Article Text

Abstract
Objective Myocardial fibrosis related to non-specific inflammation can be detected using late gadolinium-enhancement cardiovascular MR (LGE-CMR), which is an important prognostic indicator for dilated cardiomyopathy (DCM). The aims of this study were to define the prognostic factors for DCM with LGE-CMR, and to evaluate the impact of the prognostic factors on adverse effects.
Methods We performed a retrospective analysis of a prospectively maintained single centre registry. We analysed the data from 76 patients with DCM who had been admitted for acute heart failure. The primary combined end point was defined as all-cause mortality and rehospitalisation.
Results LGE-CMR was present in 39 patients (51%), and the mean follow-up period was 813±54 days. The primary end point occurred in 20 patients (5 (13.5%) patients without LGE-CMR and 15 (38.5%) patients with LGE-CMR, p=0.006). Sixteen of 39 patients with LGE-CMR exhibited elevated high-sensitivity C reactive protein (hs-CRP >0.3 mg/dL). Patients with elevated hs-CRP and LGE-CMR had a significantly higher incidence of the primary end point compared with patients with normal hs-CRP and LGE-CMR (62.5%; 10 patients, 22.7%; 5 patients, respectively, p=0.001). Elevated hs-CRP was significantly associated with the primary end point (HR: 4.04; 95% CI 1.67 to 9.76; p=0.002). After elevated hs-CRP was adjusted for known predictors of DCM, it was still associated with the primary end point (HR: 2.91; 95% CI 1.19 to 7.15; p=0.02).
Conclusions Among patients with DCM, LGE-CMR and elevated hs-CRP are associated with a higher incidence of the long-term combined end point of all-cause mortality and hospitalisation.
Trial registration number: UMIN000001171.
- HEART FAILURE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Dilated cardiomyopathy (DCM) with late gadolinium-enhancement cardiovascular MR (LGE-CMR) has a significant relationship with mortality and rehospitalisation.
What does this study add?
In these patients, prolonged elevation of high-sensitivity C reactive protein (hs-CRP) at stable state was the strongest predictor of adverse events during long-term follow-up.
How might this impact on clinical practice?
This is the first clinical study to evaluate a complementary role by LGE-CMR and hs-CRP in the risk-stratification of patients with DCM after acute decompensation.
Dilated cardiomyopathy (DCM) is a common phenotype of cardiomyopathy, with a prevalence of approximately 1 in 2500 patients.1 Outcomes are generally adverse, and the 10-year mortality remains over 40%, despite advances in medical devices and pharmacotherapy.2 Therefore, precise risk stratification is necessary, and various imaging and serological techniques have been implemented for this purpose.
Myocardial fibrosis related to non-specific inflammation is an important prognostic indicator for DCM and can be detected using late gadolinium-enhancement cardiovascular MRI (LGE-CMR).3 As a serological marker, C reactive protein (CRP) has emerged as an important biomarker of inflammation. Recently, elevated high-sensitivity CRP (hs-CRP) has been shown to indicate low-grade inflammation and might contribute to the risk stratification of patients with DCM.4
The purpose of this study was to define the prognostic factors for patients with DCM with LGE-CMR after hospitalisation, and to evaluate the impact of these prognostic factors on adverse effects. As a serological marker of inflammation, elevated hs-CRP was used to complement LGE-CMR, in the hope that it would facilitate precise risk stratification and differentiate patients with DCM with ongoing inflammation.
