Article Text

Abstract
Background In this pilot feasibility study, we aimed to establish a reproducible means of performing serial optical coherence tomography (OCT) procedures in the abdominal aorta of the cholesterol-fed rabbit.
Methods Eight cholesterol-fed New Zealand White rabbits were assigned to abdominal aortic balloon injury at baseline (n=6) or as controls (n=2). Three of the balloon injured rabbits received statins from weeks 6 to 12 post balloon injury. OCT of the abdominal aorta in each rabbit was performed at baseline±week 6±week 12 via alternate vascular access points (left or right femoral artery or left carotid artery). OCT sequences were analysed to derive an indexed plaque volume and other OCT measures of plaque complexity, and results were compared between groups. Histopathological correlations with OCT images were made following terminal procedures.
Results Of the 16 OCT procedures in these rabbits (6 at baseline, 4 at 6 weeks, 6 at 12 weeks), excellent and analysable images were obtained on 15 occasions (94%). Inability to obtain adequate arterial access for the OCT catheter was the major experimental limitation encountered in the early part of our experience. Balloon injured rabbits developed larger volume and more complex plaque than non-balloon injured rabbits on all OCT indices measured (eg, both mean plaque volume and lumen stenosis were approximately double in the balloon injured group, p<0.0001). A significant correlation between 12 week measures of plaque area by OCT and histology was demonstrated (Pearson correlation coefficient: 0.992, p<0.0001).
Conclusions Our preliminary experience suggests that serial OCT of the abdominal aorta in the New Zealand White rabbit is feasible and a potentially promising means of performing serial studies of aortic atherosclerosis.
- IMAGING AND DIAGNOSTICS
- INTERVENTIONAL CARDIOLOGY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Balloon injury of the abdominal aorta in cholesterol-fed rabbits is a well-validated model for human atherosclerosis. Optical coherence tomography (OCT) is an emerging intravascular imaging technique which provides superior resolution for intravascular ultrasound and allows detailed assessment of plaque characteristics and complexity. To date, the only repeat OCT studies of atherosclerosis in rabbits have involved baseline and preterminal imaging of mostly peripheral vessels. We sought to develop a reproducible technique to perform serial non-fatal OCT studies of the aorta in the same rabbit and compared OCT measures of plaque in rabbits with and without aortic balloon injury.
What does this study add?
Serial OCT imaging of the rabbit aorta is feasible. There are a number of technical considerations in performing non-fatal procedures which we overcame and have outlined to assist researchers in this area. In cholesterol-fed rabbits, balloon injury of the aorta produces significantly more complex plaque on all OCT indices measured compared to no balloon injury.
How might this impact on clinical practice?
This research provides a platform for ongoing rabbit research into anti-atherosclerosis therapies with OCT. It may, therefore, allow the effects of such interventions on plaque characteristics to be carefully examined over time in the same rabbit, providing greater understanding of treatment effects on atherosclerosis.
Introduction
The New Zealand White rabbit provides a valuable model for human atherosclerosis.1 ,2 The species develops hypercholesterolaemia within a few days of dietary supplementation. In this setting, aortic endothelial denudation with balloon injury has been demonstrated to promote atherosclerotic plaque development similar to human lesions, allowing for descriptive and interventional studies aimed at examining plaque size and characterisation.3–5 A major limitation of such studies has been the inability to perform serial analyses in the same animal, as detailed plaque examination has conventionally relied on histology.
Optical coherence tomography (OCT) is an emerging intravascular imaging technique using light waves through a fibre optic core which allows for extremely high-resolution imaging, enabling accurate in vivo plaque characterisation. More recent advances allowing for rapid, non-obstructive luminal imaging have provided a unique opportunity to conduct serial imaging studies investigating the sequence of events during plaque development, and to assess the effects of treatments on plaque morphology and stability.
