Article Text

Abstract
Background Patients with diabetes are at increased risk of acute coronary syndromes (ACS) and their mortality and morbidity outcomes are significantly worse following ACS events, independent of other comorbidities. This systematic review sought to establish the optimum management strategy with focus on P2Y12 blockade in patients with diabetes with ACS.
Methods MEDLINE (1946 to present) and EMBASE (1974 to present) databases, abstracts from major cardiology conferences and previously published systematic reviews were searched to June 2014. Relevant randomised control trials with clinical outcomes for P2Y12 inhibitors in adult patients with diabetes with ACS were scrutinised independently by 2 authors with applicable data was extracted for primary composite end point of cardiovascular death, myocardial infarction (MI) and stroke; enabling calculation of relative risks with 95% CI with subsequent direct and indirect comparison.
Results Four studies studied clopidogrel in patients with diabetes, with two (3122 patients) having primary outcome data showing superiority of clopidogrel against placebo with RR0.84 (95% CI 0.72–0.99). Irrespective of management strategy, the newer agents prasugrel (2 studies) and ticagrelor (1 study) had a lower primary event rate compared with clopidogrel; RR 0.80 (95% CI 0.66 to 0.97) and RR 0.89 (95% CI 0.77 to 1.02), respectively. When ticagrelor was indirectly compared with prasugrel, there was a trend to an improved primary outcome with prasugrel (RR 1.11 (95% CI 0.94 to 1.31)) particularly in those managed with percutaneous coronary intervention (PCI) (RR 1.23 (95% CI 0.95 to 1.59)). Prasugrel demonstrated a statistical superiority with prevention of further MI with RR 1.48 (95% CI 1.11 to 1.97). This was not at the expense of increased major thrombolysis in MI (TIMI) bleeding rates RR 0.94 (95% CI 0.59 to 1.51).
Conclusions This meta-analysis shows the addition of a P2Y12 inhibitor is superior to placebo, with a trend favouring the use of prasugrel in patients with diabetes with ACS, particularly those undergoing PCI.
- CORONARY ARTERY DISEASE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this subject?
In acute coronary syndrome (ACS), clopidogrel in addition to aspirin shows a reduction in cardiovascular death, myocardial infarction and stroke. However, in the patient with diabetes, there has been a suggestion of a muted response to clopidogrel, cited as multifactorial, including genetic, metabolic, cellular and clinical. This has increased the interest in more novel P2Y12 receptor antagonists, such as prasugrel and ticagrelor.
What does this study add?
In patients with diabetes with ACS, the addition of a P2Y12 receptor inhibitor is superior to placebo in reducing cardiovascular mortality, non-fatal myocardial infarction, and non-fatal stroke without significantly increasing major bleeding events.
Prasugrel is superior to clopidogrel, with a trend to superiority against ticagrelor in this cohort, particularly in those undergoing percutaneous coronary intervention, without amplified risk of major bleeding.
How might this impact on clinical practice?
Guidance committees need to consider a more tailored approach to ACS management.
The findings from this study support further randomised control trials directly comparing prasugrel and ticagrelor, particularly in the diabetes population.
Background
Acute coronary syndromes (ACS) are a spectrum of cardiovascular conditions characterised by the presence of an unstable atherosclerotic plaque with overlying thrombus.1 Globally, the prevalence of diabetes mellitus (DM) is increasing,2 ,3 and given that this population is well described to have increased platelet reactivity,4–6 it is unsurprising that in large landmark antiplatelet trials, as many as 15–39% of all patients presenting with ACS have a background of DM7 ,8; this figure correlates well with registry data percentages (GRACE registry 26%, Swedeheart registry 24%, PACIFIC registry 35%).9–11 Furthermore, this population is known to have worse mortality and morbidity outcomes compared to patients without diabetes; independent of other comorbidities.12
This increased aggregation of platelets in DM is driven primarily by hyperglycaemia affecting a multitude of pathways including increasing p-selectin expression via activation of protein kinase C, impaired function of endogenous antiplatelet agents such as nitric oxide and prostacyclin,13 amplified platelet adhesion,14 a proinflammatory environment2 and increased platelet turnover.15 Importantly, upregulation of P2Y12 signalling and GPIIb/IIIa surface receptors are also implicated.3 ,14 Therefore, with the focus of pharmacological management of ACS being the reduction of thrombus burden and platelet reactivity,16 ,17 targeting P2Y12 receptors is of great importance particularly in this population, who may stand to receive the most benefit.
Until recently, clopidogrel was the most widely used P2Y12 receptor inhibitor in addition to aspirin, following randomised control trial data showing a reduction in cardiovascular death, myocardial infarction (MI) and stroke.8 ,18 ,19 However, in the patient with diabetes, there has been a suggestion of a muted response to clopidogrel, which has been cited as multifactorial, including genetic, metabolic, cellular and clinical.20 ,21 This has increased the interest in more novel P2Y12 receptor antagonists, such as prasugrel and ticagrelor. Published data has led to preferential use of these agents in the general population,7 ,22 ,23 and possible better outcomes with prasugrel in the cohort with diabetes,2 ,15 but no specific data has been systematically reviewed with both direct and indirect comparison for the management of the patient with diabetes.
Review question
To establish, through the available literature, the optimum antiplatelet therapy practice for management of patients with DM who present with ACS.
The specific review questions:
In combination with aspirin, which is the superior agent for P2Y12 blockade to improve the primary outcome of cardiovascular (CV) death, non-fatal MI and non-fatal stroke (CV accident, CVA)?
Is this benefit outweighed by increased risk of major bleeding (secondary outcome)?
Methods
This review was reported in accordance with the PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) guidelines,24 and a protocol prior to embarking on search was written (see online supplementary appendix 5).
Supplementary appendix 5
Search strategy and study selection
MEDLINE and EMBASE databases were systematically searched up to 18 June 2014 with no date or language restrictions. The search threads were limited to human, adult (≥18 years) and randomised controlled trials evaluating: clopidogrel, cangrelor, ticagrelor, prasugrel, elinogrel, P2Y12 receptor antagonist, P2Y12 receptor inhibitor, ADP receptor antagonist or ADP receptor inhibitor. The results were combined with the Boolean operator ‘OR’ and linked to Medical Subject Headings.
