Article Text

Abstract
Objective A previous randomised trial showed that structured, nurse-led atrial fibrillation (AF) care is superior to conventional AF care, although further research is needed to determine the outcomes of such care in a real-world setting. We compared the outcomes of patients in real-world, nurse-led, structured hospital AF clinics with the outcomes of a randomised trial of the efficacy of a nurse-led AF clinic, with respect to a composite outcome of cardiovascular-related hospitalisation and death.
Methods All patients were referred to the AF nurse specialist by cardiologists. The AF nurse specialist provided patient education, risk-factor control and stimulated empowerment and compliance. During follow-up, treatment was adjusted according to clinical guidelines. Patient education was repeated, and compliance with medical treatment was controlled. The study size was powered as a non-inferiority study. Outcome measures were adjudicated by the same principles in both cohorts.
Results A total of 596 patients from the real world and 356 patients from a clinical trial were included in this study. No significant difference between groups with respect to age, type of AF or CHA2DS2VASc score was found. The composite primary end point occurred with an incidence rate of 8.0 (95% CI 6.1 to 10.4) per 100 person-years in the real-world population and 8.3 (95% CI 6.3 to 10.9) per 100 person-years in the clinical trial, with a crude HR of 0.83 (95% CI 0.56 to 1.23).
Conclusions Structured, nurse-led, hospital-based AF care appears to be effective, and patient outcomes in an actual, hospital-based, structured AF care are as least as good as those in trial settings.
- QUALITY OF CARE AND OUTCOMES
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this subject?
A randomised study has demonstrated that structured, nurse-led, guideline-based atrial fibrillation (AF) care was superior to standard care.
What does this study add?
Patient outcomes in an actual, hospital-based, structured AF service are as least as good as those in trial settings.
How might this impact on clinical practice?
Structured, hospital-based AF service is effective.
Background
The management of atrial fibrillation (AF) is often inadequate because of a lack of adherence to clinical guidelines.1–3 Indeed, a lack of adherence to diagnostic and therapeutic recommendations (eg, inadequate control of anticoagulation therapy) can have serious clinical implications, including a higher risk of thromboembolism, bleeding and death.4 A more effective and patient-centred organisation of AF care is therefore warranted. A randomised study recently demonstrated that structured, nurse-led, guideline-based AF care was superior to standard care in terms of hospitalisation due to cardiovascular (CV) causes or death.5 This structured, nurse-led AF service also resulted in lower costs and better quality of life,6 ,7 presumably driven by the combined effect of patient education and better adherence to clinical guidelines. However, the dramatically better outcomes of nurse-led AF care versus usual care reported from Maastricht led to sound scepticism. Patients randomised to the nurse-led AF care were seen by a dedicated staff, who reported the study results in scientific journals.5–7 In the real-world setting, nurse-led AF clinics will be staffed by nurses, who will never deal with AF at an academic level. Thus, there has been fear that the high quality care with an excellent outcome delivered in the academic hospital of Maastricht could not be replicated.
Nurse-led, structured, hospital-based AF care appears to be feasible, although further research is needed to determine whether this approach could be effective in real-world settings. ‘Real-world patients’ are defined here as those patients who have been in contact with the hospital system either because they were hospitalised for symptoms of AF or because they were referred to an outpatient cardiology clinic by a general practitioner. The aim of this study was to compare patient outcomes in nurse-led, structured, hospital-based AF care between real-world patients and those in the nurse-led care arm of a randomised trial of the efficacy of a nurse-led AF clinic, the only such trial that has been reported to date.5 We hypothesised that patient outcomes in an actual population of patients in nurse-led AF clinics would be at least as good as those obtained in a clinical trial patient population with respect to a composite outcome of hospitalisation and death due to CV causes.
Materials and methods
Study design and population
Real-world data consisted of prospectively collected baseline and follow-up data from two nurse-led AF clinics of the Regional Hospital of Central Jutland located in Viborg Regional Hospital and Silkeborg Regional Hospital, Denmark, which serve a population of approximately 260 000 people. The patients included in this study were ≥18 years of age with AF documented by ECG and/or Holter monitoring; the patients were referred by a cardiologist to the nurse-led AF clinics in this study between January 2012 and January 2014. An ECG was performed in all patients. Each patient's type of AF was categorised as paroxysmal, persistent or permanent according to the patient's symptoms and medical history. Follow-up data were obtained from the AF clinic database and from electronic patient files, which guaranteed complete follow-up. The participants of this study were unaware of the study. The study was approved by The Danish Data Protection Agency j. no. 1-16-02-589-14 and by the Danish Health and Medicines Authority j. no. 3-3013-740/1/. According to Danish law, the study did not require informed consent from the study participants.