To date, published studies using the rabbit model for atherosclerosis have been limited to either focal plaque creation and analysis in peripheral vessels (eg, carotid arteries)6 or pre-euthanasia imaging,7 and have not described an approach which allows for serial imaging of aortic plaque pre-intervention and post-intervention. This is likely a reflection of technical obstacles in providing serial images in the aorta, including arterial access, blood clearance for reliable recording of OCT imaging, rabbit handling and survival in the context of multiple procedures. Our aim in this pilot study was to overcome the anticipated difficulties in performing serial OCT of the aorta in rabbits to provide a platform for use by atherosclerosis researchers.
Methods
Eight castrated male New Zealand White rabbits (South Australian Health and Medical Research Institute) aged 3 months were acclimatised on a normal chow diet for at least 2 weeks. One week prior to their first planned OCT procedure, the rabbits were transitioned to a 1% w/w cholesterol diet (Specialty Feeds Australia) which was continued throughout the experimental period.
Rabbits were assigned to one of three treatment arms:
Abdominal aortic balloon injury at week 0 (n=6)
No abdominal aortic balloon injury (n=2).
Of the six balloon injured rabbits, three were given statin treatment from weeks 6 to 12 (atorvastatin 5 mg/kg/day).
OCT imaging of the aorta was scheduled for rabbits at weeks 0 and/or 6 and/or 12.
The intended initial vascular access site for OCT±balloon injury was either the right or left femoral artery. The aim at the second imaging procedure was to use the alternate femoral vessel and then at the final imaging procedure, to catheterise either one of the previously accessed femoral vessels at a more proximal location or to access the left carotid artery.
At the final procedure, rabbits were euthanised and their aortas were removed for histopathological analyses.
All procedures were approved by the University of Sydney Animal Ethics Committee.
OCT and balloon injury protocol
Rabbits were presedated with buprenorphine 100 µg subcutaneously and then placed under general anaesthesia with inhalational isoflurane. The common femoral artery was surgically exposed and after identifying an intended access point, ligated distally and then clamped proximally. A small quantity (total <1 mL) of glyceryl trinitrate (100 µg/mL) was administered topically to the vessel to assist in dilatation. A small arteriotomy incision was made and the tip of a 4F 10 cm Terumo sheath (Radifocus Introducer II; RS+B40K10MR) was inserted. The proximal vessel clamp was removed and the sheath inserted 2–3 cm into the vessel after establishing that intraluminal access had been achieved. The sheath was secured with a suture around the vessel and injected with 3 mL of diluted heparinised saline (1 unit/mL). A 0.018″ interventional wire was inserted ∼35 cm.
For rabbits assigned to abdominal aortic balloon injury at baseline, a 3F Edwards Fogarty Arterial Embolectomy catheter was inserted over the interventional wire to the embolectomy catheter's 30 cm marker, corresponding to a position roughly 12–15 cm above the iliac bifurcation. The balloon was inflated with 0.2 mL saline and gently retracted ∼12 cm. The balloon was then deflated and the catheter readvanced 12 cm, with two additional cycles of inflation and retraction performed before the catheter was removed.
For OCT imaging, a St Jude C7 Dragonfly OCT catheter (St Jude Medical) was inserted over the guidewire through the sheath to the silver/black junction on the OCT catheter—a distance of 28 cm. In practical terms, this distance corresponds to about 10 cm above the iliac bifurcation, influenced mainly by the length of Terumo sheath outside the femoral vessel. After preparing the OCT console (St Jude Medical) for manual injection, 15 mL of normal saline was firmly injected through the side port of the 4F sheath with simultaneous activation of the imaging sequence. The OCT catheter was then pulled back 5 cm and another imaging sequence was performed. These two sequences typically yielded images over a 10 cm abdominal aortic segment from around the renal artery bifurcations to the iliac bifurcation, with a ∼1 cm overlap between sequences. For rabbit safety, no more than three fluid boluses for OCT clearance were attempted in live rabbits, irrespective of the image quality obtained.
In non-fatal procedures, after the imaging sequences were completed, the catheter, wire and sheath were removed and the femoral artery ligated at a point immediately proximal to the arteriotomy site, followed by wound closure.
