Article Text

Abstract
In patients with heart valve disease, echocardiography is the mainstay for diagnosis, assessment and serial surveillance. However, other modalities, notably cardiac MRI and CT, are used if echocardiographic imaging is suboptimal but can also give complementary information to improve assessment of the valve lesion and cardiac compensation to aid the timing of surgery and determine risk. This statement discusses the way these imaging techniques are currently integrated to improve care beyond what is possible with echocardiography alone.
- VALVULAR DISEASE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Heart valve disease is common and a major indication for imaging in all cardiac centres. Imaging needs to assess: (1) valve morphology to determine the aetiology and suitability for invasive intervention; (2) haemodynamic severity; (3) remodelling of the left ventricle (LV) and right ventricle (RV); (4) involvement of the aorta and (5) the prediction of adverse cardiovascular events. Echocardiography will continue as the first-line technique for diagnosis and is likely to remain the mainstay for assessment and serial surveillance in most cases. However, other modalities, notably cardiac MRI (CMR) and CT, are used if echocardiographic imaging is suboptimal and can give complementary information, particularly to aid risk assessment.
The purpose of this statement is to summarise those multimodality approaches to valve disease currently available and how these might develop in the future. It is not intended as a systematic review. The aim is to encourage thinking beyond echocardiography towards an integrated approach to imaging in valve disease that uses each technique to its best advantage.
Aortic valve disease