Methods
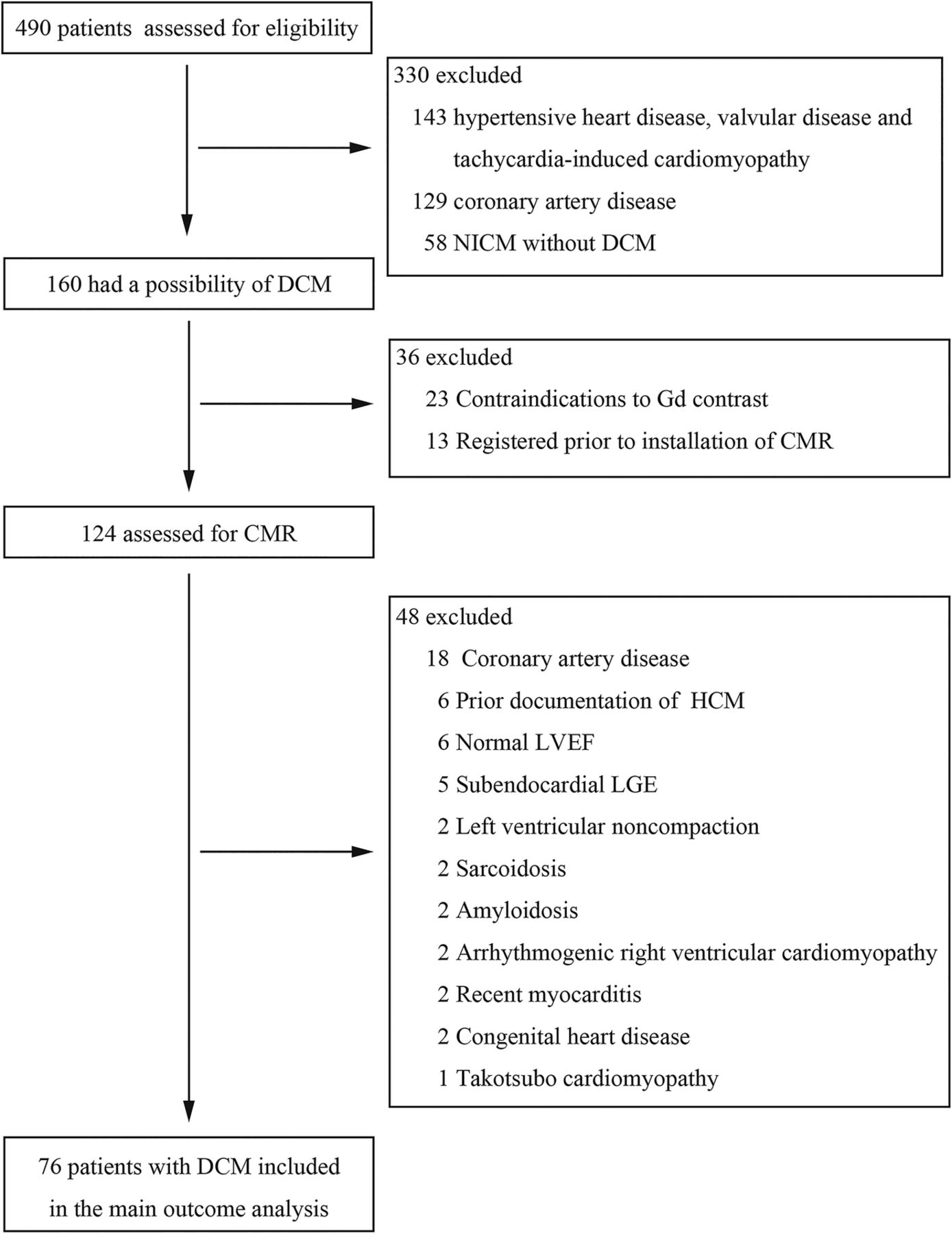
We performed a retrospective analysis of patient records from a prospectively maintained registry of patients admitted to the Keio University Hospital. Patients are enrolled in the database at the time of their admission for acute heart failure (AHF), which is diagnosed according to the Framingham criteria. Our analysis spanned all records for patients admitted between January 2006 and September 2013. Four hundred and ninety patients with AHF were assessed for eligibility, and 160 patients (32.6%) were suspected to have DCM. Of these patients, 36 were excluded due to contraindication of gadolinium contrast medium, or registration prior to the installation of CMR at our facility. CMR was performed on 124 patients (25.3%) during the study period.
For the present study, DCM was defined as echocardiographic evidence of unexplained dilation of the left ventricle (LV) (ie, LV diastolic dimension >55 mm) and impaired contraction (ie, LV ejection fraction (LVEF) <45%), without the presence of obstruction coronary disease. All patients with DCM underwent coronary angiography and cardiac biopsy to rule out obstructive coronary disease and infiltrative cardiac disease. Exclusion criteria for our analysis were the presence of other cardiomyopathy, myocarditis, significant valvular disease or contraindications for LGE-CMR. Patients with presumed DCM and LGE-CMR in distributions other than the mid-wall (eg, subepicardial, epicardial or patchy) were also excluded. Using these criteria, 48 patients were excluded from our analysis due to coronary artery disease (n=18), other cardiomyopathy (n=15), normal LVEF (n=6), non-mid-wall LGE-CMR (n=5), congenital heart disease (n=2) and myocarditis (n=2). The final study population consisted of 76 patients (figure 1). The majority of CMR was performed during the index acute heart failure hospitalisation of our patients (median, 10.X days; IQR 4.X–14.X days).