The randomised clinical trial ‘Nurse-led care versus usual care for patients with AF’5 was conducted in the Maastricht University Medical Centre in the Netherlands and recruited patients between January 2007 and December 2008. The design of the study has been described previously.8
Patient care plans
The real-world patients, who were referred by a cardiologist on a hospital ward or in an outpatient clinic, were offered the components of a care package in the outpatient, nurse-led AF clinic. Prior to the first contact in the nurse-led AF clinic, the patients underwent laboratory testing and, optionally, Holter monitoring and 24-h ambulatory blood pressure monitoring. The AF care consisted of 1–4 planned, individual visits during the first year, with 3–4-month intervals between visits. The number of visits was determined by knowledge of AF, symptoms, need for adjustment of medication and treatment strategy. If changes in a patient's treatment were required, then the patient was seen at additional visits or was followed up by telephone. For questions between visits, patients could telephone the AF nurse specialist. When starting of Class 1C Antiarrhythmic drugs or elective cardioversion was needed, the AF nurse specialist planned the procedure with the department of cardiology and informed the patient. The AF specialist nurses were supervised by a cardiologist, and any modification of therapy, including increases in medication dosages or changes in the treatment strategy, was approved by the cardiologist.
To increase patient empowerment, the AF nurse specialist provided tailored, evidence-based patient education about AF, including the physiological and pathological basis of symptoms and of the underlying condition.9 ,10 Patients also received information about factors that cause AF and promote its progression, about how AF affects quality of life and about treatment options for AF. There was a strong emphasis on providing information about anticoagulant treatment and practical advice as well as the importance of adhering to treatment regimens and advice. Patients were given information about stroke prevention and awareness, and they also received information about heart rate management and rhythm control, including information about how to handle palpitations and how to measure their pulses. Patients were screened for other CV risk factors, and empowerment and adherence to treatment were encouraged. At each visit, the risk category for stroke and thromboembolism was assessed using the CHA2DS2VASc (congestive heart failure/left ventricular dysfunction, hypertension, age ≥75 years (doubled), diabetes, stroke (doubled)—vascular disease, age 65–74 years, and sex category (female)) scoring system,11 and the risk of bleeding was assessed using the HASBLED (hypertension, abnormal renal/liver function, stroke, bleeding history or predisposition, labile international normalized ratio (INR), elderly (eg, age >65 years, frailty, etc), drugs/alcohol concomitantly) scoring system.12 The European Heart Rhythm Association symptom classification for AF EHRA scores13 was applied, an ECG was recorded, and the patients’ blood pressure was measured. Patients were informed about whom to contact for advice if needed. During follow-up, treatment was adjusted as needed, according to clinical guidelines.14 ,15 Patient education was repeated, and adherence and compliance were controlled by reviewing the medication list in conjunction with the patient. Questions about side effects, routines for intake, dose, remember technologies (pill dispensing box, SMS, email, diary) both at home and outdoor, and problem solutions were discussed with the patient.
Outcomes
To compare the outcomes of the real-world AF clinics with those of the AF clinic in the clinical trial, all outcomes among real-world patients were adjudicated using the same principles as those used in the clinical trial. The primary outcome was a composite of CV-related hospitalisation and death. Hospitalisation was defined as at least one overnight stay for heart failure, ischaemic stroke, acute myocardial infarction, systemic embolism, major bleeding, severe arrhythmic events, or life-threatening adverse effects of drugs. CV deaths were classified using a modified Hinkle and Thaler16 classification system. An independent clinical end point committee adjudicated all primary outcome events on the basis of pre-specified criteria. The real-world outcomes were adjudicated by the neurologist who chaired the event committee of the clinical trial, using the same definitions of CV-related death and hospitalisation as were used in the clinical trial.5
Statistical analysis
The aim of the study was to determine whether the results observed in the real-world AF clinics cohort were inferior or non-inferior to the results observed for patients randomised to nurse-led AF care in the clinical trial cohort. The study power calculation was based on an expected 10% event rate after 1 year of observation based on findings in the Maastricht study,5 an α level of 5%, a β level of 20% and a non-inferiority limit of 3.5%. Thus, a 12-month event rate ≤ 11.1% was considered to represent non-inferiority of the patient outcomes. On the basis of these assumptions, it was calculated that a minimum of 500 study participants would need to be recruited from AF clinics to participate in this study.