Transthoracic echocardiography (TTE) is used for assessing the aetiology and severity of the valve disease and the remodelling response of the LV. If echocardiographic image quality is poor (table 1), CT or CMR can image the valve (figure 1) while CMR can measure velocities across the valve.1 Anatomical area on CT or CMR can be useful and, although not the same as effective orifice area, it is possible that a combination of anatomical area and calcium score will give a reliable measure of the grade of stenosis2 (figure 1).
Role of CT and CMR beyond those provided by echocardiography
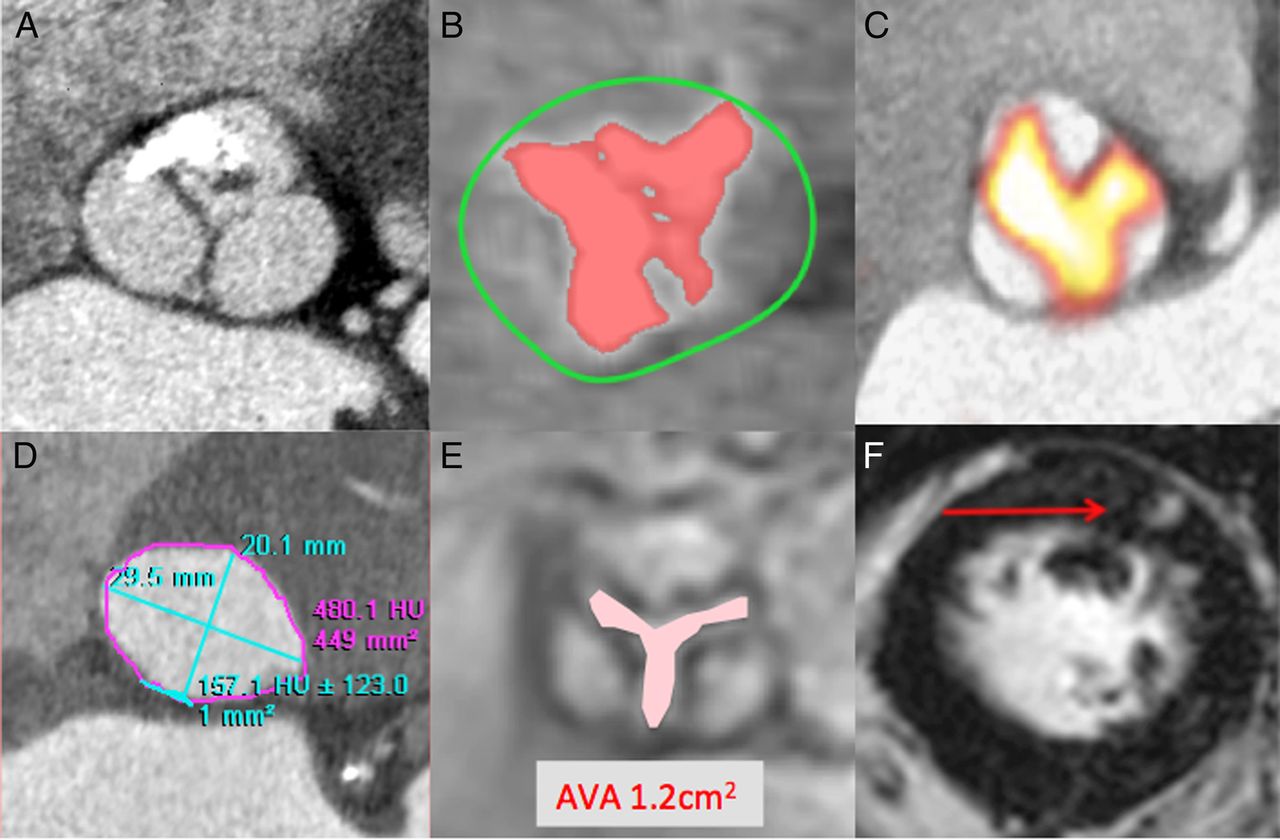
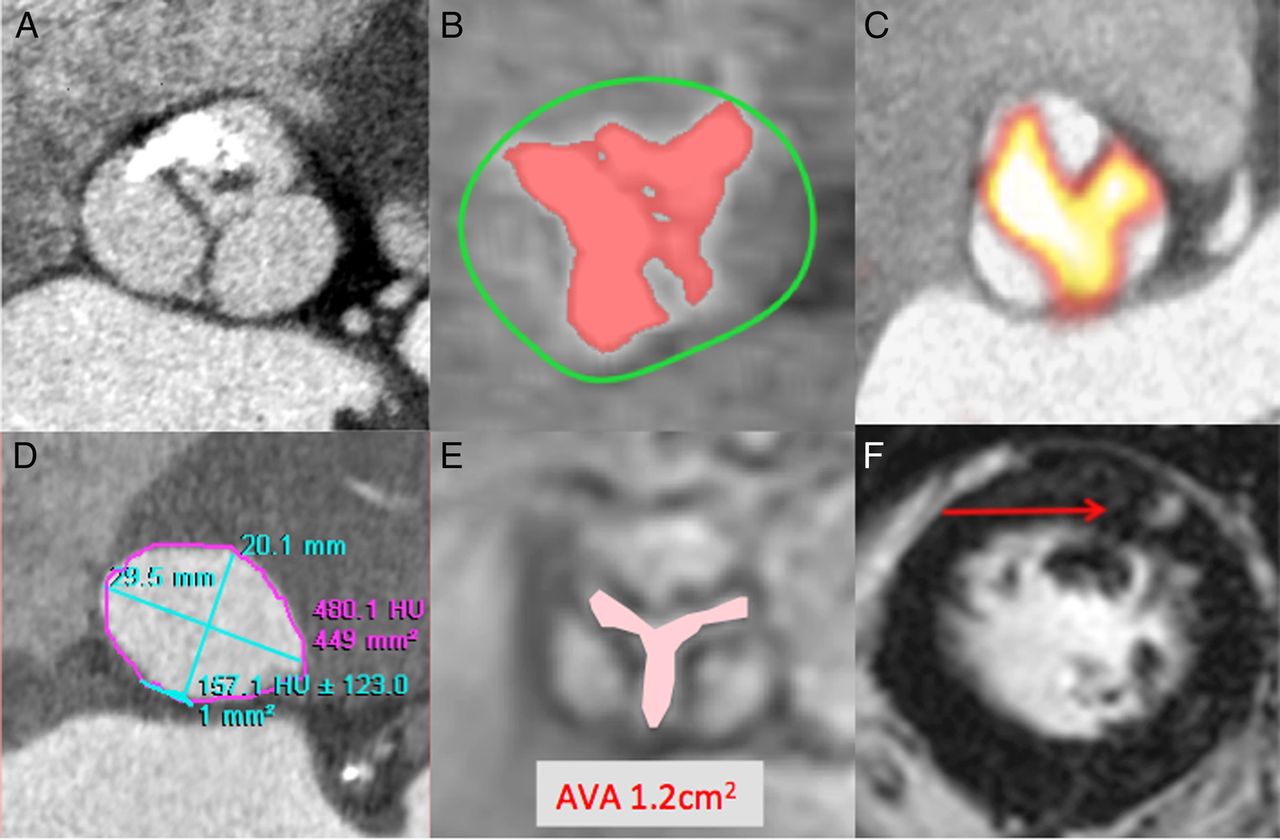
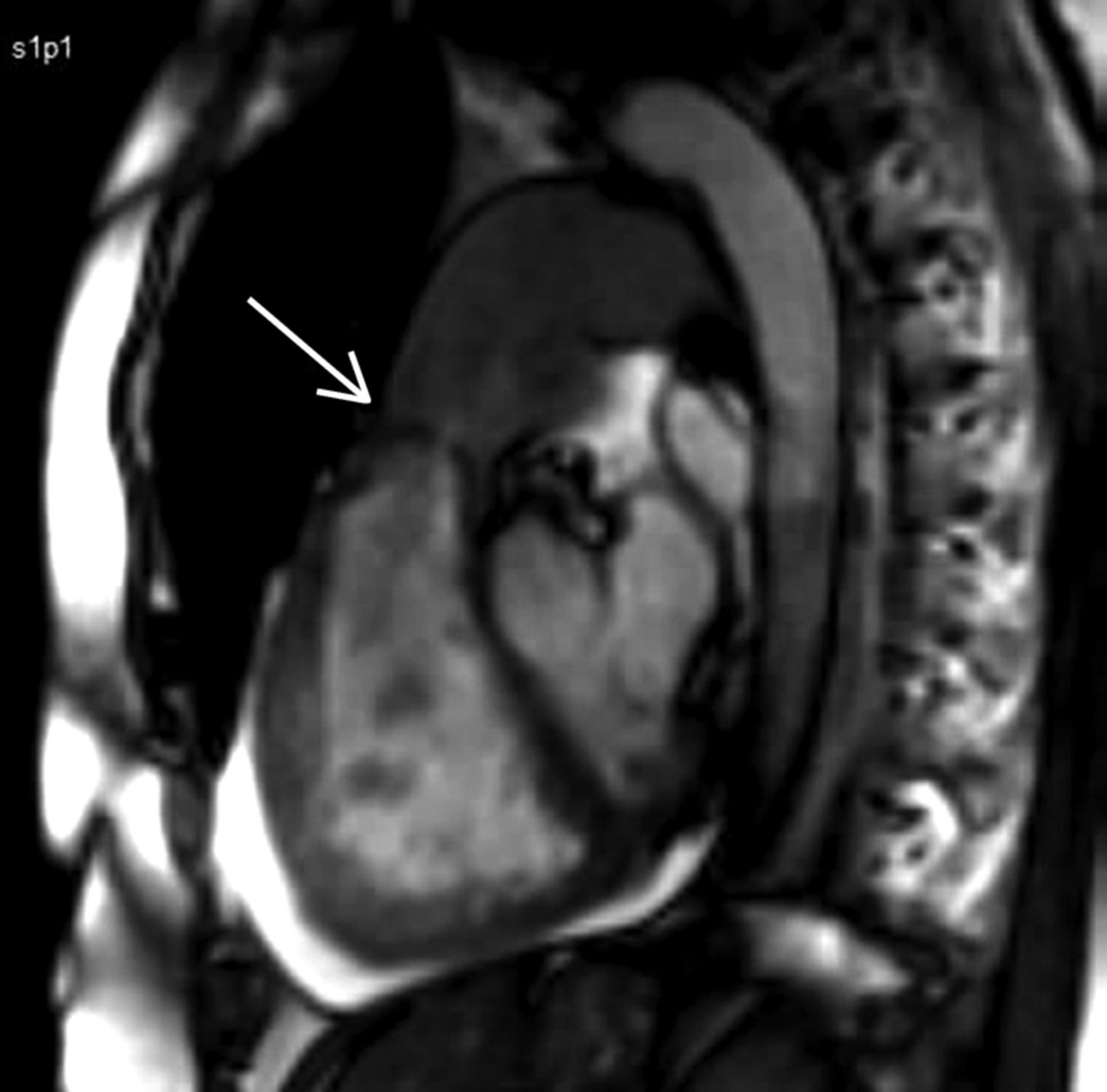
Multimodality imaging of aortic stenosis. (A) Contrast CT imaging of the aortic valve can provide detail regarding valve morphology and the distribution of calcification. (B) CT calcium scoring allows reproducible quantification of the calcific burden, which acts as a marker of disease severity. (C) Fused positron emission tomography and CT imaging with 18F-fluoride provides an indication of ongoing calcification activity in the valve. CT has an important clinical role in the workup of patients prior to transcatheter aortic valve implantation, providing accurate dimensions of the annulus for valve sizing (D) while cardiac MRI can be used to planimeter the aortic valve area (E) and to detect replacement myocardial fibrosis, red arrow (F).
In aortic stenosis, the echocardiographic minimum data set is the peak transaortic velocity, the mean gradient and the effective orifice area,3 but these measures sometimes give discordant results.2 CT can help resolve this. First, the LV outflow tract may be oval rather than circular4 and CT can