Following exclusion of duplicates, the retrieved titles and abstracts were independently screened by two authors (JAR and OIB) for relevant studies with focus on coronary artery disease. The full texts for the remaining studies were obtained.
The authors reviewed these residual articles by electronically searching the studies for the word stems ‘diab’, ‘mellitus’ or ‘DM’. Studies were excluded if they did not contain these terms, or only included in baseline patient characteristics. Each figure was individually searched to ensure no data relating to a diabetes patients subset. Also explored was the documentation of supplementary data using stem ‘supplement’, ‘append’ and ‘online’. This data was then evaluated for results relevant to the review. Medically trained peers fluent in that language translated the foreign language papers discovered.
Finally, the authors again independently assessed for the presence of clinical outcome data for ACS (ACS, ST elevation MI, non-ST elevation MI and unstable angina) distinct from stable disease. The remaining studies were analysed to confirm there was clinical outcome data of P2Y12 receptor inhibition in patient with diabetes presenting with ACS. Any discrepancies in results were resolved by group consensus.
In parallel with the systematic search process, we searched for studies in major cardiology conference abstract databases (American Heart Association (AHA), American College of Cardiology and European Society of Cardiology (ESC)). Further we retrieved other meta-analyses of antiplatelet agents reviewing the studies included and manually searched the references to ensure no relevant studies were missed.
Data extraction
The authors scrutinised the resulting studies, and relevant data was extracted, as outlined in the protocol. This included: title, author(s), country, publication year, study period, patient population, treatment arms, outcome definition, follow-up duration, overall incidence, diabetes patients subgroups, number of patients and relative risks with 95% CI.
The outcome measures included both primary and secondary outcome measures. Primary outcome measures mentioned were: CV mortality, non-fatal MI, non-fatal CVA, and any other relevant clinical end point. Secondary outcomes incorporated, but were not limited to, major bleeding. Methodological quality was assessed via the ‘The Cochrane Collaboration's tool for assessing risk of bias’ utilising the protocol or design and rationale papers to aid.25 Any discrepancies were resolved by group meeting and discussion with a third investigator if agreement not met (AH).
Data synthesis
The eligible studies were entered into RevMan5 software package, and the statistical methods were programmed into RevMan V.5.3 analysis software.
The number in each comparator group and the number of events were extracted. For the dichotomous data, the risk ratios (RR) along with 95% CIs were calculated. In cases of common comparators and outcomes, the results were pooled using the fixed effects and random effects models dependent on heterogeneity. Heterogeneity was explored with the Cochrane Q statistic, which was considered to be significant if p<0.10, and if significant a random effect model was used to allow generalisation of the results. Z tests were used to test for the overall effect.
Indirect comparison analysis of relative risk was performed to evaluate prasugrel versus ticagrelor, and both newer P2Y12 inhibitors against control. This was completed using Bucher's method.26
Results
Literature search
Articles numbering 1162 were identified on the search of MEDLINE and EMBASE following restriction to human adult randomised control trials. Review of the title and abstract excluded 896 papers, with elimination of 184 articles due to failure to mention diabetes beyond baseline characteristics. Absence of clinical outcomes or a separate ACS cohort resulted in exclusion of further 65 articles. Therefore, 17 papers, consisting of study populations from seven randomised control trials were included in the analysis.7 ,8 ,18 ,19 ,22 ,27–38 The search overview can be found in online supplementary appendix 2. Study populations, design and outcomes are documented in online supplementary appendix 4.
Supplementary appendix 2
Supplementary appendix 4
Seven papers evaluated clopidogrel as the intervention of interest in four study populations. Two studies compared clopidogrel with placebo in addition to aspirin therapy.8 ,18 ,32 One reviewed clopidogrel against aspirin,19 ,37 and finally one population examined double-dose clopidogrel versus standard-dose therapy in a 2×2 factorial design with aspirin low and high doses.33 ,34
Seven papers were written based on data from two study cohorts comparing prasugrel with clopidogrel,7 ,22 ,28–31 ,38 and three relevant papers generated from single study examining ticagrelor versus clopidogrel.27 ,35 ,36 The initial trials were all found to be high quality and low risk of bias, as demonstrated in online supplementary appendix 1; using Cochrane risk of bias tool.25 Each study's treatment arms were balanced for characteristics and management strategy (eg, coronary artery bypass grafting (CABG), PCI or fibrinolysis, dependent on the study).