Continuous variables are reported as means±SDs, and categorical variables are reported as observed numbers and percentages. We used Pearson’s χ2 test for categorical variables, and the Mann-Whitney test and t test for comparisons of ordinal and continuous variables between independent groups.
We used Cox regression analysis to calculate HRs, both unadjusted and adjusted for sex, age, comorbidity and oral anticoagulant treatment, together with 95% CIs. We considered a value of p<0.05 to be statistically significant. All analyses were performed using Stata V.11.0 (College Station, Texas, USA).
Results
Table 1 shows the baseline characteristics of the 596 real-world AF patients and the 356 clinical trial AF patients
Characteristics of patients according to setting of patient
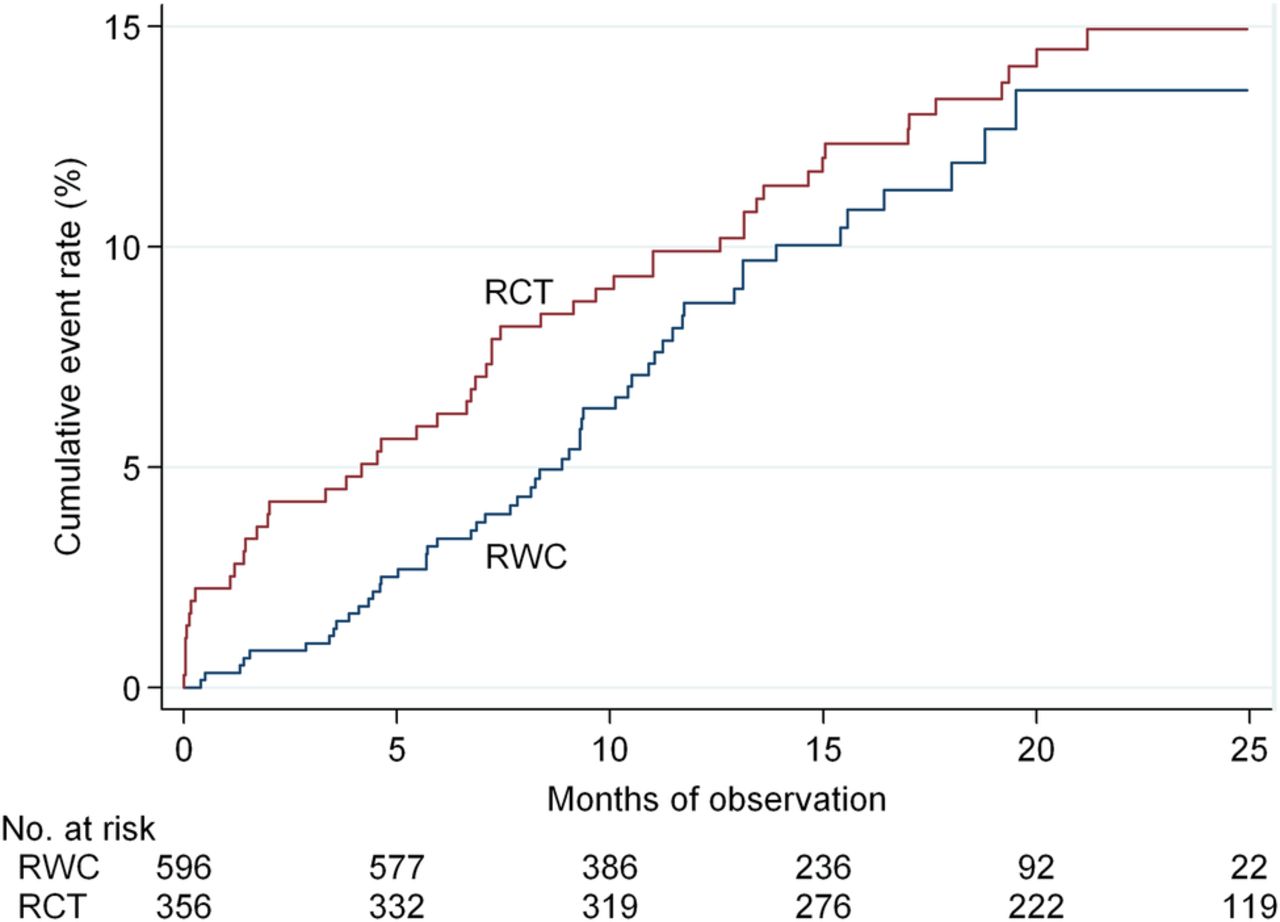
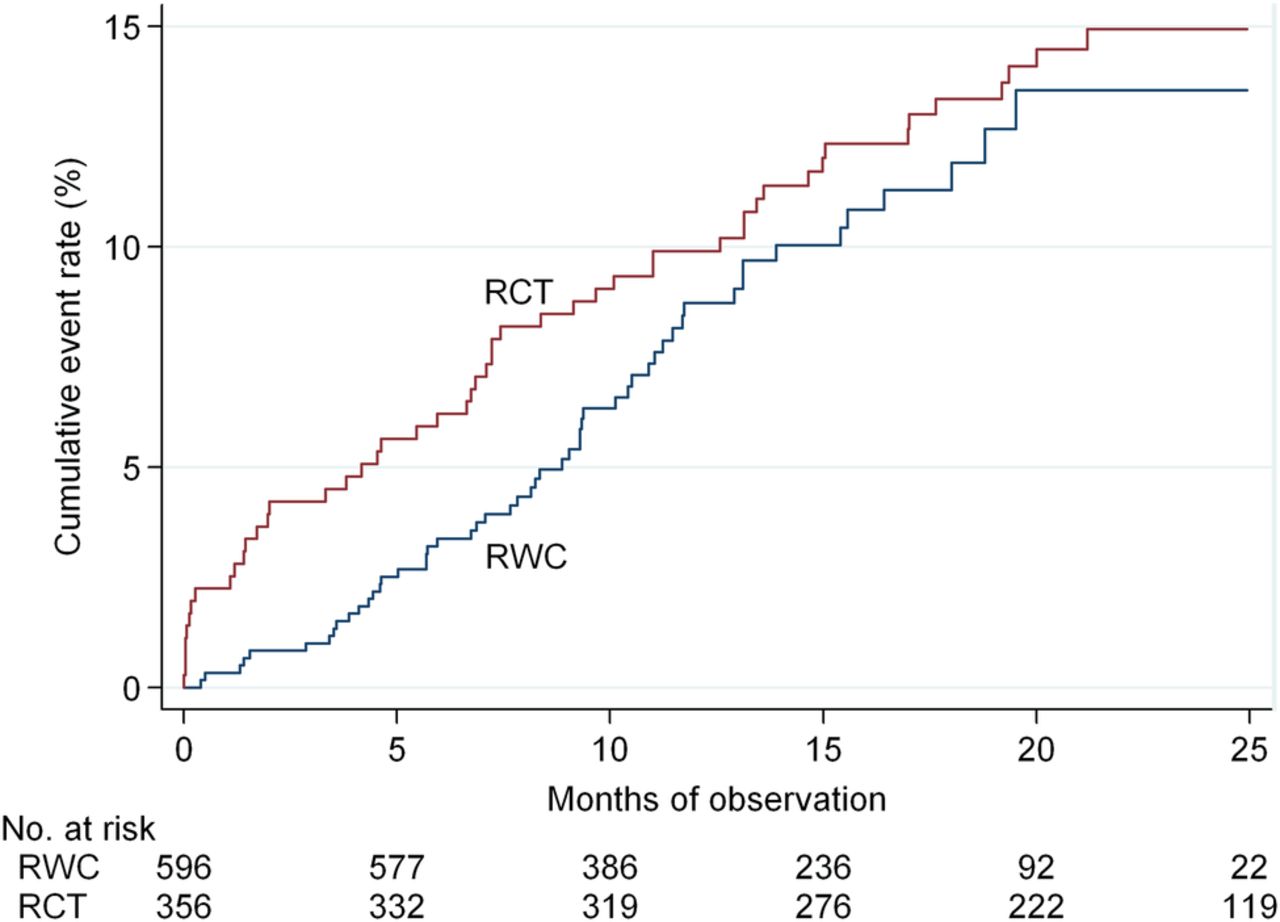
During a total of 1373 years of follow-up (the mean follow-up period was 1.2 years in the real-world cohort and 1.9 years in the clinical trial cohort), the composite primary end point occurred with an incidence rate of 8.0 (95% CI 6.1 to 10.4) per 100 person-years in the real-world cohort and 8.3 (95% CI 6.3 to 10.9) per 100 person-years in the clinical trial cohort (table 2).