assess the size and shape of the LV outflow tract to allow correction of the continuity equation. This can also be carried out using three-dimensional (3D) echocardiography provided that image quality is adequate.5 Second, CT can give a calcium score for the valve which can differentiate severe from more moderate stenosis6–8 with one suggested cut-off of 2065 Agatston units (AU) in males and 1275 AU in females.
The risk of events in aortic stenosis is dependent on a number of factors including the results of exercise testing. TTE suggests a high risk of events if the Vmax has increased by >0.3 m/s in a year with heavy calcification as assessed subjectively,9 but quantification of calcification by CT is likely to be more accurate.6 ,7 Fused positron emission tomography (PET)/CT imaging with 18F-fluoride could assess both the burden of valve calcification (CT calcium score) and its activity (18F-fluoride PET) and is of potential use in refining the prediction of aortic stenosis progression.10 ,11
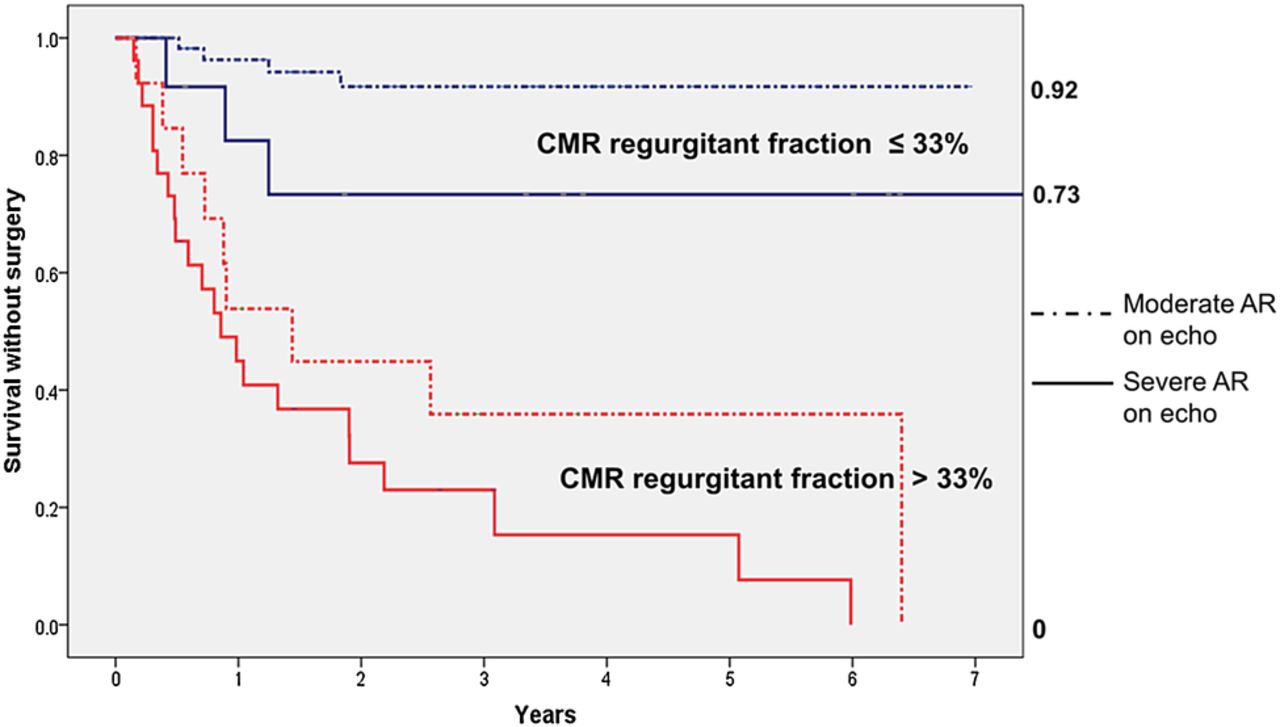
Estimation of the grade of aortic regurgitation (AR) using multiple echocardiographic modalities remains standard.12 However, some situations, for example, a bicuspid valve with an eccentric jet, may be difficult to assess and CMR quantification may provide useful complementary information. In addition, there is evidence that CMR identifies patients at high risk of events better than does TTE13 (figure 2). The quantification of AR appears to differ between echocardiography and CMR, with a significant overlap between grades, and a suggestion of lower quantities by CMR than TTE (figure 2). This may be due to differing techniques for each method, and/or the potential for mild underestimation of AR by CMR.
