Article Text

Abstract
Objective Female sex is considered a risk factor for adverse outcomes following isolated coronary artery bypass graft (CABG) surgery. We assessed the association between sex and short-term mortality following isolated CABG, and estimated the ‘excess’ deaths occurring in women.
Methods Short-term mortality was investigated in 13 327 consecutive isolated CABG patients in North Texas between January 2008 and December 2012. The association between sex and CABG short-term mortality, and the excess deaths among women were assessed via a propensity-adjusted (by Society of Thoracic Surgeons-recognised risk factors) generalised estimating equations model approach.
Results Short-term mortality was significantly higher in women than men (adjusted OR=1.39; 95% CI 1.04 to 1.86; p=0.027). This significantly greater risk translates into 35 ‘excess’ deaths among women included in this study (>10% of the total 343 deaths in the study cohort) and into 392 ‘excess’ deaths among the ∼40 000 women undergoing isolated CABG in the USA each year.
Conclusions The higher risk associated with female sex lead to 35 ‘excess’ deaths in women in this study cohort (over 10% of the total deaths) and to 392 ‘excess’ deaths among women undergoing isolated CABG in the USA each year. Further research is needed to assess the causal mechanisms underlying this sex-related difference. Results of such work could inform the development and implementation of sex-specific treatment and management strategies to reduce women's mortality following CABG. Based on our results, if such work brought women's short-term mortality into line with men's, total short-term mortality could be reduced by up to 10%.
- QUALITY OF CARE AND OUTCOMES
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Previous studies comparing outcomes for men and women following coronary artery bypass graft (CABG) surgery show inconsistent and contradictory results, ranging from higher mortality among women, to a protective effect of female sex. Among those reporting higher mortality for women, inconsistent conclusions have been reached as to whether it stems from risks inherent to their sex or from worse preoperative risk profiles.
What does this study add?
This study provides evidence that female sex itself is associated with higher risk of mortality in CABG. Based on this higher risk, it estimates that an ‘excess’ 392 deaths occur among women undergoing isolated CABG in the USA each year.
How might this impact on clinical practice?
These results show that a meaningful number of women’s lives will be impacted by research aimed at uncovering the causes underlying their higher risk of CABG mortality and developing sex-specific management and treatment approaches that offer them an equivalent chance of survival to men.
Introduction
Men and women present for coronary artery bypass graft (CABG) surgery with very different profiles: women are generally older and have more significant comorbidities1–5 and more urgent/emergent surgery,1 ,3 but have less extensive disease patterns requiring less revascularisation1–3 and shorter cross clamp times.1 Despite female sex being among the risk factors included in both the Society of Thoracic Surgeons (STS)6 and EuroSCORE risk models,7 ,8 the question of whether—and how—sex independently impacts outcomes following CABG continues to be raised, with large, recent studies that take patient risk factors into account showing contradictory results.1 ,3 ,5 ,9 Resolving this question is important because, if female sex is an independent risk factor for poorer outcomes, sex-specific strategies for treatment and management may need to be developed to offer men and women in need of surgical revascularisation equivalent chances and qualities of survival. We present the comparison of short-term mortality following isolated CABG in men versus women, and estimate the ‘excess’ deaths associated with female sex, using a large cohort (n=13 327) of consecutive patients in North Texas.
Methods
This multicentre, retrospective, cohort study included all consecutive patients who underwent isolated CABG from January 2008 to December 2012 in a hospital participating in the Texas Quality Institute (TQI). Through TQI, 32 of the 34 cardiac surgery programmes in North Texas region share the data submitted to the STS National Adult Cardiac Surgery Database6 with the Dallas-Fort Worth Hospital Council, where they are combined into a single registry and paired with administrative/claims data, enabling long-term comparative effectiveness, cost-effectiveness and quality outcomes research.10 ,11
After excluding patients with previous valve surgery (n=28), preoperative endocarditis (n=13) and/or a ventricular assist device (n=0), the final study cohort consisted of 13 327 consecutive isolated CABG patients.
Means, SDs and percentages were calculated to describe the study cohort. Differences in demographic and clinical details were assessed with a Wilcoxon test for continuous factors and a χ2 test for categorical factors. A Bonferroni correction was applied to account for multiplicity.