Incidence rates of outcomes according to setting of patient care
Figure 1 shows the cumulative event rate of the primary outcome.
{kind=link}
Cumulative event rate of the primary outcome. The primary outcome is a composite of first occurrence of cardiovascular hospitalisation and/or cardiovascular death. RWC, real-world cohort; RCT, randomized controlled trial.
Table 3 shows the absolute number of outcomes for each setting of patient care. Table 3 also reveals no significant difference in the primary outcome or any of its components between the nurse-led AF clinics in the real-world cohort and in the clinical trial cohort (crude HR: 0.83; 95% CI 0.56 to 1.23). Three (0.5%) CV deaths occurred in the real-world cohort and 4 (1.1%) occurred in the clinical trial cohort (crude HR: 0.53; 95% CI 0.12 to 2.38). A total of 50 (8.4%) patients were hospitalised for CV causes in the real-world cohort, and 48 (13.5%) patients were hospitalised for CV causes in the clinical trial cohort (crude HR: 0.84; 95% CI 0.56 to 1.26). A total of 2 (0.3%) stroke events occurred among the patients in the real-world cohort, compared with 3 (0.8%) in the clinical trial cohort, and 5 (0.8%) major bleeds occurred among the patients in the real-world cohort, compared with 6 (1.7%) in the clinical trial cohort. The total mortality observed consisted of 9 deaths in the real-world cohort (1.5%) and 13 (3.7%) deaths in the clinical trial cohort (crude HR: 0.57; 95% CI 0.24 to 1.35). Adjusting for sex, age, comorbidities and the use of oral anticoagulation therapy did not change any of the HRs substantially. For the composite outcome, the age-adjusted and sex-adjusted HR was 0.83 (95% CI 0.56 to 1.22), the age-adjusted, sex-adjusted and warfarin-adjusted HR was 0.84 (95% CI 0.57 to 1.24), and the age-adjusted, sex-adjusted and comorbidity-adjusted HR was 0.84 (95% CI 0.56 to 1.26).
Number of outcomes and HRs of outcomes according to setting of care
Discussion
The patient outcomes of nurse-led, structured AF care in a routine clinical setting were not inferior to those observed in a previous randomised trial. Notably, no substantial difference in a range of well-established prognostic factors, including age, type of AF, history of underlying disease and consequently CHA2DS2VASc score, was observed between the real-world patients enrolled in our study and the patients who participated in a previous clinical trial. Our finding that the real-world AF clinics performed as well as the trial clinic may have several explanations. A larger proportion of the patients in the real world were taking oral anticoagulants, whereas more patients in a clinical trial received aspirin; this difference reflects changes in clinical guideline-based treatment practices during the study period based on a change from using the CHADS2 score to using the CHA2DS2VASc score and also reflects the availability of new oral anticoagulants, which has allowed more patients to be eligible for oral anticoagulation.1 ,17 However, the main difference between the CHADS2 score and the CHA2DS2VASc score is the recommendation of oral anticoagulation to patients with a CHA2DS2VASc score of 1. The risk of stroke in patients with a CHA2DS2VASc score of 1 is rather low, and therefore we cannot expect the present study to have statistical power to evaluate any difference in outcome between our two cohorts based alone on the introduction of the CHA2DS2VASc score.
The incidences of stroke and systemic embolism were lower in the AF clinic patients than in those observed in pivotal randomised trials of the efficacy of new oral anticoagulants versus warfarin, including the Randomised Evaluation of Long-Term Anticoagulation Therapy (RELY) trial,18 the Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation (ARISTOTLE) trial,19 and the Rivaroxaban Once Daily Oral Direct Factor Xa Inhibition Compared with Vitamin K Antagonism for Prevention of Stroke and Embolism Trial in Atrial Fibrillation (ROCKET-AF) trial.20 We recognise that we only counted stroke events requiring hospitalisation; however, we consider the low stroke-related hospitalisation rates that we observed to be a very important finding because structured service addresses many components of a care pathway such as medical examinations, planning and coordination of treatment, patient education and patient empowerment developed through self-management and reinforcement of treatment adherence.