Supplementary appendix 1
Diabetes versus non-diabetes
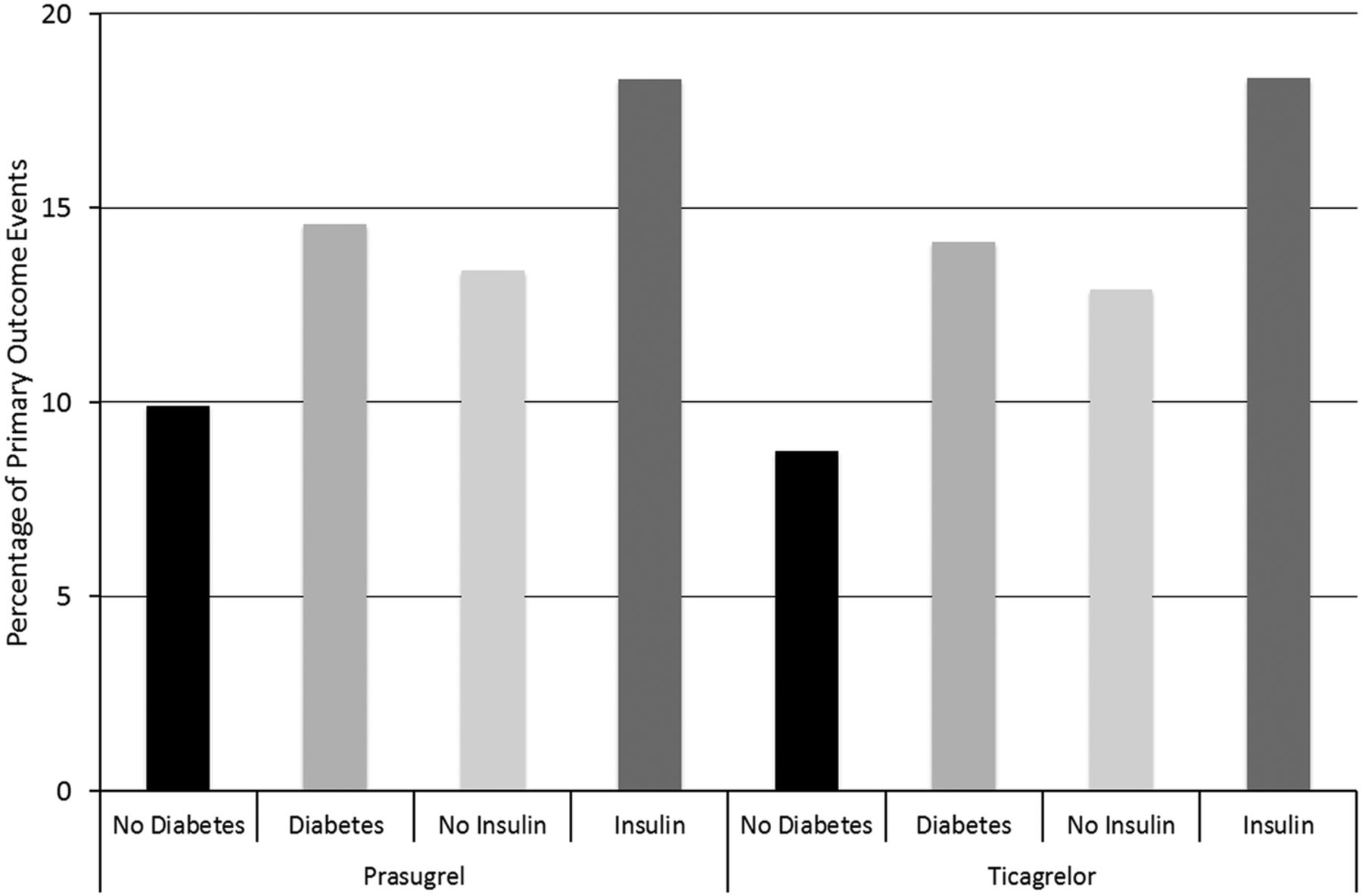
The importance of assessing the population of patients with diabetes in the ACS patient group was highlighted by the universal agreement that patients with diabetes have a worse outcome, notably with the predominant primary composite end point (CV mortality, non-fatal MI and non-fatal CVA)8 ,27 ,29 and MI.27 ,37 Management of patients with diabetes with insulin conferred a worse primary outcome still29 (figure 1). Insulin use is likely to be a surrogate marker for severity of diabetes, as the population with type 1 diabetes will comprise only a minority of these patients. Data from PLATO shows that type 1 diabetes accounted for only 4% of their total population with diabetes.27

Comparison of outcomes in patients with versus patients without diabetes; primary outcome event rate (CV death, non-fatal MI and non-fatal CVA) as a percentage of the population in TRITON-TIMI 38 (prasugrel) and PLATO (ticagrelor) studies, exploring effects of presence of diabetes and nature of management.27 ,29 CV, cardiovascular; CVA, CV accident; MI, myocardial infarction; TIMI, thrombolysis in myocardial infarction.
In the studies that statistically assessed for interaction between patients with and without diabetes, the majority found that there was no significant difference in the overall results.19 ,22 ,27 ,34 The exception to this was TRITON-TIMI 38 which found that the diabetes population had superior benefit from prasugrel compared to clopidogrel in the reduction in fatal/non-fatal (MI; HR 0.60 (95% CI 0.48 to 0.76) (patient with diabetes) versus HR 0.82 (95% CI 0.72 to 0.95) (patients without diabetes (Pinteraction=0.02)), and composite of all-cause death, MI, CVA and major bleed unrelated to CABG (HR 0.74 (95% CI 0.62 to 0.89) versus HR 0.92 (95% CI 0.82 to 1.03 (Pinteraction=0.05)).7 ,29
Clopidogrel versus placebo
In 3122 patients from two randomised studies, treatment with clopidogrel was associated with a significant reduction in CV death, non-fatal MI and non-fatal stroke at 30–360 days (RR 0.84 (95% CI 0.71 to 0.99)). The larger study looked at patients managed both medically and with revascularisation (36.4%),32 whereas the second studied only those undergoing a percutaneous invasive strategy.8 There was no statistical heterogeneity (Q=0.68, p=0.41, I2=0%), so fixed effects were calculated (figure 2).

Clopidogrel versus placebo; risk ratio with 95% CIs for the primary composite end point of CV death, non-fatal MI and non-fatal CVA in the diabetes population comparing clopidogrel versus placebo in addition to aspirin. CV, cardiovascular; CVA, CV accident; MI, myocardial infarction; PCI, percutaneous coronary intervention.
High-dose versus low-dose clopidogrel
In light of the favourable results of clopidogrel versus placebo CURRENT-OASIS 7 looked at 25 086 patients referred for percutaneous coronary intervention (PCI) following presentation with ACS. Patients were assigned either double dose or standard therapy clopidogrel, and high-dose or low-dose aspirin. In the prespecified subgroup of diabetes, there was a non-significant benefit of higher dose clopidogrel in primary composite end point rate (CV death, non-fatal MI and CVA) with RR 0.85 (95% CI 0.69 to 1.05 (p=0.13)).34
Ticagrelor versus clopidogrel
The PLATO study compared ticagrelor and clopidogrel as P2Y12 inhibitor in addition to aspirin in ACS patients managed with and without coronary intervention. The diabetes patient population was a prespecified subgroup that was subsequently analysed showing additional benefit with ticagrelor reducing composite of CV death, non-fatal MI and non-fatal CVA (RR 0.89 (95% CI 0.77 to 1.02) p=0.10) over a 12-month follow-up period.27 Interestingly, compared to the whole study population (RR 0.85 (95% CI 0.78 to 0.92) p=0.0002), the diabetes patient cohort results were not statistically significant.23 Reassuringly, in the patients with diabetes, there was no increased risk of major bleeding as defined by PLATO,27 with RR 0.95 (95% CI 0.81 to 1.10 (p=0.47)).
