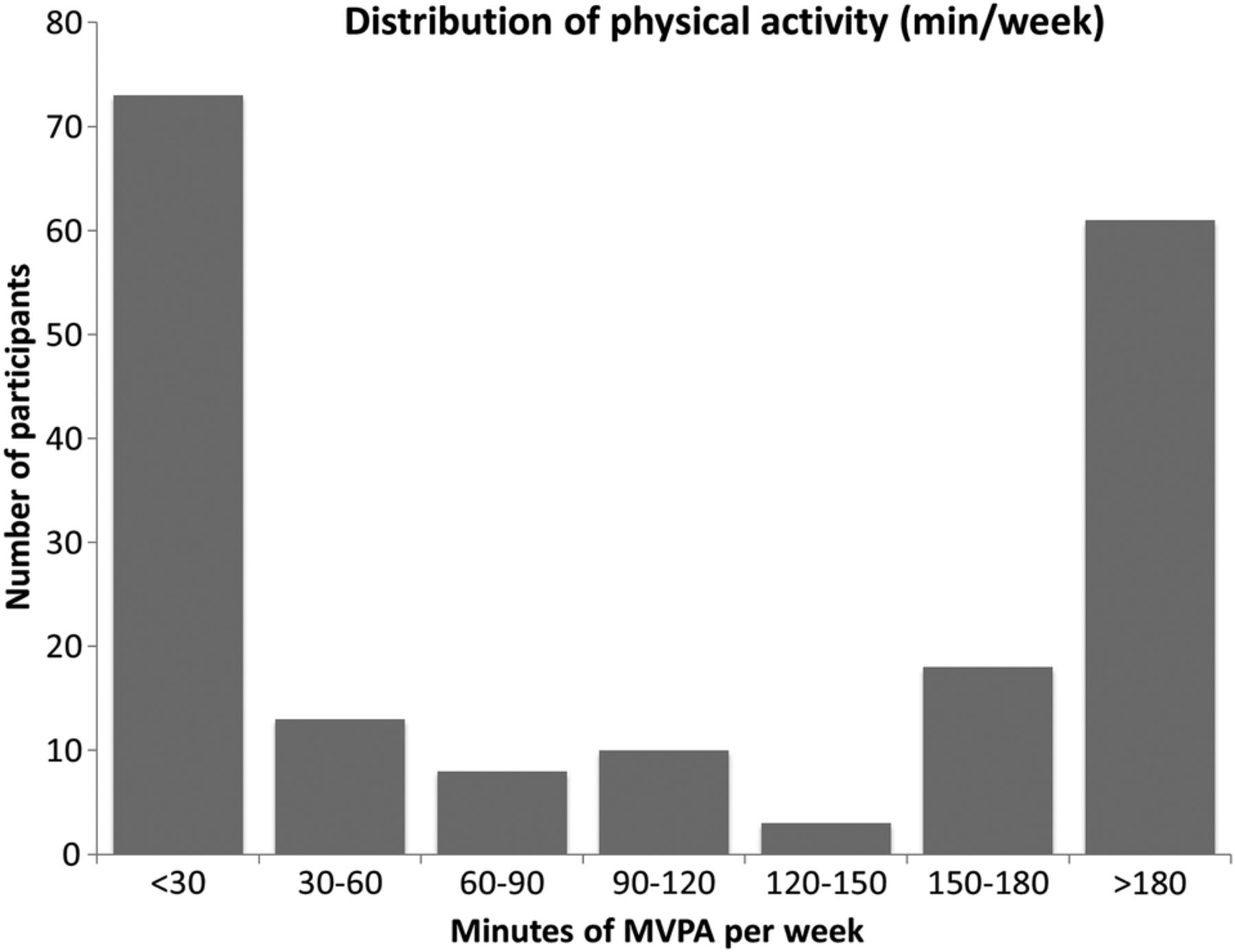
Distribution of physical activity (min/week) across 30 min increments. MVPA, moderate–vigorous physical activity.
Accelerometer data were obtained from 69 individuals, of whom 63 satisfied requirements for a minimum of 10 hours wear time on a minimum of 3 days. The minutes per week in each activity were higher according to accelerometry data than self-reported data, with a mean of 4.6 hours/week of accelerometer-assessed moderate–vigorous physical activity (table 2). When restricted to activity undertaken in bouts of 10 min or more, the mean moderate–vigorous physical activity was 55.5 min/week, and only 12.7% (n=8) performed a minimum 150 min/week (accrued in at least 10 min bouts) of moderate–vigorous physical activity. Supplementary analyses were conducted to rule out the possibility that the differences observed in the proportions meeting guidelines according to IPAQ and accelerometry data were attributable to differences between the samples. The proportions of these two groups who met guidelines according to the IPAQ were not significantly different (41.5% vs 47.1%, p=0.47). There was also no significant difference between mean minutes per week of LTPA between the accelerometer participants and survey-only participants based on self-report (169.4 vs 192.9 min, p=0.57).