Derivation of the study cohort. CMR, cardiovascular MR; DCM, dilated cardiomyopathy; EF, ejection fraction; Gd,gadolinium; HCM, hypertrophic cardiomyopathy; LGE, late gadolinium enhancement; LV, left ventricular; NICM, non-ischaemic cardiomyopathy.
Informed consent was obtained from each patient included in the registry, and informed written consent was obtained from all participants in this study. The study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki, and was approved by the Institutional Review Board of the Keio University School of Medicine.
All images were acquired using electrocardiographic gating on a 1.5-T scanner, with the patient in a supine position and holding their breath. LGE-CMR were acquired 10 min after intravenous injection of 0.1 mg/kg body weight gadodiamide hydrate. Inversion times were chosen to null normal myocardium. To exclude artefacts, images were repeated in two separate phase encoding directions. The presence of mid-wall LGE-CMR was evaluated by an independent expert cardiologist and radiologist, and an example of DCM with LGE-CMR is shown in figure 2.
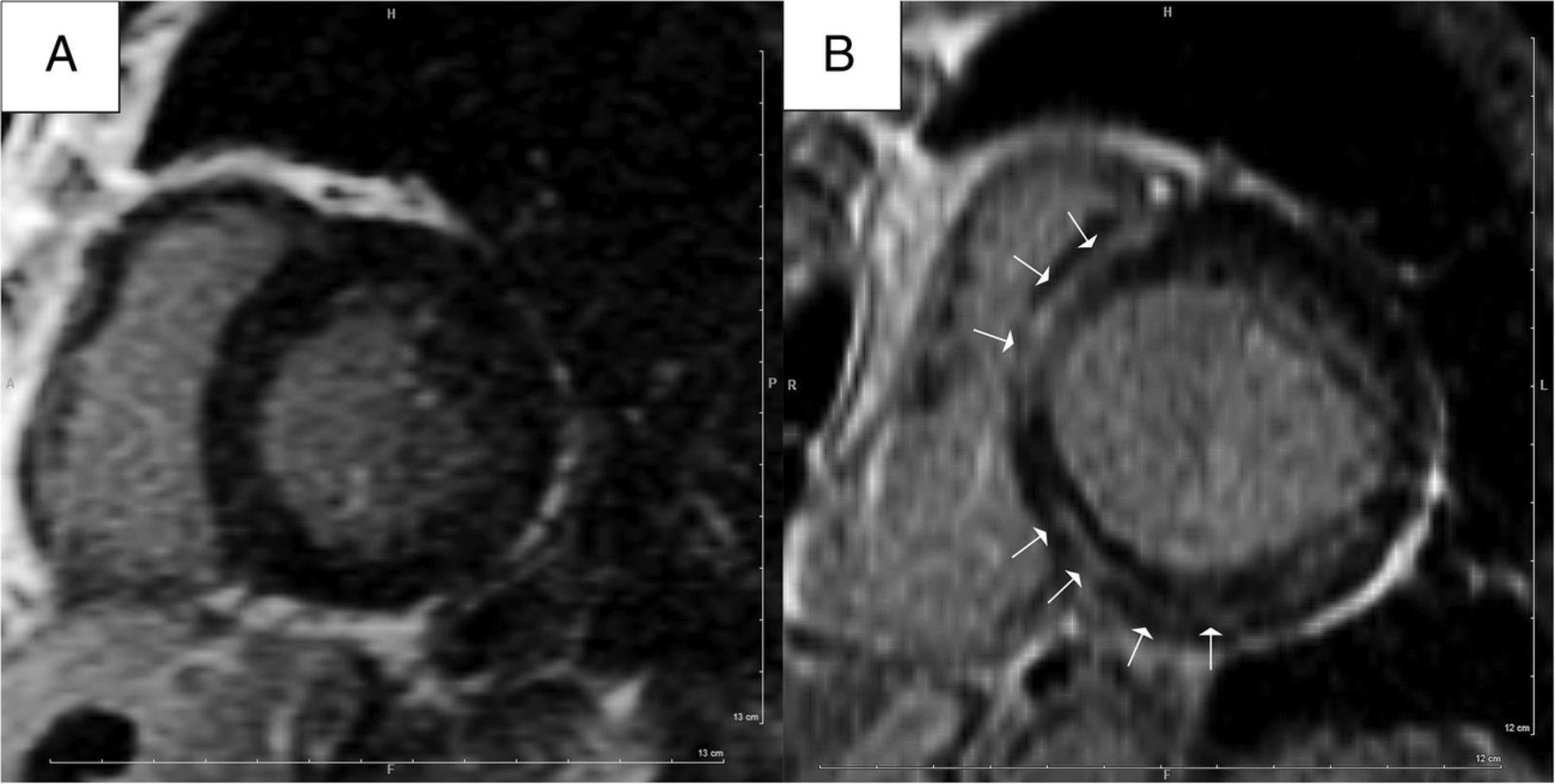
Representative late gadolinium enhancement (LGE) images. Images were obtained on a short-axis slice, and compare a patient without LGE (A) with a patient with mid-wall LGE (B), as seen in the dilated cardiomyopathy. White arrows indicate areas of LGE.
Blood samples were obtained on the day of admission, and repeated at stable state during the first follow-up appointment. Plasma B-type natriuretic peptide (BNP) levels were measured using a commercially available assay kit (Shionogi, Tokyo, Japan). Patients’ hs-CRP levels were measured using a commercially available assay kit (Mitsubishi, Tokyo, Japan), with a lower limit of detection of 0.01 ng/mL.
All patients were directly observed by their cardiologists, or followed up by telephone. The primary end point was a composite of all-cause mortality and hospitalisation for a cardiovascular event. The cause of death was identified in all cases, and cardiovascular death was defined as death preceded by signs or symptoms of heart failure or documented ventricular arrhythmia.