Prasugrel versus clopidogrel
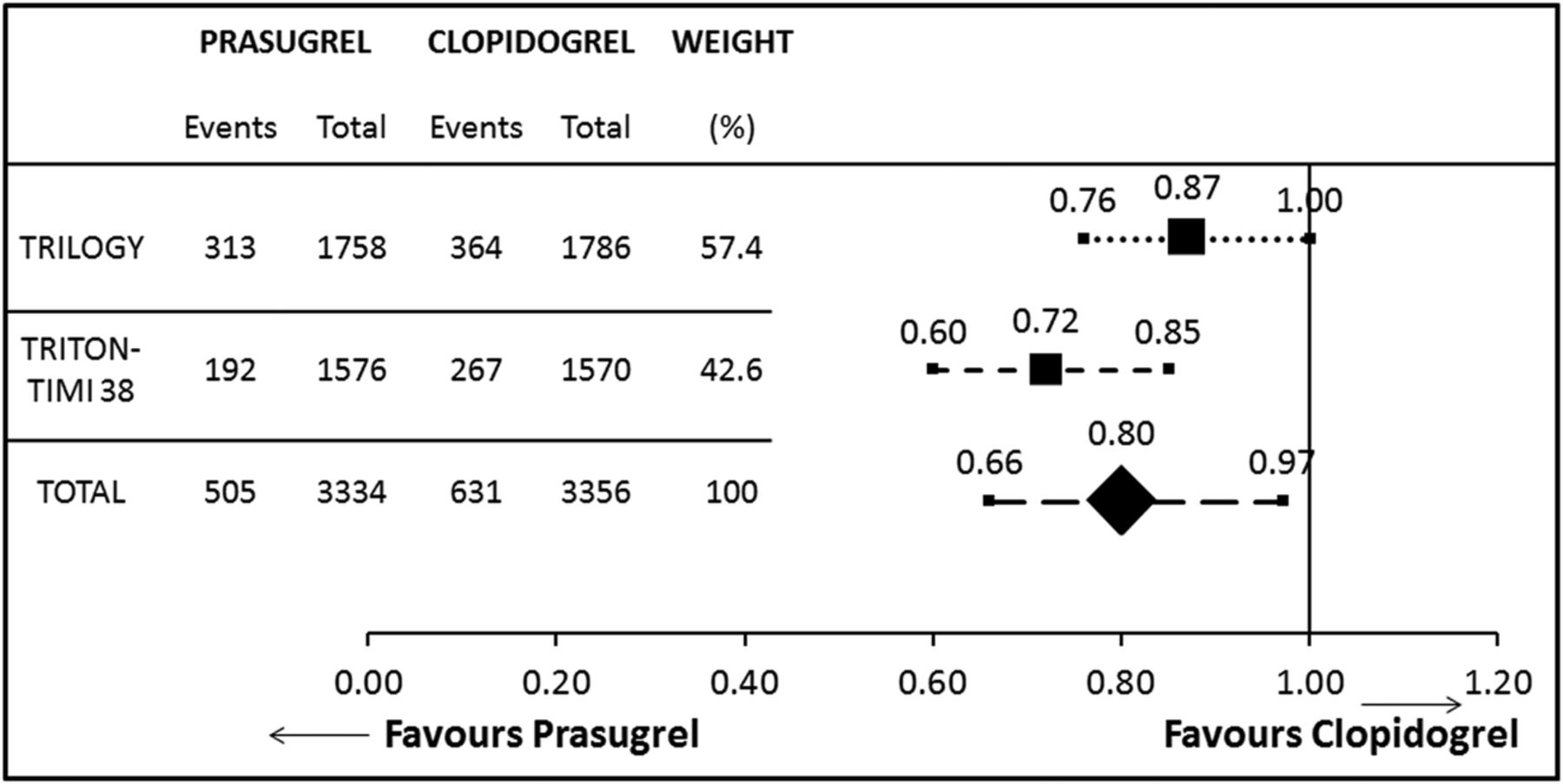
The two studies with prasugrel and clopidogrel as comparators were TRITON-TIMI 38 and TRILOGY,7 ,22 which evaluated the ACS population managed with scheduled PCI and no revascularisation, respectively. A total population of 6690 with diabetes was monitored for events predetermined with the composite primary end point of CV death, non-fatal MI and CVA, for the duration of follow-up (14.5–30 months). Heterogeneity was observed (Q=3.15, p=0.08, I2=68%), so the RR was calculated using the random effects model. The overall effect was in favour of prasugrel in the diabetes patient population RR 0.80 (95% CI 0.66 to 0.97) (figure 3).

Prasugrel versus clopidogrel; risk ratio with 95% CIs for the primary composite end point of cardiovascular death, non-fatal myocardial infarction and non-fatal stroke in the diabetic population comparing prasugrel versus clopidogrel in addition to aspirin.