For procedures involving left carotid artery access, a similar access and OCT imaging process was followed. The length from the aortic arch to the abdominal aorta is roughly the same as the length from the abdominal aorta to the iliac bifurcation (∼10 cm), requiring an additional 5 cm advancement to image the same initial anatomical region described above.
For week 12 procedures, a combination of pre-euthanasia and post-euthanasia OCT imaging was performed, but the presented data analyses were conducted, unless otherwise stated, on the post-euthanasia series only.
OCT image analyses
Calibration
Image series were reviewed and common aortic branches were identified by frame position, allowing identifiable unique segments of multiple OCT series to be analysed. This allowed a total aortic segment length to be defined, and also ensured similar aortic segments were being compared serially in the same rabbit. For uniformity, only aortic segments ranging from the coeliac artery proximally to the iliac bifurcation distally were included in quantitative analyses.
Measurements
For each aortic segment analysed, every 10th frame (0.2 to 0.25 mm—according to OCT console resolution setting) had the following measurements recorded:
Lumen area (mm2)
Lumen+intima and media (IM) area (mm2)—defined by a border representing the junction between the media and adventitia
Maximal lumen diameter (mm)
Minimal lumen diameter (mm)
Maximal IM thickness (mm)
Minimal IM thickness (mm).
In cases where image artefact prevented adequate analyses for a given frame, the nearest frame with appropriate clarity was used. Segments with artefact extending more than 15 consecutive frames were excluded from the analyses.
These measurements allowed the following values to be derived:
Indexed plaque volume (mm3/mm)
Plaque volume was derived using the areas of plaque measured on each OCT frame and the distance these were separated (0.2–0.25 mm), summed across the total distance of aorta measured and then indexed for comparison between rabbits or time periods. This is a novel measurement we used to examine overall plaque burden over a continuous aortic segment.
In more detail, the volume between two analysed frames was calculated using the common formula deriving volume from two different cross-sectional areas (A1 and A2) at a given height (h):
 Volumes of plaque were derived by subtracting the volume between two sequential Lumen area measurements from the volume between two ‘Lumen+IM’ area measurements. The sum of all the volumes calculated between each OCT frame was indexed by the length of segment imaged, producing a volume per mm.
Volumes of plaque were derived by subtracting the volume between two sequential Lumen area measurements from the volume between two ‘Lumen+IM’ area measurements. The sum of all the volumes calculated between each OCT frame was indexed by the length of segment imaged, producing a volume per mm.
Modified lumen stenosis (%)
Defined as (‘Lumen+IM Area’−‘Lumen Area’)/‘Lumen+IM Area’×100 and expressed as a mean of all analysed frames
Mean maximal IM thickness (mm)
Mean lumen eccentricity
A mean of the ratio: (maximal lumen diameter−minimal lumen diameter)/maximal lumen diameter derived for each analysed frame
Mean plaque eccentricity
A mean of the ratio: (‘Maximum IM thickness’−‘Minimal IM thickness’)/‘Maximum IM’ derived for each analysed frame.

OCT measurements were performed by investigators blinded to treatment allocation.
Histological analyses
Aortas were stored in a 10% formalin solution until histological preparation. For each rabbit, five aortic segments evenly spaced between the subclavian artery and iliac bifurcation were fixed in paraffin oil and representative slices from each segment were stained with H&E. For each cross-sectional aortic slice, the plaque area was calculated by manually tracing the luminal border and the border of the EEM. Histological analyses were performed using Image Pro-Premier 9.1 (Media Cybernetics). Slices were matched with OCT images (where available) by examination of OCT images in the region from which the aortic slice was obtained for a match. Only definitively matched cross sections were used for correlation.
Statistical analyses
Comparisons between OCT plaque areas and histological plaque areas were made using a bivariate Pearson correlation coefficient with a two-tailed test of significance. Mean OCT measurements at 12 weeks were compared in balloon injured versus control rabbits by independent two-tailed t tests. In an exploratory analysis, mean OCT measurements for statin treated and non-statin treated balloon injured rabbits were compared using independent two-tailed t tests at weeks 6 and 12. Statistical significance was inferred at p<0.05. Analyses were performed using IBM SPSS Statistics V.22.