Baseline characteristics were compared between patients with LGE-CMR and those without. Continuous variables were expressed as mean±SD unless otherwise specified. Categorical variables were expressed as absolute values and percentages. The unpaired two-sample t test was used to compare the means of continuous variables. The Pearson χ2 test was used to compare categorical variables. Event curves were determined using the Kaplan-Meier method, and mortality rates were compared using the log-rank test. Univariate and multivariate Cox proportional hazards models were used to calculate HR and the 95% CIs (95% CI). All tests were two-sided, and results were considered to be statistically significant at a p value <0.05. All statistical analyses were performed using SPSS V.21.0 (SPSS Inc, Chicago, Illinois, USA).
Results
After exclusions, 76 patients were included in our analysis, and their characteristics are summarised in table 1. The mean follow-up period was 813±54 days, and no patients were lost to follow-up. In the study population, LGE-CMR was present in 39 patients (51%). As seen in table 1, patients with LGE-CMR had lower systolic and diastolic blood pressure and required longer hospitalisation compared with patients without LGE-CMR. LVEF and left ventricle stroke volume were significantly higher among patients without LGE-CMR. No significant differences were observed in the medication being taken at baseline, device implantation rate or the laboratory test results.
Characteristics of all patients, stratified by the presence or absence of LGE
Elevated hs-CRP levels were detected at baseline and subsequently declined to a stable state (table 1). Patients with LGE-CMR were stratified according to their levels of hs-CRP, and 16 of 39 patients with LGE-CMR (41%) exhibited hs-CRP elevation over 0.3 mg/dL at stable state. However, there was no significant difference in the hs-CRP levels at hospitalisation between the two groups. No significant differences were observed when the clinical variables, medication, laboratory examination and CMR results were compared. Aldosterone antagonist use was significantly higher among patients with LGE-CMR and elevated hs-CRP (see online supplementary table 1).