From the TRITON-TIMI 38 data, we can also elicit benefits of prasugrel over clopidogrel in the population with diabetes, with reduction in MI (RR 0.62 (95% CI 0.50 to 0.76) p≤0.01) and definite/probable stent thrombosis (RR 0.56 (95% CI 0.36 to 0.86) p=0.01) events. This advantage is consolidated in the knowledge there is no increase in major bleeding risk associated (RR 0.95 (95% CI 0.61 to 1.46) p=0.81).29 Interestingly, TRITON-TIMI 38’s outcomes appear better in the diabetes patient cohort compared to the total enrolled population whose RR 0.82 (95% CI 0.74 to 0.91 (p≤0.01)).7
Insulin-dependent diabetes patients versus non-insulin-dependent diabetes patients
Three studies further divided the population with diabetes, categorising by insulin use.27 ,29 ,37 CAPRIE study showed that there was variable response to antiplatelet therapies in the acute setting dependent on the nature of management of the patient. An absolute risk reduction of 3.8% with clopidogrel treatment compared to aspirin therapy in annual event rate for those managed on insulin against 2.1% overall for the population with diabetes.37
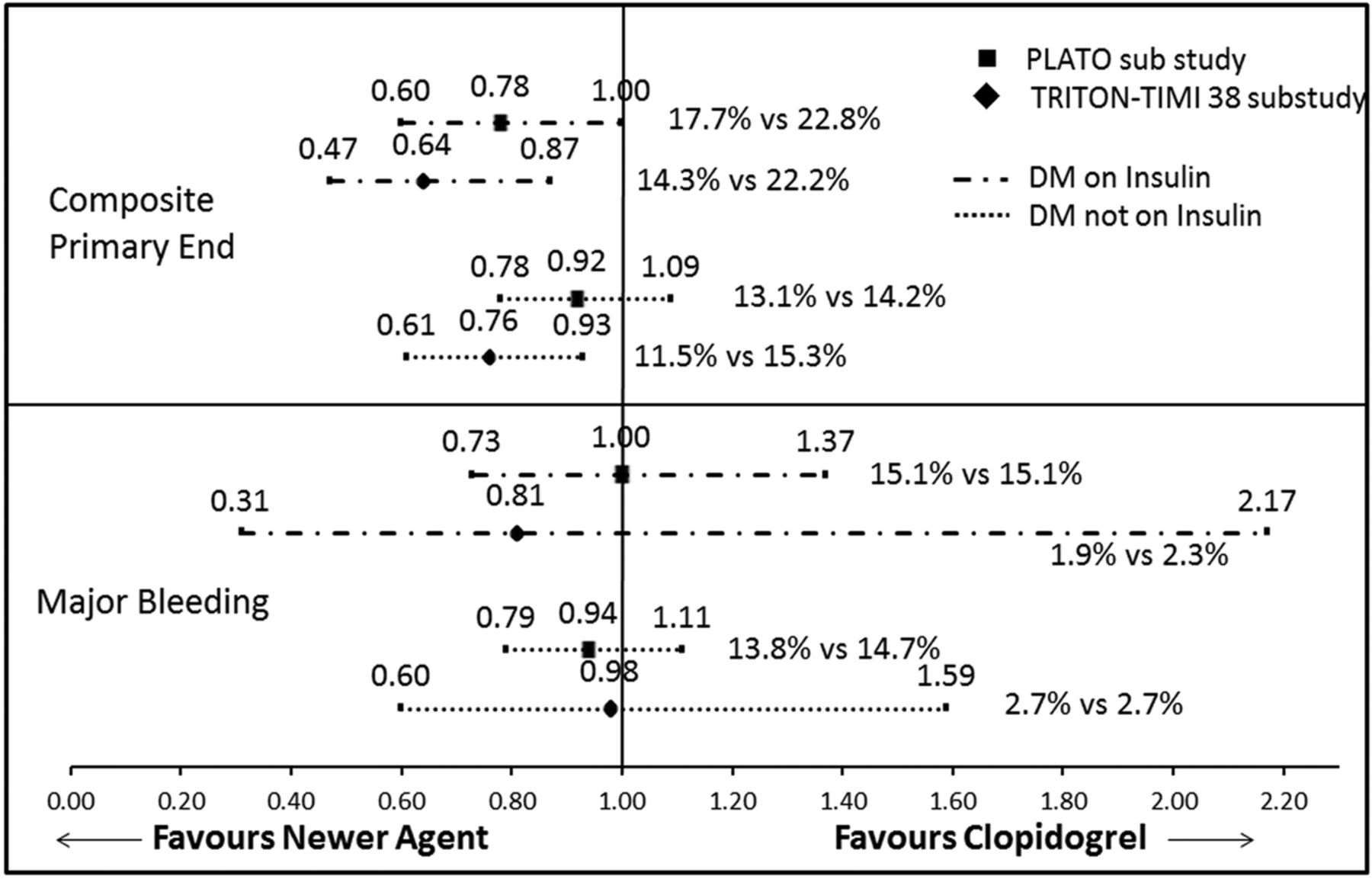
A subsequent analysis has shown that the benefit of the newer P2Y12 inhibitor was more pronounced in the group treated on insulin with a reduction in risk of 36% with prasugrel and 22% with ticagrelor, compared to 24% and 8%, respectively, in the non-insulin treatment arm. However, these were not adequately powered and failed to reach statistical significance (Pinteraction=0.2 for prasugrel and Pinteraction=0.13 for ticagrelor).27 ,29 Reassuringly, there was no increased risk of major bleeding risk in any group, independent of antiplatelet or DM management strategy (figure 4).

Prasugrel and ticagrelor versus clopidogrel; risk ratio with 95% CIs for the primary composite end point of cardiovascular death, non-fatal myocardial infarction and non-fatal stroke. Also, major bleeding in the diabetic populations managed with and without insulin; comparing prasugrel and ticagrelor versus clopidogrel in addition to aspirin. Event rate percentage of newer agent versus clopidogrel. DM, diabetes mellitus.
Indirect comparison
Ticagrelor versus prasugrel
In the diabetes patient population, we were able to indirectly compare a number of outcomes that showed no statistical difference, however, a trend to prasugrel's superiority with regard to the composite primary end point of CV death, non-fatal MI and non-fatal CVA, particularly in the cohort undergoing PCI.27 ,29 ,35 A significant 33% risk reduction in MI events favouring prasugrel was noted. Regarding safety parameters, there was no difference in definite/probable stent thrombosis (RR 1.19 (95% CI 0.58 to 2.45)) or major thrombolysis in myocardial infarction (TIMI) bleeding events (RR 0.94 (95% CI 0.59 to 1.51)) (figure 5).
