Article Text

Statistics from Altmetric.com
The growing prevalence of valvular heart disease represents a major challenge in terms of short-term and long-term management and surveillance.1 ,2 Despite well-defined guidelines, appropriate detection and follow-up strategies are still poorly applied in valvular heart disease.3 ,4 In many countries, valvular heart diseases are managed by non-experts in the field, which may result in misdiagnosis and lead to inappropriate delays in decisions about valve interventions, and compromise patient outcome. The establishment of multidisciplinary services delivered by experts in valvular heart disease in a well-structured environment in order to provide specialised and centralised evaluation, care and education to patients with valvular heart disease has become the basis of implementation of ‘Heart Valve Centre of Excellence’ across Europe and outside Europe.5
Centres with a dedicated ‘Heart Valve Clinic’ have a designed pathway to diagnose and monitor patients with valvular heart disease. They regroup a multidisciplinary team of cardiologists, nurses, radiologists, anaesthesiologists, and surgeons proficient in diagnosing and treating all cardiac valve syndromes and disorders. This involves sophisticated cardiac valve symptoms recognition, diagnostic techniques such as three-dimensional echocardiography, cardiac magnetic resonance, cardiac CT and cardiac catheterisation.6 The ‘Heart Valve Clinic’ also provides help in optimising and monitoring medical treatment, assisting the general cardiologists for clinical decision-making, determining the correct timing and type of intervention, referring the patient to the most suitable surgeon, assessing results after intervention, and informing patients to motivate them to follow their prescribed medications and be alert for signs indicating a worsening of their disease.1 ,2
The ‘Heart Valve Clinic’ model is generally organised as a consultative cardiologist nurse-based clinic that forms the basis for the standard and advanced ‘Heart Valve Clinic’ structure. The vast majority of patients with valvular heart disease are suitable for investigation in the ‘Heart Valve Clinic’. However, prioritisation based on capacity, the degree of valvular heart disease severity, and the presence of an emergency condition might be applied. In the UK, senior nurses or sonographers are allowed to ensure surveillance and monitoring of patients with uncomplicated valve disease before and after surgery.2 Applying this model of care, the group of Chambers et al7 have shown that the proportion of patients followed up according to best practice guidelines rose (from 41% to 92%), while the total number of unwarranted echocardiograms performed fell significantly. Also, Rosenhek et al8 reported that the ‘wait’ for symptoms approach is a safe strategy when carried out in a ‘Heart Valve Clinic’. Surveillance in these clinics seems to also