Health-related quality of life (SF-36v2)
A total of 175 (88.4%) participants satisfactorily completed the SF-36v2. There were significant differences between the study cohort and age-matched Australian norms observed in all domains excepting bodily pain and social function (figure 3). The mean weighted t-scores for physical health (PCSAT) and mental health (MCSAT) were 45.9 (SD=10.6) and 45.6 (SD=13.4), respectively. Australian-weighted t-scores correspond to a population mean of 50 for the PCSAT and MCSAT, with the majority of individuals falling within 1SD of the mean (between 40 and 60). In the study cohort, 29.7% (n=52) of participants had a PCSAT<40 and 26.3% (n=46) of participants had a MCSAT <40.
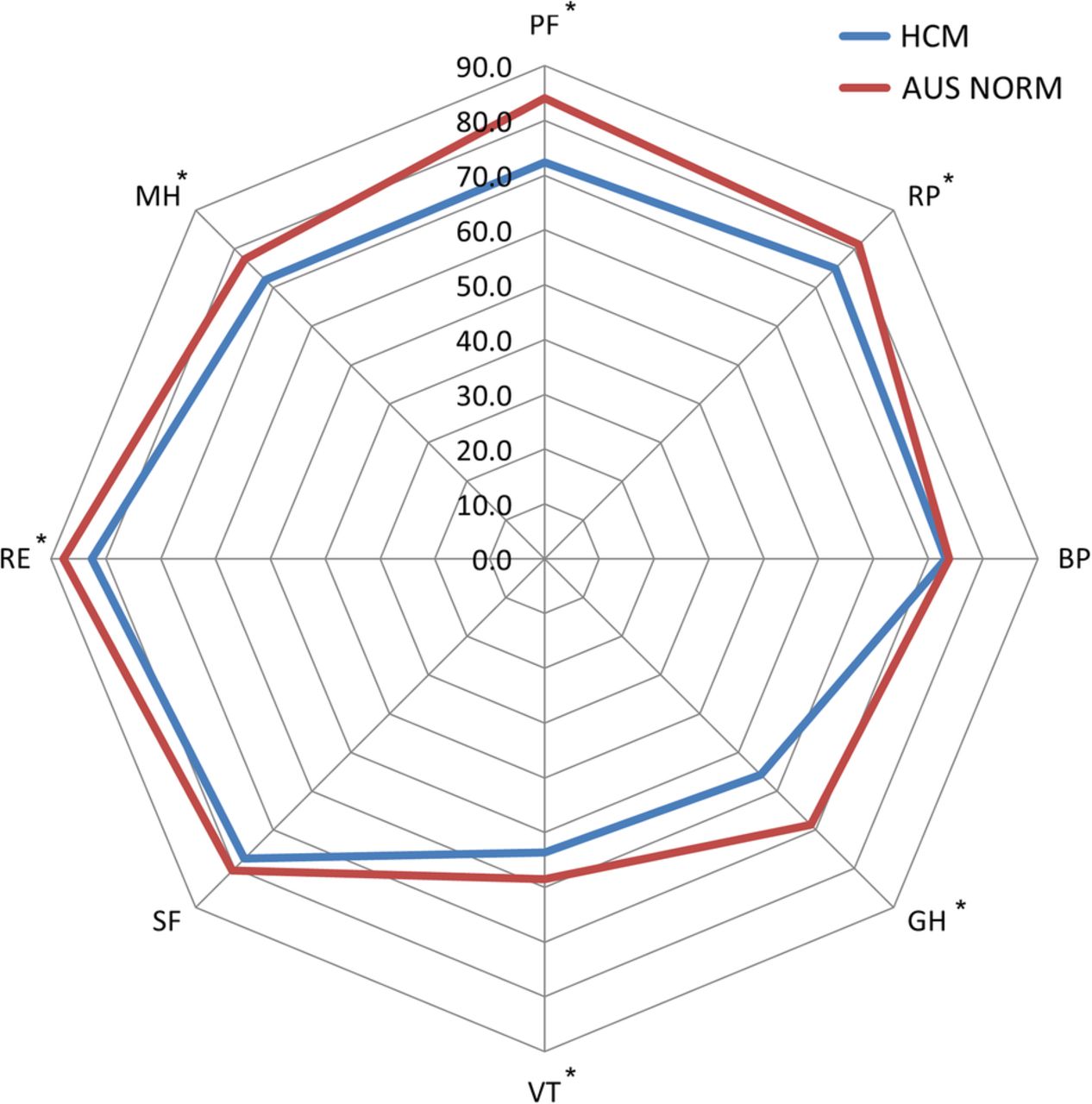
Spider plot of the unstandardised SF-36v2 subscales, comparing our HCM population with the mean for the general population (aged 45–54 years). Patients with HCM scored significantly lower than the age-matched general AUS population norms on the following subscales (marked with an asterisk); PF (p<0.001), RP (p=0.004), GH (p<0.001), VT (p=0.01), RE (p=0.01) and MH (p<0.001). BP and SF were non-significant. AUS, Australian; BP, bodily pain; GH, general health; HCM, hypertrophic cardiomyopathy; MH, mental health; PF, physical functioning; RE, role emotional; RP, role physical; SF, social function; SF-36v2, Short Form-36 V.2; VT, vitality. *p<0.05.