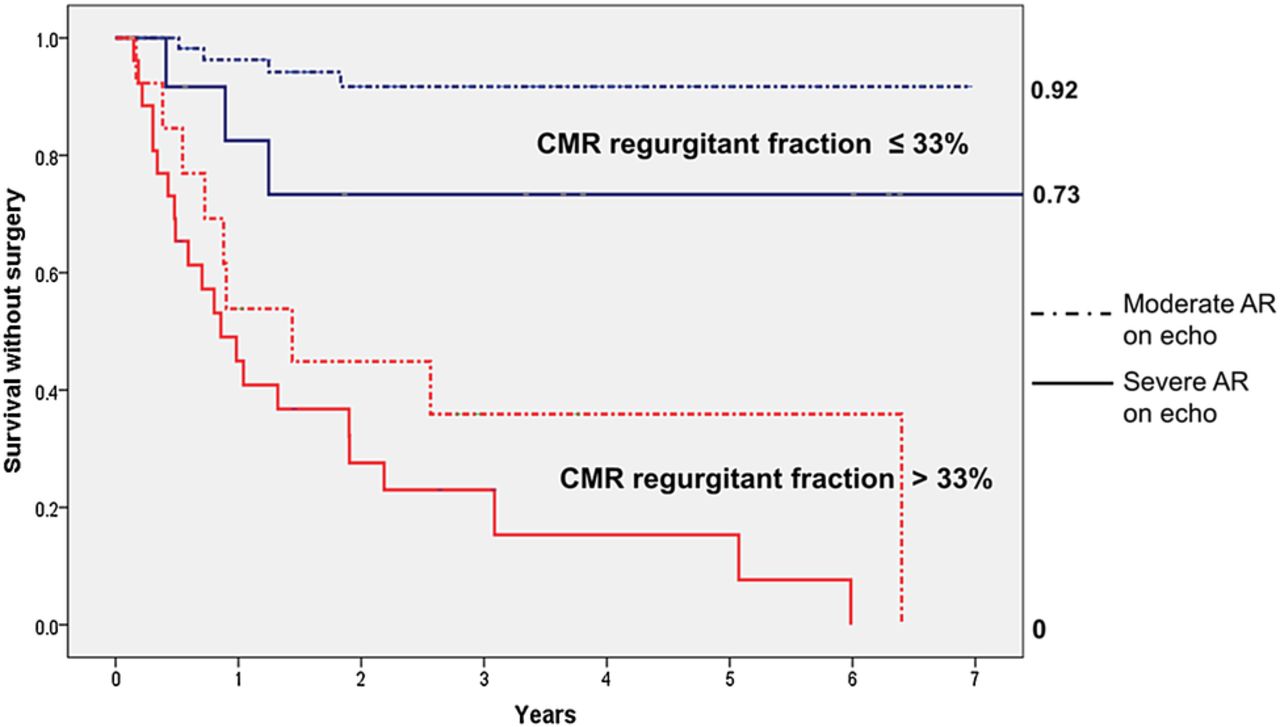
Comparison of CMR and echocardiography in aortic regurgitation. In 109 asymptomatic patients with moderate or severe aortic regurgitation on echocardiography, prognosis was better related to the regurgitant fraction on CMR with a cut-point of 33%.The graph shows CMR regurgitant fraction ≤ 33% in blue and >33% in red. The regurgitation was either moderate or severe by echocardiography in both of these two CMR groups.