Results
Of eight cholesterol-fed rabbits, six underwent baseline aortic balloon injury, and five had adequate baseline OCT imaging for analyses. Four had successful OCT imaging at week 6. Two rabbits with balloon injury were euthanised between weeks 6 and 8; one suffered acute leg paralysis from a non-experiment related twisting spinal cord injury, and the other suffered a suspected myocardial infarction likely related to large ruptured aortic root plaque seen on autopsy. All six remaining rabbits had OCT imaging at week 12 (table 1).
Rabbit treatment allocation and OCT aortic segment lengths analysed
Inability to obtain adequate arterial access for the OCT catheter was the major experimental limitation encountered in the early part of our experience. Thus, arterial access was unable to be obtained in 7 of our first 16 attempts but was uniformly successful in all six rabbits studied at the 12-week time point, consistent with a ‘learning curve’ for this technique.
Compared to control rabbits, those with aortic balloon injury at week 12 had a significantly higher indexed plaque volume, mean lumen stenosis, mean maximal IM thickness, plaque eccentricity and lumen eccentricity (all p≤0.001; table 2).
Aortic OCT analyses at week 12, subdivided by balloon injury status
Among balloon injured rabbits, those treated with statin therapy from weeks 6 to 12 had a lower indexed plaque volume at week 12, despite similar measures at baseline and week 6 (week 12 mean difference −0.79 mm3/mm, 95% CI −0.48 to −1.10, p<0.0001) (see online supplementary figure 1).
Eighteen aortic cross-sectional slices spaced intermittently between the aortic arch and iliac bifurcation among six rabbits were matched with OCT images for histological correlation. Comparisons of total plaque area between OCT and histology cross-sections demonstrated a highly significant correlation (Pearson correlation coefficient: 0.992, p<0.0001) (figures 1 and 2).
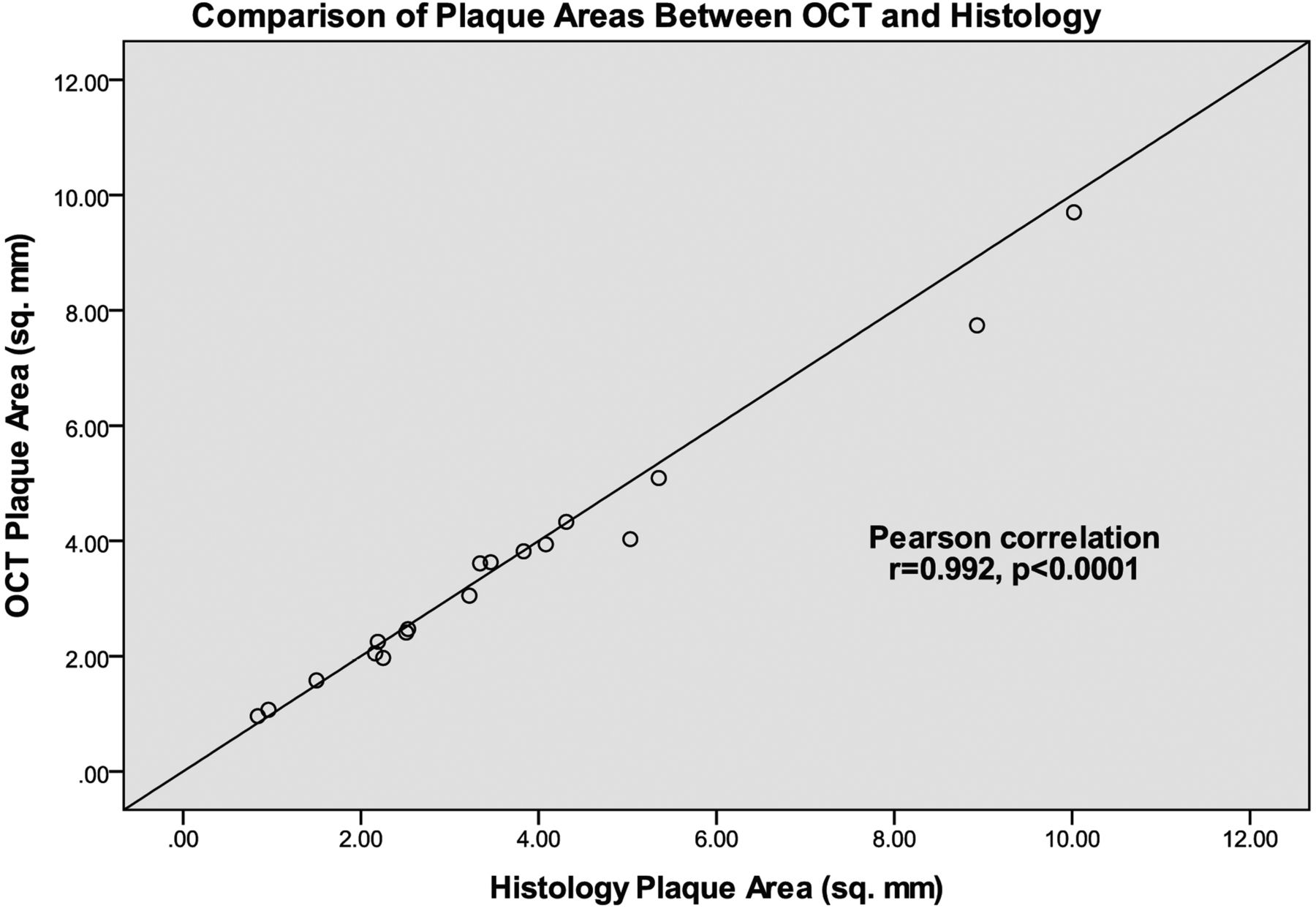
Comparison of plaque areas measured from OCT and histology images. OCT, optical coherence tomography.

{kind=link}
{kind=link}
Examples of matched OCT and histology images. OCT, optical coherence tomography.
Discussion