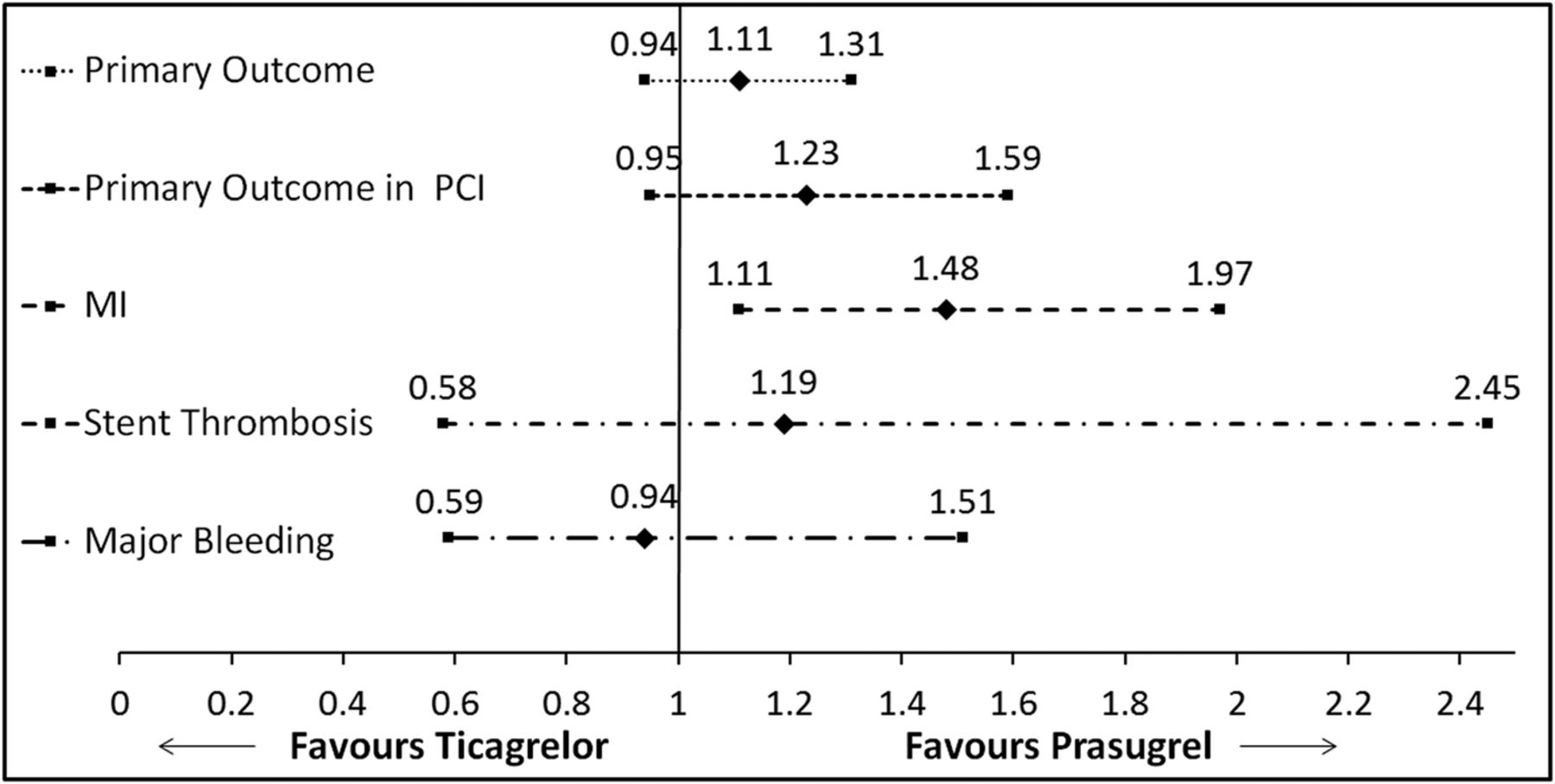
Ticagrelor versus prasugrel; risk ratio with 95% CIs for the primary composite end point, primary composite end point in those undergoing PCI, myocardial infarction, definite/probable stent thrombosis and major bleeding (TIMI classification) in the diabetes population, indirectly comparing ticagrelor versus prasugrel in addition to aspirin. MI, myocardial infarction; PCI, percutaneous coronary intervention; TIMI, thrombolysis in MI.
Newer P2Y12 inhibitor versus placebo
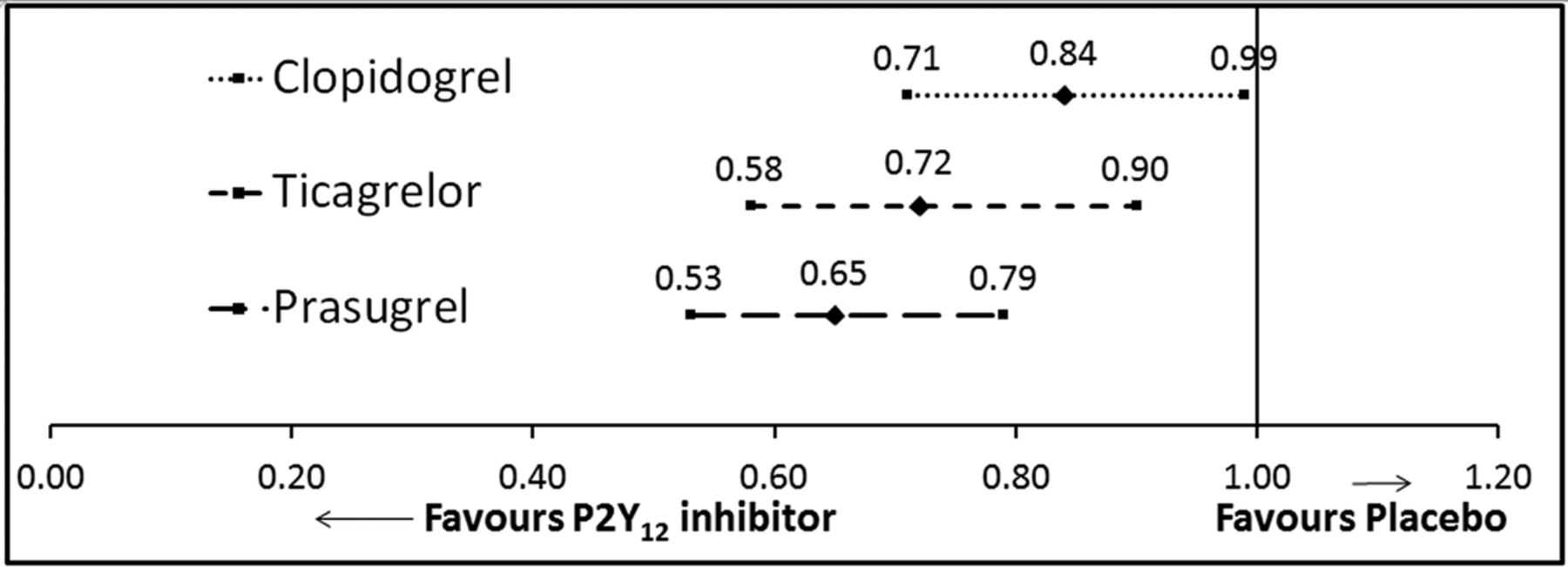
No clinical studies have compared the newer P2Y12 inhibitors to placebo for ethical, clopidogrel in addition to placebo has already been proven to be of significant benefit, and practical reasons, shift to predominant invasive strategy in ACS treatment as stent implantation mandates the use of dual antiplatelet therapy. However, using the indirect comparison method we were able to confirm the superiority of the newer agents against placebo. This showed a marked reduction in the composite end point of cardiovascular death, non-fatal MI and CVA (figure 6). There was further suggestion of prasugrel’s clinical superiority in this population.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
P2Y12 blockade versus placebo; risk ratio with 95% CIs for the primary composite end point of cardiovascular death, non-fatal myocardial infarction and non-fatal stroke in the diabetes population, comparing P2Y12 blockade versus placebo in addition to aspirin.