CT (figure 3) or CMR (figure 4) is already used in clinical practice if the ascending aorta is not well imaged on TTE or to check the aortic diameter when approaching a surgical threshold. It may be better to use CT when considering referral for aortic valve surgery since this can also detect calcium in the ascending aorta and identify porcelain aorta as an indication for a transcatheter procedure instead of conventional surgery. In those at no more than moderate coronary risk (eg, younger patients with a bicuspid aortic valve), CT can produce an assessment of the aorta and coronary arteries in one study. CT is also useful in the workup towards intervention. For transcatheter aortic valve implantation, it provides information additional to echo including the degree of calcification of the leaflets, the distance to the coronary arteries and the calibre, tortuosity and calcific burden of the peripheral vessels.14
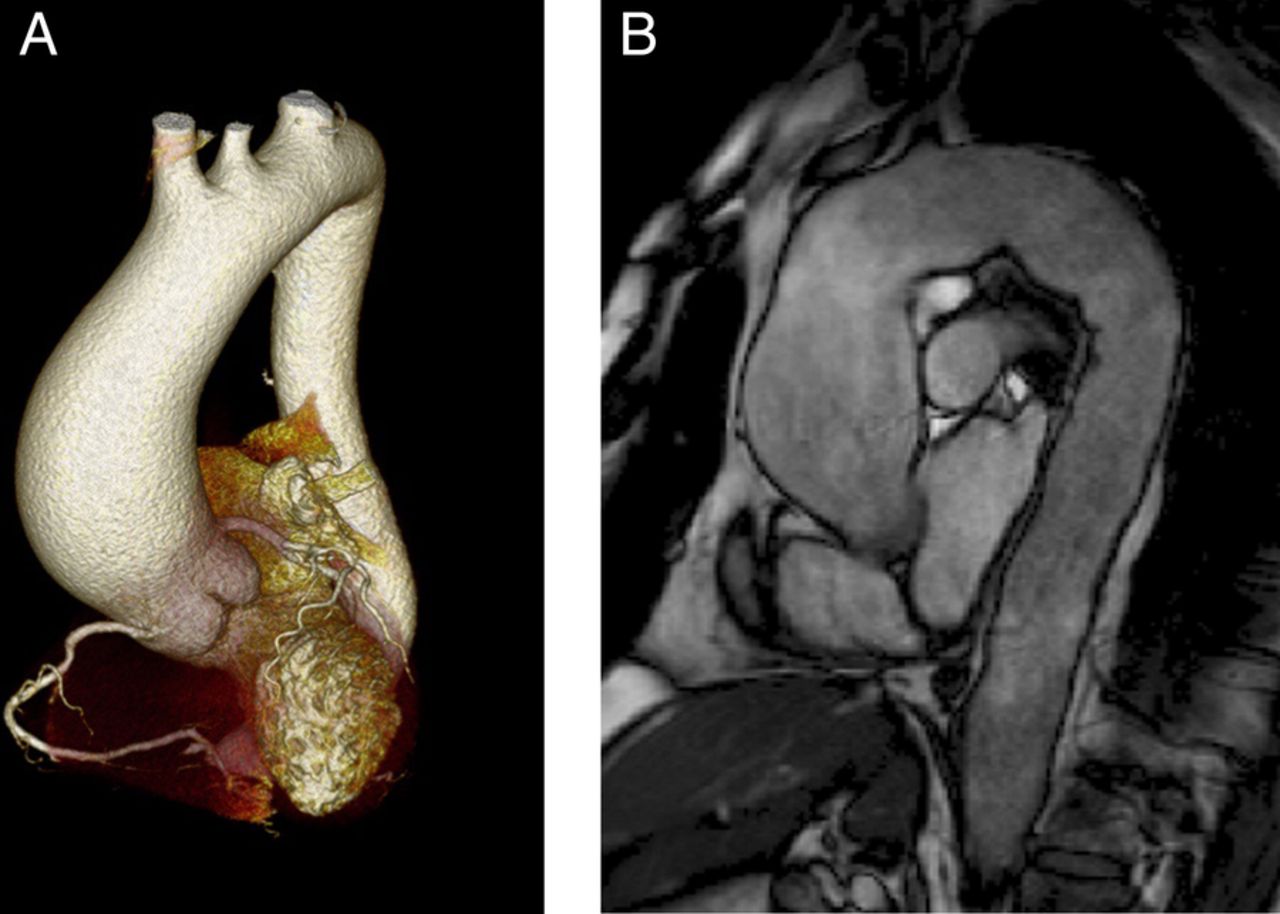
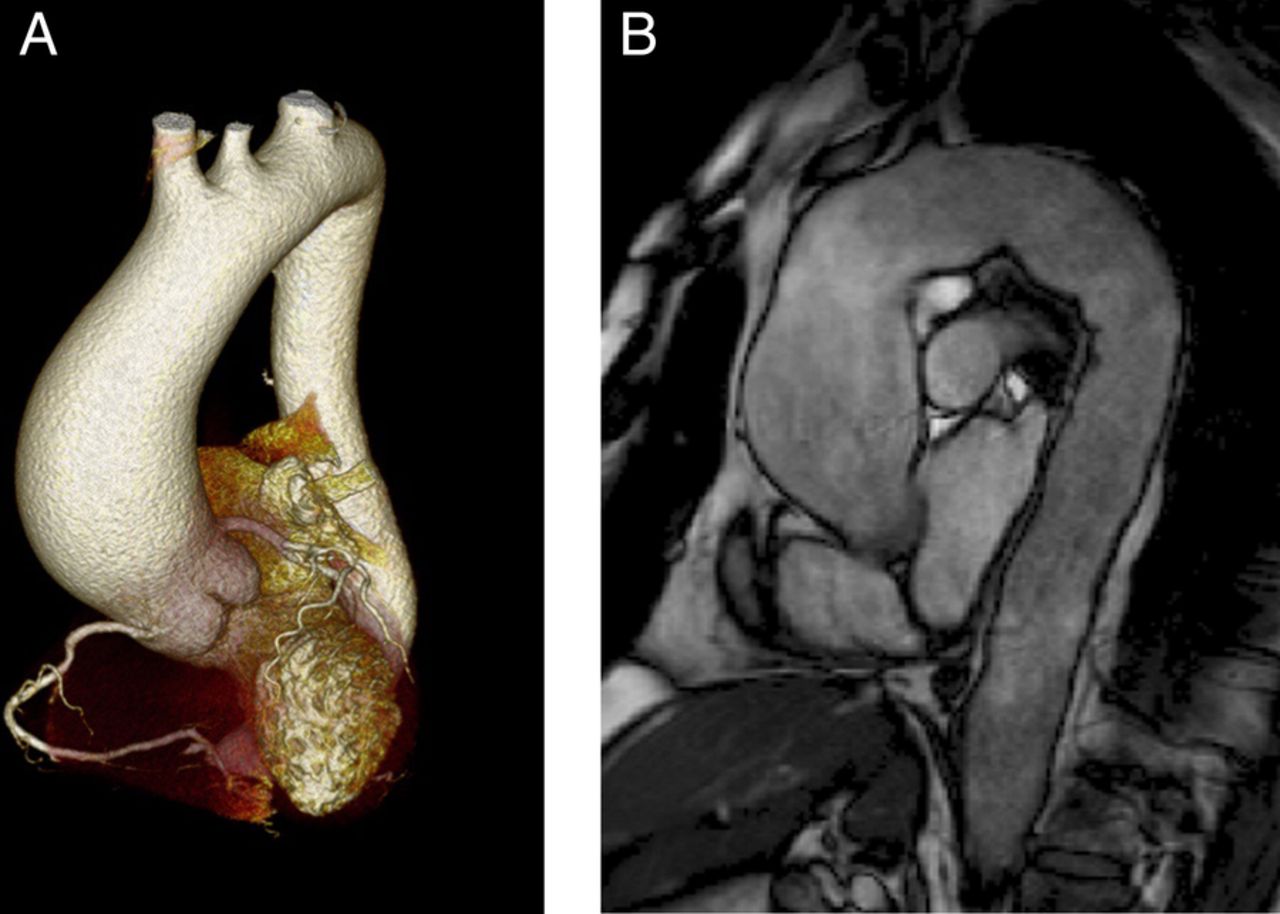
Imaging the aorta using CT and cardiac MRI (CMR). On the left is a reconstructed three-dimensional-rendered CT scan of the heart with a dilated ascending aorta and on the right is a steady-state free precession (SSFP) image on CMR of a moderately dilated ascending aorta.

The aorta using cardiac MRI (CMR). (A) A contrast MR angiogram showing critical coarctation and very dilated thoracic collateral vessels. (B) A four-dimensional CMR flow image showing very helical flow in the ascending aorta in a patient with a bicuspid aortic valve.
Current thresholds for surgery in AR are based on LV diameters on TTE, but these may be unreliable since the LV becomes more spherical in severe AR and a linear dimension may not be representative of the whole LV. There is still little information on volumetric thresholds for surgery, but it is possible that LV volumes by CMR will be better than those by TTE. It is most likely that myocardial fibrosis detected by CMR15–17 will provide a powerful predictor of events in aortic stenosis and regurgitation, but further work is required before this can be recommended clinically. CMR is far more accurate than TTE for quantifying LV mass and is therefore useful in research studies to document the regression of LV hypertrophy after surgery,18 although it has not yet been shown to be a prognostic marker.
Mitral valve disease