OCT has emerged as an increasingly popular high-resolution intravascular imaging modality, and we have presented a practical approach to allow effective in vivo abdominal aortic imaging and image analyses in the New Zealand White rabbit. We have also presented preliminary data demonstrating rapid plaque formation achieved with aortic balloon injury in the cholesterol-fed rabbit, and the feasibility of serial aortic imaging studies in this in vivo model of progressive atherosclerosis.
OCT procedure
This study is the first published research describing an approach to serial OCT imaging of the aorta in the New Zealand White rabbit. Several previous studies have described carotid artery or iliac OCT imaging,6 ,8 ,9 but serial imaging in the same animal has only rarely been reported.10 The aorta is a site of particular interest as it is the first site of development of plaque in children and young adult humans.11 Abdominal aortic intravascular imaging (using OCT and or other modalities) has only to date been described as a preterminal technique.7 ,12–14
The methods described here were, therefore, derived through case-by-case experiences and unearthed a number of practical issues which may help guide future researchers in this area.
Saline is a better ‘blood clearing’ agent than iodinated contrast in the rabbit. While teratogenicity studies in rabbits report safety in administering iodinated contrast up to 2.5 g iodine/kg, the volumes required for blood clearance for OCT with this technique are not substantially different to human volumes despite obvious differences in body size. Standard non-ionic contrast (eg, iohexol 370 mg/mL) would typically expose a rabbit (noting an average weight of 2.0–3.5 kg) to 5.5 g per 15 mL injection. Two recent studies involving administration of a 6 mL/kg intravenous dose of iopamidol (370 mg iodine/mL) to rabbits examined effects on renal function using MR renography and functional MRI, and both demonstrated marked impairment of renal function occurring immediately15 and persisting at 72 h, without any impact from an equivalent injection of isotonic saline.16 In addition to these nephrotoxic risks, in practice we consistently observed acute haemodynamic reactions to smaller boluses of 10 mL of iohexol 370 mg/mL, even when diluted 50:50 with saline. These typically included a profound, transient bradycardia and loss of perfusion consistent with hypotension. Effects appeared to resolve over 20–30 s and we experienced no acute fatalities; however, on balance, boluses with iodinated contrast do not appear safe at the volumes required for aortic OCT.