The STS definition for operative mortality was applied for short-term mortality: the patient died during the operation, during the subsequent hospital stay, or within 30 days from surgery. To assess the adjusted association between sex and post-CABG short-term mortality, so that the excess deaths associated with female sex could be estimated, we used a propensity-adjusted generalised estimating equations model approach.12 ,13 The propensity adjustment accounted for risk factors recognised by the STS;6 these factors are listed in table 1. A restricted cubic spline function with five knots was used to fit the propensity score as an independent variable in a generalised estimating equations model with short-term mortality as the dependent variable and sex as the independent variable. Multiple imputation of all covariates used in the propensity model was done by Markov Chain Monte Carlo simulation,14 ,15 to account for missing data (preoperative atrial fibrillation: 29.7% missing, ejection fraction: 7.3% missing and left main disease: 0.4% missing). A total of 10 imputed data sets were created using 200 burn-in iterations. The point estimates and variances from the imputed data sets were pooled using standard methods developed by Rubin.16–18 All continuous variables in the propensity model were fitted using restricted cubic splines with five knots.13 ,19 Effect modification between sex and all the risk factors listed in table 1 were tested. Where significant interactions (p<0.05) were identified, sex-stratified ORs and CIs were estimated.
STS clinical and non-clinical risk factors by sex
The excess deaths associated with female sex (ie, the number of women who would not die if women's risk of operative mortality was the same as men's) were calculated by applying the estimated adjusted risk difference between men and women to:
The total number of isolated CABGs performed on women in the present study (excess deaths in women in this study cohort); and
To the number of isolated CABG procedures performed on women in the USA each year (reported for the most recent full year in the STS Adult Cardiac Surgery database)20 (annual excess deaths in women undergoing CABG in the USA).