TTE is the mainstay for assessing the aetiology, morphology and grade of stenosis and regurgitation as well as the adaptation of the right and left heart. A 3D echo, particularly using transoesophageal echocardiography (TOE), improves identification of the minimum orifice for planimetry in mitral stenosis19 (figure 5) and may also improve the assessment of valve anatomy and function of the valve in mitral regurgitation caused by mitral prolapse19 (figure 6).
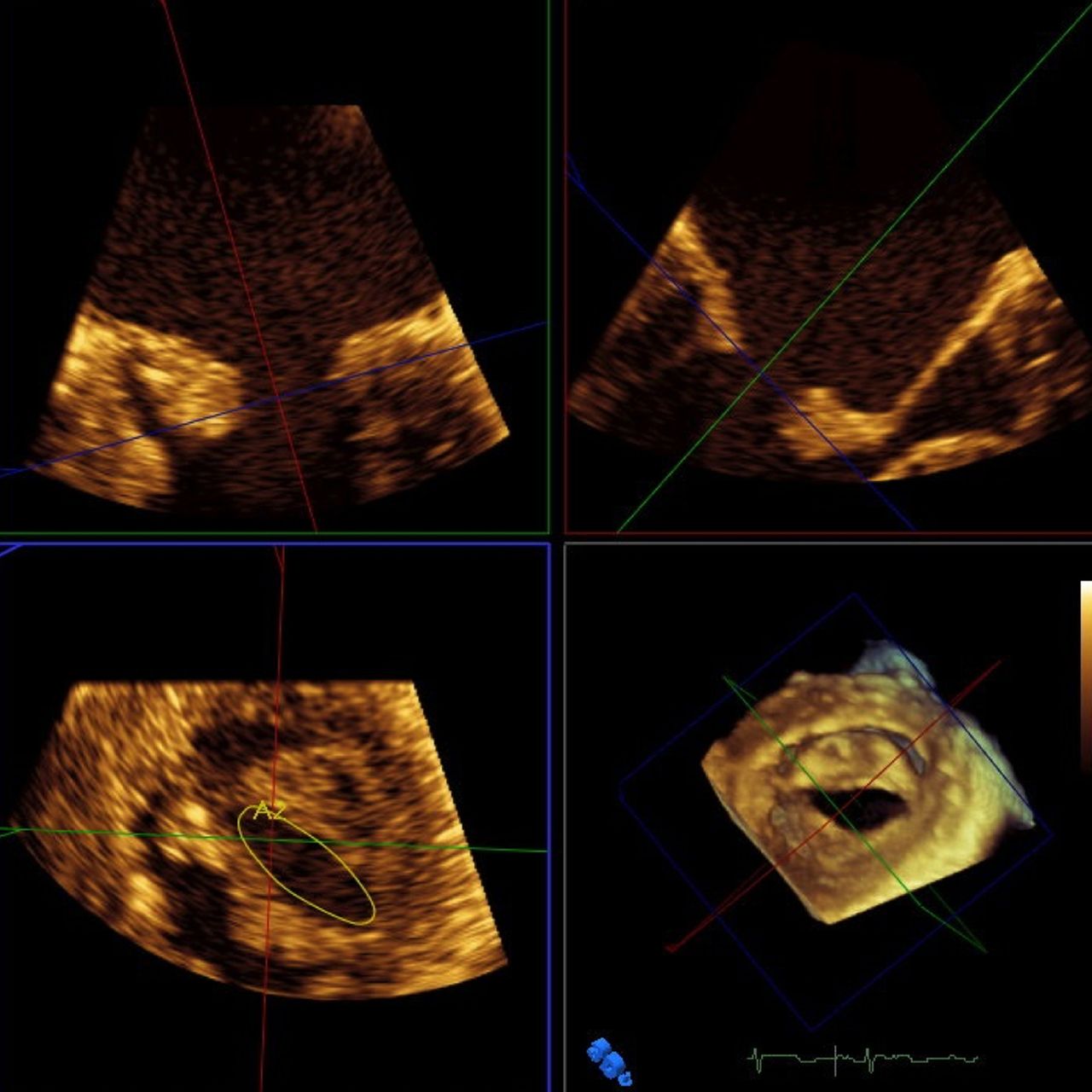
A three-dimensional (3D) echocardiogram showing planimetry of a stenotic mitral valve. The 3D image allows alignment of the plane to ensure that planimetry is performed at the minimum orifice (courtesy Dr Stam Kapetanakis).

Three-dimensional (3D) in mitral prolapse. (A) A 3D image of the valve showing prolapse of the middle scallop, P2 using the Carpentier classification. (B) A colour-contoured map with prolapsing areas in red and restricted areas in blue. The main lesion is prolapse of the middle portion of the anterior leaflet. (C) A colour-contoured map in a patient with functional mitral regurgitation showing restriction of both mitral leaflets (courtesy Dr Stam Kapetanakis). A, anterior; AL, anterolateral; Ao, aorta; P, posterior; PM, posteromedial.
CMR is already used to assess mitral valve morphology if the TTE window is suboptimal and quantification can be performed by CMR if the TTE is uncertain or produces discrepant results. In mitral regurgitation, thresholds for surgery are based on a linear diameter on TTE, but volumes are expected to be more reliable.20 This is a potential role for CMR, although this is not a clinical routine. It is possible that risk stratification by CMR assessment of the grade of MR and LV volumes may aid the frequency of follow-up clinically and by echocardiography and the need for functional tests.
CT can provide an assessment of mitral annular calcification if this appears severe on TTE to help determine the feasibility and safety of mitral repair or replacement. For percutaneous mitral valve interventions, CT may also be useful in further defining mitral valve anatomy and the subvalve structures including false tendons and hypertrabeculation. CT may be useful for predicting LV outflow tract obstruction after percutaneous mitral valve implantation.
Tricuspid and pulmonary disease