Adherence to oral anticoagulation is improved by individually tailored educational interventions.21 Tailored educational interventions about AF leads to increased patient knowledge and understanding of AF, which are important factors to be able to make informed choices and actively participate in their own treatment process.22
Structured, nurse-led hospital care has also been shown to be effective in heart failure and resulted in less hospitalisation and decreased all-cause mortality.23 Recently, nurse-led service in relation to elective cardioversion was reported to be feasible, effective and safe.24 ,25 Confirmation of these results can potentially expand structured, nurse-led AF service to also include elective cardioversion. The 2014 guidelines on AF from the National Institute for Health and Care Excellence (NICE) recommend, on the basis of the limited evidence-based literature available to date, a personalised package of care in the management of AF.26 The following components of a care package are recommended for patients with AF: stroke awareness and measures to prevent stroke, rate control, assessment of symptoms for rhythm control, whom to contact for advice if needed, psychological support if needed, and up-to-date and comprehensive education and information on the (1) causes, effects and possible complications of AF; (2) heart rate management and rhythm control; (3) anticoagulation therapy; (4) practical advice about anticoagulation therapy and (5) support networks (such as CVcharities).26
Mortality due to non-CV causes was observed more frequently than mortality due to CV causes. The dominance of non-CV mortality over CV mortality was also observed in the RELY trial.27 This finding could provide an impetus for directing future AF trials into randomising AF patients with multiple disease conditions into structured, multidisease care versus standard care.
Strengths and limitations of this study
The strengths of this study include the population-based design, the standardised and prospective data collection and the independent adjudication of clinical outcomes.
Although we obtained detailed data for each patient, we cannot exclude the possibility that residual confounding occurred when the two patient populations were compared in our study, because the study cohorts were from different time periods, and also treatment guidelines changed during the study period.
Furthermore, the follow-up period of our study was relatively short, and longer term follow-up data, in particular with respect to patient adherence to oral anticoagulation therapy, would provide additional useful information. In addition, the statistical precision of our study was modest. Finally, caution is warranted before generalising our findings to all patients with AF because the patients referred to the AF clinics in our study were not necessarily representative of all patients with an incident diagnosis of AF; for example, Danish patients with a first-time diagnosis of AF have a mean age of 73 years compared to the mean age of 67–68 years in this study.28
There is increasing focus on renal function as a risk factor for stroke and bleeding in patients with AF.28 Renal function was not accounted for in the clinical trial cohort, and was therefore not recorded in the real-world cohort. We agree that there could be residual confounding from not knowing renal function. However, renal function is closely correlated to age and comorbid conditions, which were accounted for.
The real-world AF clinic nurses knew that their outcomes were being monitored, as did the nurse in the clinical trial. From the beginning of 2016, all Danish general practitioners and hospitals will be under surveillance for clinical performance by a national AF quality management programme. Surveillance may hopefully contribute to better patient management and outcomes across the healthcare system.
After taking into consideration both the strengths and weaknesses of our study, we conclude that structured, nurse-led, hospital-based AF care in routine clinical settings can have as least as good patient outcomes as the results achieved in clinical trial settings.
Acknowledgments
The authors are grateful to Dr C L Franke of Heerlen, the Netherlands for adjudicating the end point events.
References
Footnotes
Contributors IQ, JMLH, DSM, AEA, HMM, GDO, AO, LSM, SPJ and LF all participated in the original conception and design of the study. LSM, LF and IQ were involved in the data analysis and interpretation. IQ, JMLH, DSM, AEA, HMM, GDO, AO, LSM, SPJ and LF participated in the interpretation of data as well as the drafting and critical review of the paper. IQ and LF take responsibility for the overall content as guarantors.
Competing interests None declared.
Ethics approval The study was approved by The Danish Data Protection Agency j. no. 1-16-02-589-14 and by the Danish Health and Medicines Authority j. no. 3-3013-740/1/.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.