All analyses were conducted using SAS V.9.3, SAS Institute Inc, Cary, North Carolina, USA. The study protocol was approved by the Baylor Research Institute Institutional Review Board, and was granted a waiver for informed consent.
Results
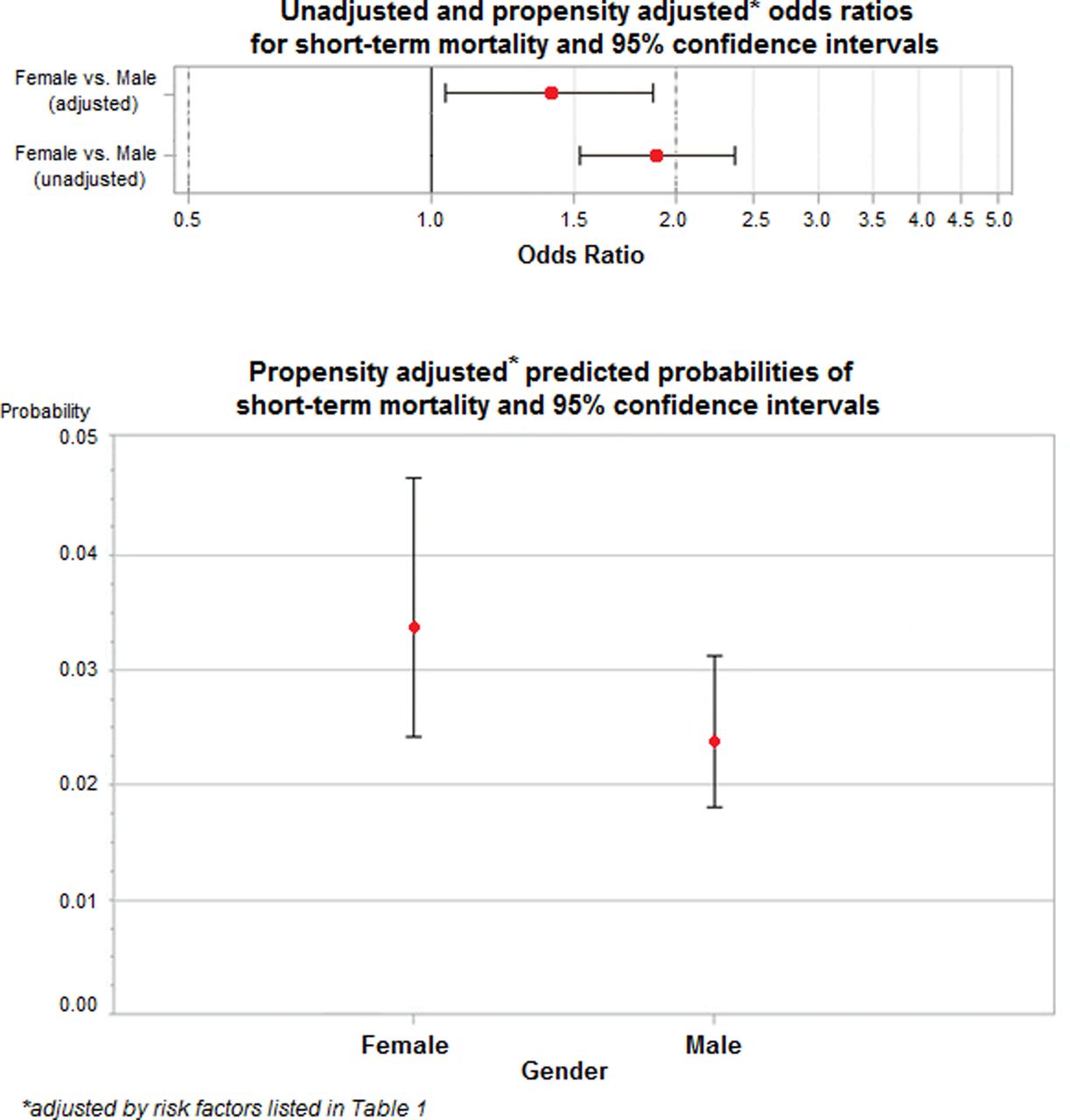
There were 343 deaths (2.6%) in the study cohort; among men, there were 206 (2.1%) deaths, while among women, there were 137 (3.9%). Patients’ clinical and non-clinical details are presented in table 1. Both the unadjusted and adjusted (for recognised STS risk factors for mortality) analyses showed that women were significantly more likely to experience short-term mortality than men (OR unadjusted=1.90; 95% CI 1.52 to 2.36; OR adjusted=1.39; 95% CI 1.04 to 1.86; figure 1). Interaction with sex was significant only for preoperative intra-aortic balloon pump (see table 1).
{kind=link}
Unadjusted and propensity-adjusted* odds ratio and propensity-adjusted* predicted probabilities for short-term mortality.
Applying the estimated adjusted risk difference observed in our study population (3.36% for women—2.38% for men) shows that the higher risk associated with female sex leads to 35 ‘excess’ operative deaths among the women included in our study (constituting >10% of the total deaths in the study cohort). In 2013, 147 600 isolated CABG surgeries were reported nationwide in the STS Adult Cardiac Surgery Database.20 Approximately, 40 000 of these procedures were performed in women.6 Applying the risk-adjusted difference estimates from our study to these numbers, 392 ‘excess’ deaths among women undergoing isolated CABG can be expected each year.
Discussion
The results of our study support a growing body of evidence indicating greater risk of short-term mortality following isolated CABG for women than men, even after adjusting for the worse preoperative clinical profiles and older age at surgery that are typical of women undergoing CABG.9 ,21–24 More importantly, it shows that this significantly greater risk of short-term mortality in women translates into 35 ‘excess’ deaths among women in the present study, and to 392 ‘excess’ deaths among the approximately 40 000 women undergoing isolated CABG in the USA each year. These ‘excess’ deaths constitute >10% of the total deaths in our study cohort, suggesting that identifying strategies to improve women's outcomes could meaningfully improve overall mortality rates for CABG.