Barriers to exercise
The most commonly identified barriers to exercise included ‘pain interferes with my exercise’ (32.8%), ‘I have an injury/disability that stops me’ (29.3%) and ‘I don't have time’ (27.9%; figure 4). There were 32 individuals (16.2%) who indicated they had been advised not to exercise. The mean number of barriers identified was 2.6±2.0 with a range of 0–9 barriers, including 32 (16.2%) who identified 5 or more barriers to exercise and 78 (39.4%) identifying 1–2 barriers each.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Barriers to exercise identified by our HCM population. HCM, hypertrophic cardiomyopathy.
Factors and barriers associated with meeting physical activity guidelines
A number of factors were found to be associated with meeting guidelines in univariate analysis based on IPAQ data (table 3). In multivariate analysis, age (adjusted OR 0.66, 95% CI 0.51 to 0.85, p=0.002), education (adjusted OR 2.31, 95% CI 1.08 to 4.93, p=0.03), PCS (adjusted OR 1.05, 95% CI 1.0 to 1.09, p=0.05) and identifying a higher number of barriers (adjusted OR 0.71, 95% CI 0.56 to 0.91, p=0.01) were significantly and independently associated with meeting physical activity guidelines (table 3).
Factors associated with meeting physical activity guidelines
The sole barrier associated with a reduced likelihood of meeting physical activity guidelines, when adjusted for age, was poor health (adjusted OR 0.18, 95% CI 0.08 to 0.41, p=0.01; table 4).
Barriers associated with meeting physical activity guidelines
Discussion
When an individual is diagnosed with HCM, the recommendation is to avoid vigorous exercise and competitive sports due to the risk of sudden death. The response to these recommendations and how much physical activity patients with HCM subsequently perform is poorly understood. This study describes the physical activity levels of individuals with HCM. Overall, 54.8% of this cohort did not meet minimum guidelines for physical activity. Older age and a higher number of perceived barriers reduced the likelihood of meeting guidelines, while better physical health-related quality of life and having a tertiary education increased the likelihood of meeting guidelines. The most critical barriers to not meeting guidelines appeared to be health-related barriers such as ‘my health isn't good enough’ and ‘I have an injury or disability that stops me’. Such barriers may be particularly important for this population, and potentially provide a basis for targeted interventions to promote physical activity in individuals with HCM.
The physical health and mental health benefits of physical activity are well established; although studies specifically in HCM are limited, there may be benefits specific to the disease that are as yet unconfirmed.14 For example, preliminary studies in murine models of HCM have shown that physical activity can prevent development of fibrosis and reverse aspects of HCM, such as myocyte disarray.32 However, for individuals with HCM, participation in competitive and vigorous-intensity physical activity have historically been discouraged, with disease management guidelines offering varying levels of activity restrictions.3 ,4 This recommendation is based largely on expert consensus that high-level exercise may trigger arrhythmias and sudden death.5 Individuals with HCM are informed of this recommendation at diagnosis and many report an intentional decrease in physical activity following diagnosis.14 Although the need to undertake sufficient low-intensity to moderate-intensity physical activity is acknowledged in the consensus guidelines,3 individuals with HCM tend to focus only on what they should not do rather than on what they should, leading to a high prevalence of physical inactivity. In the present study, 32 participants reported that they had been advised not to exercise, potentially indicating poor communication regarding the importance of performing an appropriate level of physical activity while avoiding contraindicated activities.