There is limited information available clarifying a safe fluid bolus volume to administer to a rabbit in the absence of shock or dehydration. In our experience, the administration of 2–3 manually administered boluses of 15 mL of isotonic saline for OCT clearance, after factoring in blood collection, operative losses and postoperative anorexia, was well tolerated. The approximate total blood volume of a rabbit is 7% of body weight,17 corresponding to 210 mL in a 3 kg rabbit. Daily fluid maintenance requirements are proportionally higher than in humans at 75–100 mL/kg,18 and in the setting of dehydration or shock suggested isotonic fluid boluses can range from 1019 to 100 mL/kg.18
High quality OCT imaging of the thoracic aorta via the femoral artery is difficult due to mixing of antegrade blood from cardiac output with the retrograde saline injection. Even greater difficulty in blood clearing, however, is experienced using carotid access to the thoracic and abdominal aorta, rendering antegrade aortic access for OCT imaging in a live animal extremely difficult. It is possible that the use of a larger sheath inserted more distally might allow for in vivo carotid imaging; otherwise, this vascular approach should be reserved for terminal experiments.
As expected, repeat access of a previously used femoral vessel is difficult and related to factors such as postoperative scarring. While not impossible, it would generally be preferable and more efficient to use a different vessel on each occasion, with additional options of iliac artery or carotid artery access for the terminal procedure.
OCT analyses
The aortic balloon injury model for atherosclerosis mostly creates diffuse, concentric, generalised plaque, rather than focal, eccentric lesions. This requires additional considerations when approaching OCT analyses.
The capacity to orientate multiple OCT series to define a continuous aortic segment for analysis is important. While studies detailing the anatomy of the rabbit aorta are limited, we found anatomical research by Ahasan et al20 a useful guide to the aortic lengths and branches that allow for the specific region imaged by a series to be accurately defined and to identify landmarks for potential use in aligning other series together, as well as for ascertaining histopathological correlations.
OCT consensus standards for image analyses continue to be updated by the International Working Group for Intravascular Coherence Tomography Standardisation and Validation.21 We performed their described quantitative analyses of lumen (cross-sectional) area, minimum lumen diameter, maximum lumen diameter and lumen eccentricity. Due to well acknowledged limitations in consistently defining the internal elastic lamina in rabbit OCT imaging, we substituted this border for the external elastic lamina (EEM, on the outer border of the tunica media) which was more clearly demarcated to perform measurements of plaque (cross-sectional) area, modified lumen stenosis, maximum plaque thickness, minimum plaque thickness and plaque eccentricity. In view of the extensive plaque created, we also derived a novel ‘Indexed Plaque Volume’ measurement which allowed for an accurate determination of total atherosclerotic load for comparisons over time and between different rabbits. The correlation between OCT images and histopathology has already been well validated10 and while we, therefore, did not seek to comprehensively examine this, our random analyses of plaque area between different rabbits and aortic segments by OCT and histopathology showed a highly significant correlation.
While it is acknowledged that OCT imaging has a limited tissue penetration depth of 2–3 mm,22 the maximal ‘plaque’ (IM) thickness we recorded was 1.05 mm, supporting the fact that such technical limitations did not in most instances impede the reliability of our measurements, and that measurements of plaque volume and thickness in this animal model are feasible with OCT alone. Large calcium deposits or long segments of thrombus attached to a ruptured plaque were individual instances where OCT measurements underestimated results compared to histology measurements.