Discussion
This review shows that all evaluated P2Y12 inhibitors are superior in preventing ischaemic events compared to placebo in diabetic patients with ACS. The newer agents, such as ticagrelor and prasugrel, have a more favourable outcome when directly compared with clopidogrel, although ticagrelor failed to reach statistical significance. This was without an increased risk of bleeding (see online supplementary appendix 3).
Supplementary appendix 3
There may be added value in the cohort managed on insulin, but these results were not powered to reach statistical importance. When indirectly analysed, there is a significant benefit in reduction of events of MI with prasugrel compared with ticagrelor in the diabetes patient group; with a trend to superiority relating to primary clinical outcomes, especially in those undergoing PCI.
Possible mechanisms
The clinical outcomes of patients with diabetes with ACS on clopidogrel monotherapy are superior to those on aspirin.37 It is therefore not surprising that when clopidogrel is combined with aspirin the outcomes are favourable in reduction of ischaemic events, versus placebo with aspirin. Patients with diabetes are more likely to be resistant to aspirin,39 and in addition, have increased P2Y12 receptor signalling.14 Therefore, this cohort may have amplified benefit from the addition of a P2Y12 receptor antagonist to the thromboxane A2 inhibitor aspirin compared to their non-diabetes counterparts.
Patients with diabetes have a higher level of platelet reactivity compared to the non-diabetes population.4 So the search for more potent inhibitors is especially important in this group. We have demonstrated from the analysis, that prasugrel and ticagrelor are superior to both placebo and clopidogrel. Regarding the newer agents versus clopidogrel, these findings are supported by trials of platelet function testing showing increased inhibition of aggregation with less variable response.40 This is likely to be multifactorial, but a large contributory is non-response to clopidogrel. Research shows that depending on method of assessment, 38–44% of patients with diabetes are non-responders to clopidogrel compared to 8–17% of patients without diabetes at 24 h.6 The level of poor response is still apparent at 7 days (24–53%),21 ,40 and is combined with lower levels of circulating active clopidogrel metabolite.21 ,41
Non-response to clopidogrel is a well-documented phenomenon attributed to a number of plausible factors such as increased clearance, reduced absorption altered metabolism to the active clopidogrel metabolite, and higher platelet turnover.3 Also, potential genetic factors have been linked possibly related to the abnormalities in CYP expression in the diabetes patient population.42 However, the predominant mechanism appears to be the abnormal metabolism of clopidogrel within the diabetes patient population rather than dysfunction of the P2Y12 receptor or its signalling pathway, as ex-vivo addition of active metabolite results in almost complete normalisation of response compared to controls.21 ,41
In non-responders, increased on-medication platelet reactivity is significantly correlated to major adverse cardiovascular events (CV death, ACS or stroke), with an increase in event rate from 13.2% to 37.7% at 2 years in patients with diabetes whose level of platelet reactivity is in the upper fourth quartile.43 Concern over non-responders/subresponders led to exploration of high-dose clopidogrel (150 mg) in the patient with diabetes. Although this did significantly reduce platelet aggregation, nonetheless, the majority remained categorised as a subresponder,44 which may explain the lack of statistically important benefit to double-dose clopidogrel in clinical outcomes.34
This has solidified the potential importance of the newer agents, prasugrel and ticagrelor. In the general population, they have been shown to be superior to clopidogrel in suppression of aggregation,20 ,45 ,46 even in those where patients are subjected to double-dose clopidogrel.40 Contributory to this is the reduced requirement of metabolism of prasugrel and ticagrelor, which decreases the time of onset of action and also limits the potential for drug interactions. Ticagrelor itself is a directly acting reversible agent,23 whereas prasugrel, a thienopyridine, requires a single rapid hydrolysation step to active metabolite. Interestingly, higher circulating esterases are found in patients with diabetes,39 which, in theory, would ameliorate this activation step, while inversely it would enhance clopidogrel’s conversion to inactive metabolite.3
The diabetes patient population requiring insulin therapy is trending towards increased benefit from the newer medications. As aforementioned, this represents a marker of severity and duration of diabetes, and functional studies have shown a muted response to clopidogrel in patients treated with insulin compared to oral medication.47 This would suggest that the insulin-dependent group would have added benefit from a more potent P2Y12 inhibitor. Further to this, insulin has been noted in vitro to reduce platelet aggregation by inhibition of the P2Y12 receptor, which, paradoxically, is in agreement with the findings of the review, as patients requiring insulin therapy are those who are most highly resistant to insulin.47
Against the results of this clinical outcome analysis favouring prasugrel are small studies of platelet reactivity testing. These studies have suggested superiority of ticagrelor over prasugrel at 5–30 days48–50 even in the DM-specific population.51 Thirty patients with diabetes undergoing PCI following an admission with ACS were evaluated in a prospective, single-blinded, single-centre crossover study comparing ticagrelor with prasugrel. All patients were preloaded with clopidogrel, and platelet reactivity was tested at days 0, 15 and 30 using VerifyNow P2Y12 functional assay. On day 15, patients were crossed over to the alternative comparator. The authors concluded that ticagrelor achieved a significantly higher level of platelet inhibition compared to prasugrel at 30 days. Possible explanations are the pretreatment with alternative thienopyridine to prasugrel (clopidogrel), although as the authors point out, this is more consistent with clinical practice, and the lack of washout period. Notably, prior to the crossover of patient groups from one comparator to the other, the difference in level of platelet inhibition was not statistically important.51 Does this mean reversible versus non-reversible agents would skew the results? Agreement in the discussion is reached that this is only functional testing, and may not relate to clinical outcomes, particularly as small population functional tests do not per se correlate with large study clinical outcomes.52 It does, however, raise the question of possible alternative pathways unrelated to platelet reactivity being involved. Furthermore, theoretically, ticagrelors’ functional superiority might be at the expense of a higher bleeding risk,48 however, no clinical outcome evidence was found in the analysis to support this.