During the follow-up period, the primary end point occurred in 20 patients: 5 (13.5%) patients without LGE-CMR and 15 (38.5%) patients with LGE-CMR. The difference between the two groups was significant (p value for log-rank=0.006; figure 3). Seven deaths (9%) were recorded, and the mortality rate was significantly lower for patients without LGE-CMR compared with patients with LGE-CMR (1 (2.7%) patient vs 6 (15.4%) patients, respectively, p value for log-rank=0.03). The cause of death was myelodysplastic syndrome for the patient without LGE-CMR, while mortalities in the LGE-CMR group were attributed to heart failure (n=4), infection during hospitalisation (n=1) and unknown aetiology (n=1). Patients with LGE-CMR were more frequently readmitted for heart failure compared with those without (9 (13.1%) patients vs 4 (11.8%) patients, p value for log-rank=0.07).

Survival curves according to the presence or absence of late gadolinium enhancement (LGE). Kaplan–Meier curve estimates for the time to all-cause mortality or rehospitalisation for the groups with or without LGE. The difference between the two groups was found to be significant using a log-rank test (p=0.006).
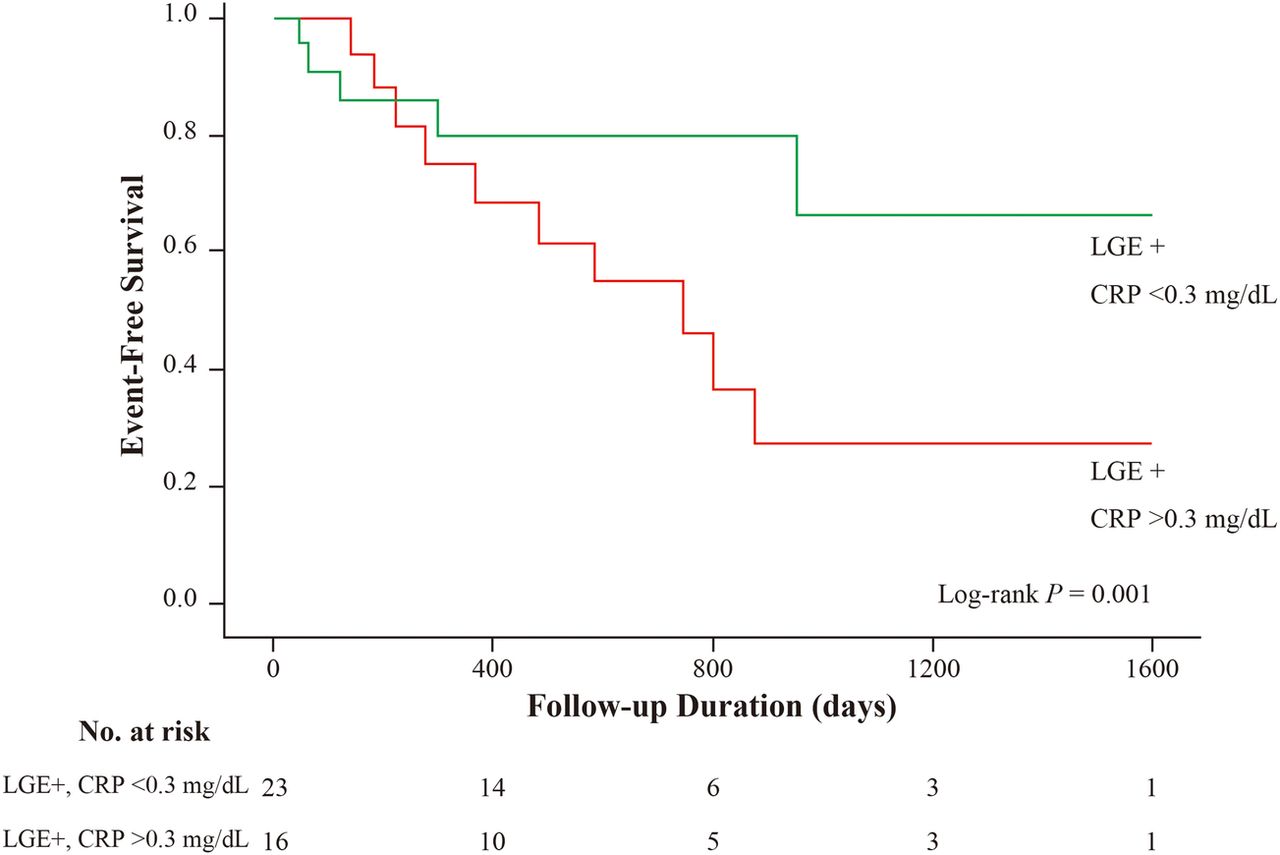
When patients with DCM with LGE-CMR were divided according to normal or elevated levels of hs-CRP, patients with elevated hs-CRP had a significantly higher incidence of adverse events compared with patients with normal hs-CRP (10 (62.5%) patients vs 5 (22.7%) patients, p value for log-rank=0.001; figure 4). The worst prognosis for patients with DCM was observed among those with LGE-CMR and elevated hs-CRP at stable state. The mortality rate was also significantly higher in patients with elevated hs-CRP compared with patients with normal hs-CRP (4 (31.2%) patients vs 1 (4.3%) patient, p value for log-rank=0.01). However, there was no significant difference in the rate of readmission for heart failure (4 (17.4%) patients without elevated hs-CRP, 5 (31.2%) patients with elevated hs-CRP, p value for log-rank=0.15).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Survival curves according to the presence of late gadolinium enhancement (LGE) and elevated high-sensitivity C reactive protein (hs-CRP). Kaplan–Meier curve estimates for the time to all-cause mortality or rehospitalisation according to the presence of LGE and elevated hs-CRP. The difference between the two groups was found to be significant using a log-rank test (p=0.001).