TTE is used for initial diagnosis and will retain a first-line role into the future. However, CMR is used routinely for the assessment of the RV in adult congenital disease,21 and we believe it should be used more frequently in severe tricuspid or pulmonary regurgitation (table 1) where decisions for surgery rest on an accurate assessment of RV volume, or a serial change in RV size or function. It is also better for refining the description of the pulmonary valve, quantifying pulmonary regurgitation looking for obstruction above and below the valve and defining branch pulmonary stenoses21 (figure 7). CMR is particularly useful in larger adult patients in whom assessment of the pulmonary valve with echocardiography may be difficult.
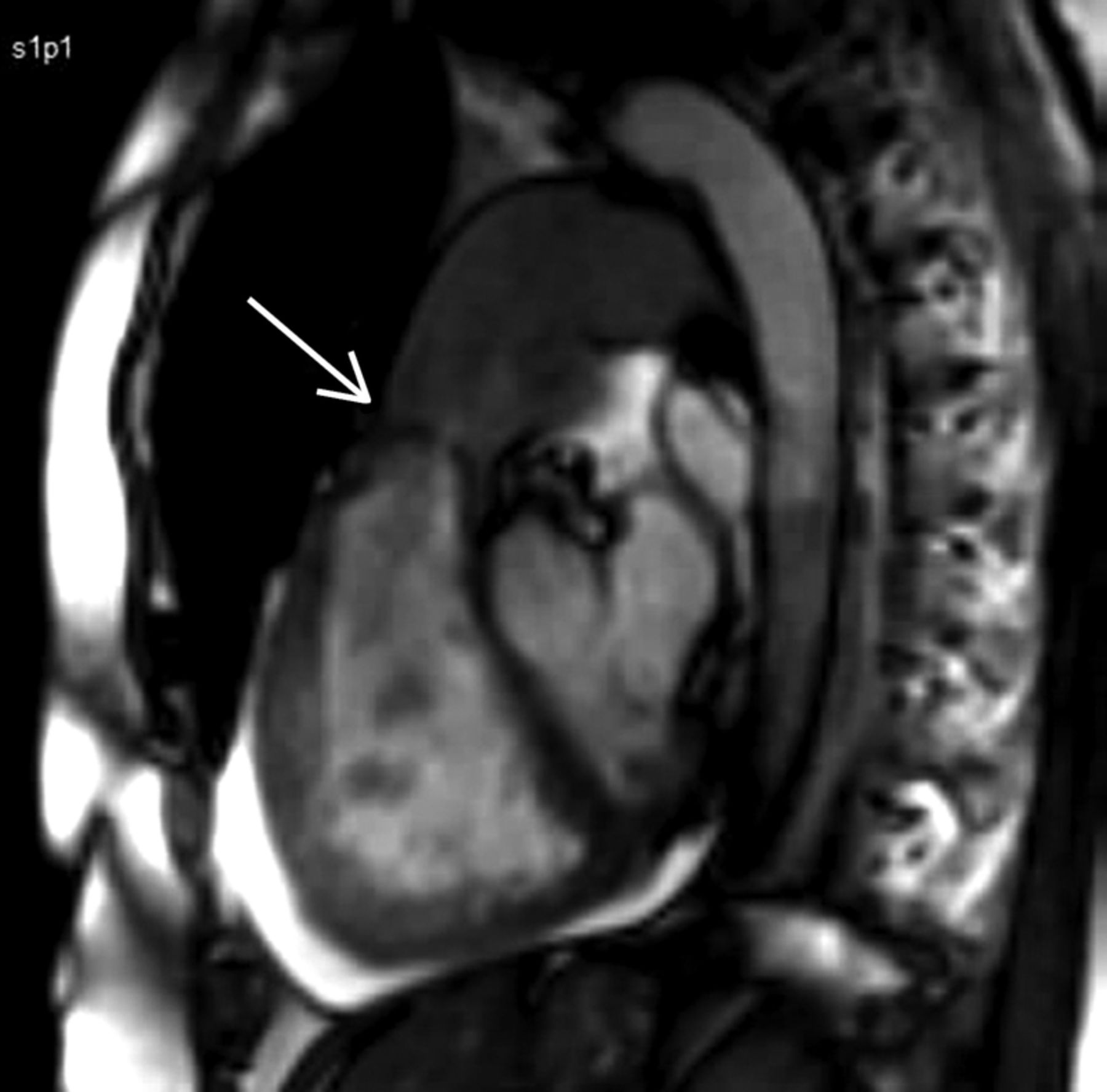
Severe congenital pulmonic stenosis. This is a cardiac MRI image (steady-state free precession, SSFP) in a sagittal view through the right ventricular outflow tract, demonstrating mobile leaflets but fused tips of the pulmonic valve (arrow).
Tricuspid valve repair may be recommended at the same time as left-sided surgery depending on the grade of tricuspid regurgitation and the annulus diameter. The latter is better assessed using 3D echocardiography than 2D and also using CMR. CT is not usually helpful for right-sided valve disease apart from excluding lung pathology contributing to elevated pulmonary artery pressures.
Replacement heart valves
TTE can usually make the initial diagnosis of valve obstruction or abnormal regurgitation. However, TOE is often needed to quantify paraprosthetic mitral regurgitation to determine the cause of mitral obstruction.
CT is likely to have a key role in patients with unexpectedly high gradients, especially when immediate postimplantation echocardiograms are not available (table 1). In the early recovery period after surgery in biological replacement valves, high gradients may be caused by small thrombi at the base of the cusps and these can be detected by CT22 ,23 but not by TTE or TOE. Thereafter, the differentiation of patient-prosthesis mismatch from primary failure in the aortic position may be difficult on TTE or even TOE since the cusps or occluder may not be imaged fully. CT can then be used for imaging the leaflet motion of bileaflet mechanical valves, although fluoroscopy may be still better for a single tilting disc and caged-ball valves. Pannus is also difficult to detect by TTE and TOE, but there is growing evidence that CT is useful24 (figure 8).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Pannus related to a stented biological valve. (A) CT and (B) surgical finding in the same patient.