In our current study, more than half did not meet the minimum physical activity guidelines. Although the IPAQ provides information across several domains, only LTPA was used in this study as self-report physical activity measures are known to have a propensity for overestimation, and time spent in physical activity during leisure time is indicative of healthy physical activity behaviours.19 Australian guidelines for physical activity recommend brisk walking as an appropriate way to achieve moderate physical activity; therefore, walking minutes were included in our analyses. The intensity of walking is not assessed by the IPAQ, and hence the proportion of the sample meeting guidelines may be an overestimate if some participants walked at a pace equivalent to less than moderate intensity. The proportion of individuals meeting physical activity guidelines based on IPAQ results was similar to the general Australian adult population (43%).33
Using an objective measure of physical activity, that is, accelerometry, we showed an elevated mean moderate–vigorous activity level compared with IPAQ results as it includes all activity across the whole week, not solely LTPA, and also includes activity not necessarily undertaken in bouts of at least 10 min. However, when total activity accumulated in bouts of 10 min or more was considered, that is, sustained physical activity, the mean (55.5 min/week moderate–vigorous physical activity) was well below the recommended 150 min, and 87.3% of the individuals were not sufficiently active.
Factors associated with a reduced likelihood of meeting guidelines (based on IPAQ data) included older age, lower education level (not tertiary) and identifying a higher number of barriers. In contrast to previous research indicating that individuals with a family history of sudden cardiac death or those with an ICD have a lower level of physical activity, these factors were not significantly associated with meeting guidelines in our study.14 ,34 In addition to the clinical factors, having a tertiary education was important, doubling the chances of meeting guidelines. This is consistent with previous studies, where low levels of education have been associated with lower physical activity levels.35 Better physical health-related or MH-related quality of life was associated with increased likelihood of meeting guidelines. However, consistent with previous studies of HCM populations,15 our results reveal lower physical and mental quality of life when compared with the normal Australian population. Given physical activity is known to improve quality of life,36 increasing physical activity in the HCM population may be an important factor in improving health-related quality of life among this patient group.
Compared with previous studies in the general Australian population, perceived barriers to exercise for individuals with HCM were more likely health-related rather than related to time or motivation. The most commonly identified barriers in our study were ‘pain interferes with my exercise’ and ‘I have an injury/disability that stops me’. In contrast, a study of physically inactive Australians showed the most commonly identified barriers were ‘I haven't got time’ and ‘I'm too lazy/not motivated/can't get started’. Having an injury/disability was the third most common barrier reported (pain was not listed as an option in this study).26 The HCM individuals who identified poor health as a barrier in our study were more likely to have a higher BMI, identify more barriers, have a higher NYHA class, report presence of comorbidities, be on β-blocker therapy, have worse physical health-related and MH-related quality of life, not be tertiary educated and live in an area of lower socioeconomic status (see online supplementary table S1). This suggests that these individuals truly have poorer health and that this is a substantial barrier to achieving adequate physical activity levels for this population.
In addition to health-related barriers, a number of individuals highlighted barriers related to everyday life, such as lack of time, and personal barriers such as being unmotivated, not enjoying physical activity or not feeling ‘sporty’. Although health-related concerns, such as disease symptoms (eg, breathlessness) or medication side effects (ie, from β-blockers), may be difficult to overcome, these other life and personal barriers may be more easily overcome with appropriate counselling and encouragement. These results identify a promising avenue for increasing physical activity in this population.
Study limitations
While we recruited consecutive patients attending a specialist HCM centre, the study was cross-sectional in nature and therefore precludes inferences about causality. Owing to the nature of the barriers survey, it was not possible to ascertain the details of the pain that people indicated interfered with their physical activity. It is feasible that individuals were referring to the potentially uncomfortable nature of undertaking moderate physical activity when not at a sufficient level of fitness, or may refer to pain induced by arthritis or other muscular–skeletal conditions.
Acknowledgments
The authors would like to acknowledge Gavin Abbott from Deakin University, Institute for Physical Activity and Nutrition, School of Exercise and Nutrition Sciences, for his assistance with data management.
References
Footnotes
Twitter Follow Chris Semsarian at @CSHeartResearch
Funding JS is the recipient of the Elizabeth and Henry Hamilton-Browne Scholarship from the University of Sydney. JI and AT are the recipients of National Heart Foundation of Australia Future Leader Fellowships (JI: #100833 and AT: #100046). KB is the recipient of an NHMRC Principal Research Fellowship (#1042442). CS is the recipient of an NHMRC Practitioner Fellowship (#571084).
Disclaimer The contents of this manuscript are the responsibility of the authors and do not reflect the views of the funding bodies.
Competing interests None declared.
Ethics approval IRB Sydney.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.