Unadjusted variables that were associated with the primary end point are listed in table 2. Prolonged elevation of hs-CRP at stable state was significantly associated with the incidence of the primary end point (HR: 4.04; 95% CI 1.67 to 9.76; p=0.002) and all causes of mortality (HR: 7.64; 95% CI 1.39 to 41.9; p=0.02). Further, when elevated hs-CRP was adjusted for known predictors of DCM, such as systolic blood pressure and plasma levels of BNP, it was still associated with all-cause mortality and hospitalisation for a cardiovascular event (HR: 2.91; 95% CI 1.19 to 7.15; p=0.02; table 2).
All-cause mortality and hospitalisation in univariate and multivariate analyses
Discussion
The major findings of this study were: (1) DCM with LGE-CMR had a significant relationship with mortality or rehospitalisation, and (2) in these patients, prolonged elevation of hs-CRP at stable state was the strongest predictor of adverse events during the long-term follow-up. The prognostic impact of LGE-CMR in patients with DCM has been previously reported,5–7 and our results indicate that LGE-CMR and elevated hs-CRP in patients with DCM following hospitalisation are associated with more number of severe outcomes.
LGE-CMR indicates the presence of myocardial fibrosis, which is an important prognostic indicator for DCM.5–8 Our results indicate that mortality or rehospitalisation was significantly higher in patients with LGE-CMR, which is in agreement with previous studies. McCrohon et al8 initially reported that 28% of patients with steady state DCM exhibited linear LGE-CMR limited to the mid-myocardium of the left ventricular wall. Subsequent studies have suggested that LGE-CMR is associated with all-cause mortality and cardiac transplantation, independent of traditional risk factors such as LVEF.6 ,7 ,9 ,10 An inherent limitation of LGE-CMR is that the extent of microscopic and diffuse fibrosis cannot be completely visualised. At times, it can also be difficult to distinguish between inflammation and fibrosis linked to LGE-CMR. The formation of cardiac fibrosis is a complex process that involves ischaemia, oxygen and pressure overload, and abnormal modulation of various hormones. These factors can result in activation of the renin-angiotensin-aldosterone system, and a strong relationship with inflammation has been established.11–15 Previous studies of patients with DCM have also suggested that patients with elevated CRP levels have a worse prognosis.16–18 Regarding the molecular mechanism of cardiac fibrosis, various factors can induce the transformation of fibroblasts to myofibroblasts.19 ,20 Through the proliferation of the extracellular matrix (ECM) and expression of ECM remodelling molecules, such as metalloproteinase (MMPs), myofibroblasts secrete multiple proinflammatory biomarkers, including interleukin (IL)-1β, IL-6, tumour-necrosis factor α (TNF-α) and CRP. These markers play an important role in subsequent myofibroblast activation and proliferation, and they are correlated with increased cardiac interstitial fibrosis.21–23 Persistence of myofibroblasts in scar tissue results in continued secretion of proinflammatory cytokines and MMPs, which can lead to excessive ECM degradation, ultimately resulting in wall thinning, dilation and progressive heart failure.24 ,25
Previously, small studies have demonstrated a correlation between hs-CRP levels and poor prognosis of DCM.16 ,17 ,26 ,27 Interestingly, in this study, hs-CRP levels at admission were not associated with adverse outcomes, although 41% of patients with LGE-CMR did exhibit elevated hs-CRP at stable state, and the combination of LGE-CMR and elevated hs-CRP at stable state was associated with poor prognosis. The results of our study confirm the value of assessing hs-CRP levels at stable state, and suggest that elevated hs-CRP should be considered an important predictor of risk in the long-term follow-up of patients with DCM with LGE-CMR. Therefore, LGE-CMR and hs-CRP might play complementary roles in the risk stratification of patients with DCM after acute decompensation. Interestingly, previous CMR studies in DCM have been limited to American Heart Association grading stage B, or to stage C in a clinically stable condition (New York Heart Association functional class II or less). The mortality rate of patients with stage C heart failure is known to be particularly high,28 and our results might have important clinical implications, as these high-risk patients would benefit greatly from precise risk stratification. Accurate stratification could be used to select advanced therapeutic modalities, such as assist device implant and/or heart transplantation, in a timely manner. However, it is unclear whether our findings can be applied to patients with Stage C heart failure who have had a recent episode of acute decompensation.