In mechanical replacement valves CMR can assess forward flow patterns and localise and quantify regurgitant flow. This is especially so for paravalvular leaks (both in conventional and transcatheter replacement valves), which can be challenging to assess with echocardiography. CMR is also useful for ventricular volumes and function if TTE images are suboptimal.
Endocarditis
The complementary use of TTE and TOE has a high sensitivity and specificity for vegetations and local complications.25 However, CT may be of value in detecting vegetations on heavily calcified valves26 ,27 and may detect abscesses missed by TOE. CMR is not ideal for detecting small vegetation due to their small size and chaotic, highly mobile motion which presents problems for the images acquired over several cardiac cycles. Both CT and CMR are useful if aortic root pathology is not well seen on TTE and if TOE is not feasible, or if there is complex pathology (eg, false aneurysms or complex abscesses). Coronary CT angiography can be considered in place of invasive coronary angiography to avoid the risk of dislodging vegetation.
In the future, combined PET-CT is likely to be useful for diagnosing endocarditis in difficult cases, for example, infection of implantable electrical devices28 and replacement heart valves,29 although issues with a myocardial uptake of this tracer will need to be resolved. This indication is now included in the most recent European Society of Cardiology guidelines on infective endocarditis.30
Conclusion including future work
Multimodality imaging implies using each technique where it has most to offer rather than simply repeating full studies by each technique. Examples are surgery based on a combination of severe aortic stenosis on TTE and high CT calcium score, or trials of early surgery in aortic and mitral regurgitation based on CMR assessment of regurgitant fraction and LV volumes. This approach has obvious advantages but has not been tested clinically and is largely unresearched. This statement is intended to draw attention to the exciting possibilities and to act as a call for the research community to plan collaborative projects.
References
Footnotes
Contributors JBC wrote the original draft and all other authors contributed significantly to rewriting and finalising the document and providing images.
Competing interests GJM-H receives lecture fees from GE for cardiac CT education.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.