We did identify marked differences in lumen area in OCT analyses performed after euthanasia compared to before, undoubtedly reflecting the impact of blood pressure on lumen size. While it is, therefore, preferable to conduct all imaging for serial analyses in live animals, substantially greater lengths of aorta could be imaged immediately after euthanasia. Differences in plaque thickness were much smaller and in plaque area were equivalent between pre-euthanasia and post-euthanasia imaging despite differences in lumen area. Since the longest and best quality aortic segments were imaged post-euthanasia in these experiments, we did not seek to compare changes in lumen area over time.
Experimental findings
The value of aortic balloon injury in New Zealand White rabbits as a model for atherosclerosis has long been recognised, and our findings of significantly greater plaque volumes, thickness and eccentricity and smaller mean lumen stenosis by 12 weeks in balloon injured cholesterol-fed rabbits compared to cholesterol-fed rabbits alone was not unexpected. In fact, aside from mild increases in generalised vessel wall thickness over 12 weeks, the only definitive evidence of plaque formation in cholesterol-fed rabbits was the presence of occasional small fibrous plaques, typically around the branch vessels. By contrast, balloon injured cholesterol-fed rabbits had long segments of irregular concentric plaque as well as occasional rupture (see online supplementary figure S2).
In a very small ‘proof of concept’ subset of two rabbits, statin therapy from weeks 6 to 12 appeared to slow plaque growth in the balloon injured cholesterol-fed rabbits. To maintain methodological consistency, statin-fed rabbits continued their high-cholesterol diet, creating an environment with both pro-atherosclerotic and anti-atherosclerotic forces. However, statin therapy appeared to substantially impact on these processes, resulting in significantly less plaque at week 12 than in the non-statin treated balloon injured rabbits. We must emphasise, however, the preliminary nature of these findings.
Analyses of atherosclerosis in the rabbit balloon injury model have frequently focused on characterising individual plaque features (or by counting plaques), while the endothelial denudation associated with balloon injury typically creates long continuous segments of atherosclerosis. For this reason, analyses performed on multiple OCT frames over a given segment length in this model may better characterise the overall disease burden as well as the effects of systemic treatments.
The demonstration of changes in plaque size after balloon injury therapy using serial OCT measurement in a rabbit model has important implications for preclinical studies of atherosclerotic progression. We have reported the ability to detect small changes using high-resolution imaging of the artery wall. This is of great relevance in a cholesterol-fed animal model, in which the pathology generated is typically concentric, but relatively modest in size. The findings suggest that OCT may be superior to intravascular ultrasound imaging, the use of which is not great in animal studies. The advantage in animal models is also supported by the thickness of the artery wall in rabbits, permitting reliable visualisation of the outer vessel wall on OCT. This is not considered to be the case in humans, where penetration limits often preclude reliable measurements of plaque burden. As a result, increasing interest in the use of OCT in humans has focused on its ability to visualise superficial features consistent with plaque vulnerability such as fibrous cap thickness, lipid pools, spotty calcification and microchannel formation.23 Though we did not investigate these features in our study, they have been the subject of other recent rabbit OCT research;10 hence, the potential for OCT to examine both superficial plaque characteristics as well as overall atherosclerotic burden with this model is promising.
Conclusion
We have established a practical guide to allow the conduct of serial non-fatal abdominal aortic OCT in New Zealand White rabbits. Aortic balloon injury was associated with steady progression of OCT measures of plaque volume and complexity over time. This provides a potential model for future OCT research into the effects of novel anti-atherosclerotic therapies over time.
Acknowledgments
The authors thank Kim Hewitt, Melinda King-Adams, Ying Teng, Cathy Yates and Manuel Menouhos.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online figures
Footnotes
Contributors JF, SP and DC conceived and designed the research. JF, SB and SP performed the animal procedures. JF and SB performed aortic histology. JF, SP, SN and DC analysed the data. JF, SP, SN, SB and DC wrote the manuscript.
Funding The study was funded by a research grant from the National Health and Medical Research Council, Australia. The sponsor played no role in study design, data collection, data analysis, manuscript preparation or manuscript submission.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
Data sharing statement Results for analyses of OCT frames may be made available, specific to the request, by contacting the senior author by email: david.celermajer@email.cs.nsw.gov.au