This study has several limitations. First, it was retrospective and conducted in a single tertiary university hospital. Therefore, a multicentre study with a large study population is required to validate the accuracy and prognostic significance of LGE-CMR and elevated hs-CRP levels. Second, there was no significant difference in the incidence of VF/sustained VT between the patients with and without LGE. Recently published data have shown that LGE-CMR is significantly predictive of VF/sustained VT in DCM.6 ,10 In our study, there was a trend towards a higher rate of VF/sustained VT in the patients with LGE, but the study seems underpowered for this comparison. However, patients with LGE-CMR and elevated hs-CRP had a significant higher incidence of VF/sustained VT. There was no significant difference in the device implantation rates between groups. In addition, in our study, the implantable cardioverter defibrillator/cardiac resynchronisation therapy implantation rate was higher than the rate of DCM in the general Japanese population.29 This is almost the same as the recent device implantation rate of DCM in western countries,6 indicating that the difference in survival rates cannot be completely explained by the device implanted. Third, despite adjusting for known risk factors, there was some residual confounding in the results of the Cox hazards models, which was caused by the use of both unmeasured and measured variables. Fourth, we did not assess fibrosis-related biomarkers, such as ST2 and galectin-3, or other inflammatory markers, such as TNF-α and MCP-1,30 ,31 as there are currently no suitable and sensitive commercially available assay systems. Moreover, these fibrosis-related biomarkers are not truly specific for fibroblasts, and might have limited use in our analysis. Fifth, our study population exhibited a higher incidence of LGE-CMR compared with previous studies. However, these studies analysed outpatients with chronic heart failure,5 ,6 ,8 which is in contrast to our population of high-risk patients who required admission due to AHF. Therefore, further confirmation is required to determine whether outpatient status decreases the incidence of adverse events associated with LGE-CMR. Sixth, the variable ‘LGE present, CRP >0.3 mg/dL’ was considered a dichotomous variable in the multivariate analysis. The two reasons were: (1) the number of patients in the study was too small to classify them into three groups as ordinal variables, and (2) the aim of the study was to investigate whether morphological and serological signs of inflammation together would predict long-term cardiovascular outcomes; as a surrogate marker of morphological signs of inflammation, we employed LGE-CMR and hs-CRP levels as serological signs of inflammation.
In conclusion, we were able to precisely stratify high-risk patients with DCM by long-term prognosis, using the presence of LGE-CMR complemented with serum hs-CRP levels. Patients with LGE-CMR and elevated hs-CRP had a higher incidence of the long-term combined primary end point of all-cause mortality and hospitalisation.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Contributors TS, SK, SO, TI, YS, TK, TY and KF conceived and designed the experiments. TS and SK were responsible for analysing the data and writing the manuscript.
Funding This work was supported by Grants-in-Aid for Scientific Research: 26461088 and 25460630.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Institutional Review Board of the Keio University School of Medicine.
Provenance and peer review Not commissioned; internally peer reviewed.
Data sharing statement No additional data are available.