The variation between the direct functional and indirect clinical findings solidifies the need for a direct comparison study between ticagrelor and prasugrel, with robust clinical and safety end points. We therefore await with great anticipation the results of the ISAR REACT 5 randomised control study,53 which will directly compare ticagrelor and prasugrel in those presenting with ACS undergoing an invasive strategy. The DM population is a clear prespecified subgroup, although patients with DM will be likely under-represented in this invasive study.23
Guidance
ESC and AHA both have clear guidance about antiplatelet management in ACS, with published guidelines for patients presenting with both non-ST elevation ACS (NSTE-ACS) and ST segment elevation MI (STEMI), all supporting the use of P2Y12 blockade in addition to aspirin (Class IA). There is already a move based on results of the landmark trials reviewed towards isolated guidance for patients with diabetes.17 ,54–57
The 2011 ESC guidelines support the preferential use of prasugrel in the diabetes patient population if P2Y12 antagonist naive and due to undergo PCI for NSTE-ACS, assuming patients are not at high risk of life-threatening bleeding.17 ,57 No specific preference is suggested in the STEMI group, where, generally, prasugrel and ticagrelor are favoured over clopidogrel.54
There are differing views in the 2014 ACCF/AHA (American College of Cardiology Foundation) NSTE-ACS guidelines, which state that with regard to antiplatelet therapy, patients with diabetes should be managed identically to the cohort without diabetes. They support the use of clopidogrel or ticagrelor (IB) with preference to ticagrelor, where the patient is undergoing early invasive or ischaemia-guided strategy. Prasugrel is not recommended for upfront therapy in any patient with ACS, unless undergoing PCI, and not at high risk of bleeding.55 In the 2013 ACCF/AHA STEMI guidelines, all P2Y12 inhibitors are given the same level of evidence without preference. But a minor comment is made to consider prasugrel in younger patients with DM with low bleeding risk, ability to continue dual antiplatelet therapy, and no planned surgery in the next year.56
In 2014, the UK National Institute for Health and Care Excellence (NICE) has followed suit with support for prasugrel in the diabetes patients cohort that present with ACS (STEMI and NSTE-ACS included), and who have a planned invasive strategy.58 They determined that in comparison to clopidogrel, prasugrel is judged to be the dominant treatment; as it is not only more effective in reducing subsequent events, it actually costs less than clopidogrel when given to patients with diabetes with NSTE-ACS managed within the UK National Health Service framework.
Our findings support the advice from NICE, and we await future guidelines from AHA/ESC with regard to a more tailored approach to ACS management.
Strengths and limitations
The original studies included in this analysis were large multicentre randomised controlled trials with careful prespecification of the DM subgroup in the majority.7 ,22 ,23 ,34 All the studies were found to have low risk of bias using the Cochrane risk of bias tool detailed in online supplementary appendix 1. However, the analysis is restricted to published literature, all in peer-reviewed journals, but an element of publication bias cannot be excluded. Further papers where we cannot exclude ad hoc subgroup analysis are at risk of statistical error.8 ,19 ,32
The definition of DM is not clearly explored in every study population, which may be open to differing interpretation. Four clearly state previous diagnosis of diabetes was required; however, this was only inferred in others. Only PLATO has analysed data on all participants on the basis of HbA1c which would enable pick up of patients previously undiagnosed with DM, arguably those at highest risk.
Indirect comparison analysis does require homogeneity of those compared, which is supported by the findings of the Cochrane Q statistics observing absence of heterogeneity in the clopidogrel versus control group. Random effects relative risk was required for the combination risk of prasugrel compared to clopidogrel in light of heterogeneity, which needs to be taken into account when considering the primary outcome indirect comparison. However, the remaining outcomes indirectly compared are single-study comparisons with similar design. In the analysis of major bleeding risk, we used results generated from identical scoring schemes (TIMI) to maximise homogeneity.
Conclusions
In patients with diabetes who present with ACS, the addition of a P2Y12 receptor inhibitor is superior to placebo in reducing CV mortality, non-fatal MI and non-fatal CVA without significantly increasing major bleeding events. There is a trend to superiority of prasugrel in this cohort, particularly in those undergoing PCI, without amplified risk of major bleeding. There is a need for the most effective antiplatelet strategy for patients with diabetes to be further explored with dedicated randomised controlled studies.
Acknowledgments
The authors thank Jufen Zhang with her statistical advice, and Dr Sam Xu and Dr Daniel Maruszewski for their help translating non-English retrieved articles.
References
Footnotes
Contributors JAR and OIB designed, searched and extracted data. AH acted a third investigator to judge on any discrepancies between JAR and OIB. All authors contributed to the final written article.
Competing interests JAR and AH have received research grants from AstraZeneca.
Provenance and peer review Not commissioned; externally peer reviewed.