The magnitude of the effect of female sex on short-term mortality (adjusted OR=1.39) in our study is similar to that reported in a recent meta-analysis of isolated CABG surgeries when the included studies were limited to the subgroup of four papers that performed propensity matching (OR=1.36; 95% CI 1.04 to 1.78).25 Two other studies, a large cohort study5 using the STS database and a study encompassing a Californian statewide cohort,9 also reported risk-adjusted odds of women's isolated CABG short-term mortality in similar ranges (OR=1.39; 95% CI 1.14 to 1.70 and OR=1.61; 95% CI 1.40 to 1.84, respectively). In contrast, a recent analysis of 21 534 isolated CABG patients across 18 Australian hospitals found that the higher short-term mortality seen in women in the raw data disappeared following adjustment for patient risk factors in multivariate analysis (adjusted in hospital OR=0.96; 95% CI 0.71 to 1.29; adjusted 30-day OR=0.93; 95% CI 0.68 to 1.27).3
It is still unknown what mechanism(s) cause the greater isolated CABG short-term mortality seen in women. Hypotheses include the smaller luminal diameter of coronary arteries (independent of body size) in women, which can increase the difficulty of revascularisation, and the less frequent use of left internal mammary artery grafts and bilateral internal mammary grafts.26–30 Other hypotheses include women's more extensive microvascular dysfunction (which the epicardial revascularisation performed in CABG does little to address28), their more frequent need for postoperative inotropic support and periprocedural blood transfusions, and longer lengths of hospital stay—all of which influence perioperative complications and can therefore affect short-term mortality.28 ,31 ,32 In our study cohort, a significantly greater proportion of women than men underwent off-pump CABG—a technique which previous research has suggested ‘disproportionately’ benefits women and helps narrow the sex gap inoperative mortality.5 ,33 However, re-running our analysis to adjust for the use of off-pump versus on-pump CABG did not alter our results (OR comparing women vs men=1.40; 95% CI 1.04 to 1.88; p=0.025).
Other studies suggest that increased risk for short-term mortality with female sex is not limited to CABG surgery. There is at least some evidence that female sex may be an independent risk factor for early death following percutaneous coronary intervention,34 aortic valve replacement34 and mitral valve surgery,35 although no conclusive explanations for these sex-based differences have been reached. The under-representation of women in the clinical trials on which current cardiovascular guidelines are based36 and resulting extrapolation the evidence obtained in men to guide the care provided to women37 may play a role in the broader disadvantage women experience.
The use of an observational design is unavoidable when examining the effects of sex, but is inherently unable to establish causality. The propensity-adjustment method used here mitigates this problem by allowing for a quasi-randomised experimental analysis. To minimise the possibility that relevant confounding factors remained unaccounted for, we adjusted for risk factors recognised by the STS.6 Importantly, our results are based on a large cohort of patients drawn from 32 of the 34 cardiac surgery programmes in North Texas (covering 7 million people),38 and include a representative mix of the predominant racial/ethnic groups in Northern America, making them highly generalisable to the broader population of patients undergoing isolated CABG surgery. The study database is a regional subset of the national STS’ Adult Cardiac Database, and so is limited to the data collected for that initiative. As such, that data necessary to examine important questions such as whether sex-based differences in time of death (during surgery vs postsurgery hospitalisation vs postdischarge) and cause of death exist, or whether sex-based differences in extent of coronary artery disease, such as previous research has identified,39 contributed to the excess mortality seen in women, were not available.
In conclusion, our results support the hypothesis that women have a greater risk of CABG short-term mortality, independent of pre-existing comorbidities or demographics, than men. While the absolute difference in adjusted risk may seem small for a single patient (3.36% for women vs 2.38% for men in our study population), applying it to the ∼40 000 women undergoing isolated CABG procedures in the USA each year,6 ,20 it translates into 392 ‘excess’ deaths. Given that the current clinical guidelines simply extrapolate the evidence obtained in men to women,37 further research is needed to investigate the causal mechanisms behind the sex-related difference in CABG short-term mortality. The results of such research might inform the development of sex-specific treatment and management approaches that could bring women's risk of short-term mortality when undergoing CABG in line with men's, and meaningfully reduce total short-term mortality rates.
References
Footnotes
Contributors GF was involved in study concept and design, data analysis and interpretation, drafting the manuscript. BLH, JE and WSR were involved in study conception, data interpretation and revising the manuscript for critical intellectual content. BDP was involved in data analysis, drafting the manuscript. BdG was involved in literature review, data interpretation, drafting the manuscript. DMS and TKP were involved in data collection and management, revising the manuscript for critical intellectual content. SLP was involved in data collection, revising the manuscript for critical intellectual content.
Funding This work was funded in part by the Bradley Family Endowment to the Baylor Health Care System Foundation (Dallas, Texas, USA), The Baylor Health Care System Cardiovascular Research Committee (Dallas, Texas, USA) and the Discovery Foundation (Dallas, Texas, USA).
Competing interests None declared.
Ethics approval Baylor Research Institute Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Study data will be available to other researchers at their request. Researchers who would like to use data from the published study should submit their requests to GF.