improve adherence to guidelines. However, despite this growing body of observational evidence supporting the notion that patient-centred care is best delivered within these organised structures, their adoption across Europe remains scanty, that is, 21% in the UK.5 Therefore, clarifying the patient outcome and the economic impact of such models of care represents a major goal for the ‘Heart Valve Community’. Outcome studies are ongoing. Several groups have merged their database, that is, the HeArt ValvE Clinic group, to enhance the clinical evidence of their usefulness.9
In practice, the decision to refer the patient for intervention is based on several factors: valvular heart disease severity, symptoms, degree of ventricular dysfunction, comorbidities, interventional risk, skill of the surgical/interventional team, patient preferences, and so on. These factors are often difficult to assess, require specific training, and a high expertise in valvular heart disease imaging, need to integrate newer risk stratification indices, require to be informed of recent changes in guidelines and cutting-edge therapeutic options in valvular heart disease.2 ,3 All this implies that professionals involved in the ‘Heart Valve Centres of Excellence’ (advanced valve clinics model) should have all the competencies to treat complex valvular heart disease or high-risk patients, and deep knowledge in the latest technologies and treatment methods (ie, valve repair, percutaneous valve intervention). These centres, thus, have all the facilities to treat and refer patients for valvular surgery/intervention. Often, they have a high-volume operation rate on valvular heart disease, which is believed to be associated with better repair results and potentially improved outcome.10 This partly explains why there is no obligation to refer patients eligible for surgical repair in centres of excellence.3 ,4
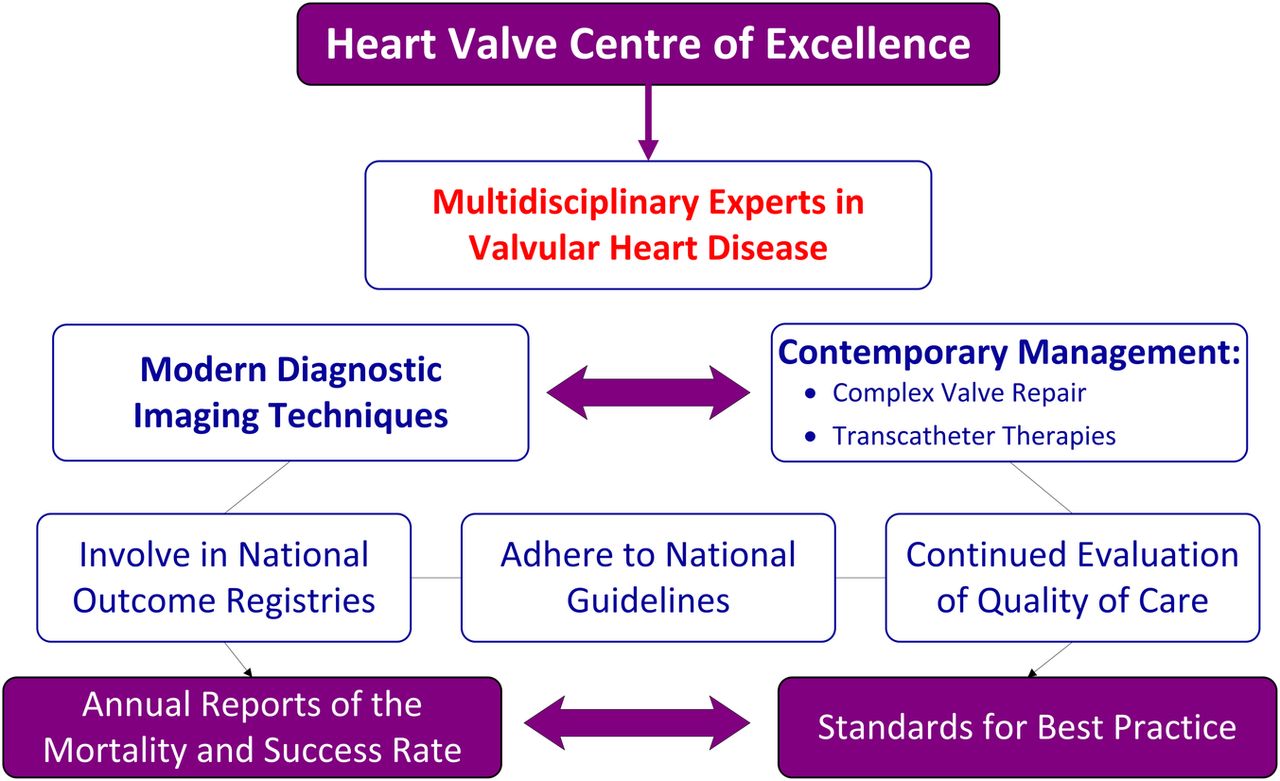
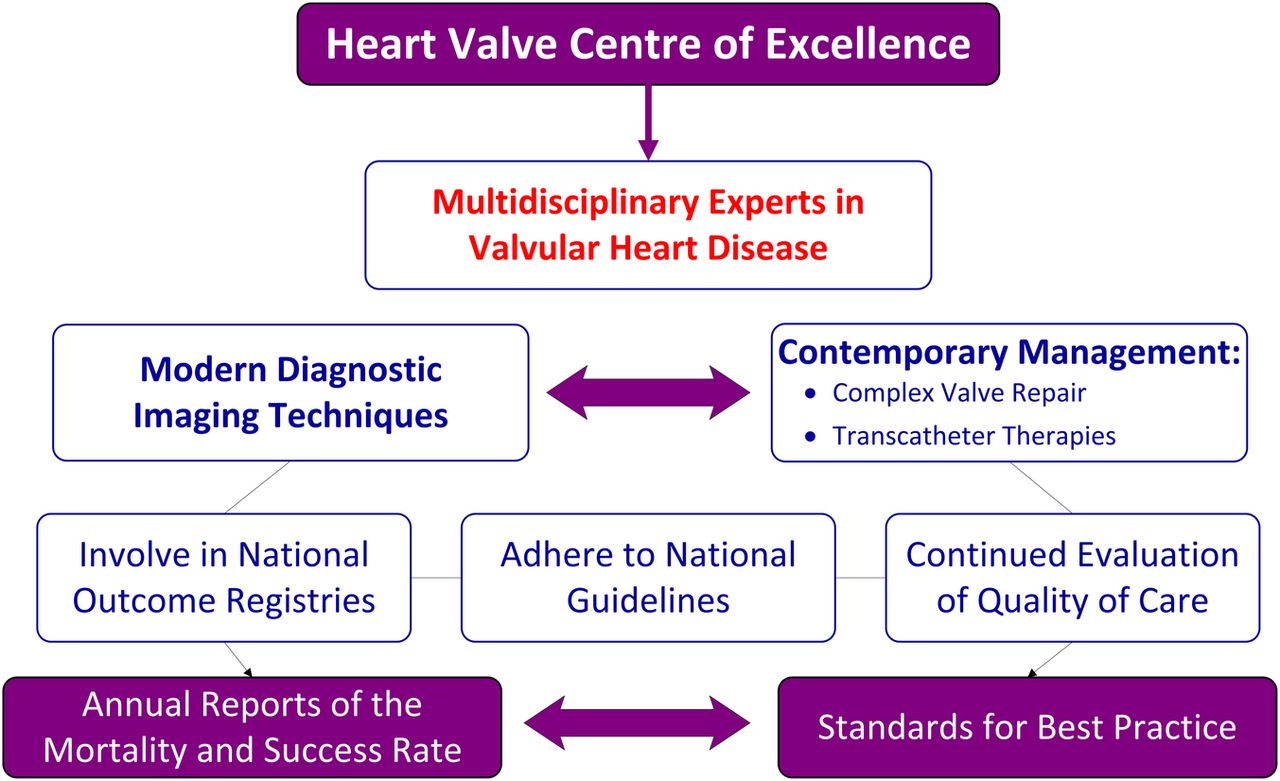
The present review paper of Chambers et al11 provides us with the appropriate standards for best practice in centres performing heart valve surgery. The strengths of the paper are that this subject is of particular relevance given this rapidly evolving field. It specifically addresses issues of multidisciplinary teams, including who the actors are, and their level of expertise/specialisation, levels of surgical experience and training, targets for surgical outcomes, acceptable hospital procedure volumes, and desirable national/international collaboration to monitor new therapeutic devices. The authors called for structured training programmes for the physicians and staff involved in the patient periprocedural care that should be performed under the umbrella of national societies. The coordination and monitoring of specialist training for all members of heart valve multidisciplinary teams should be considered as a national matter. The use of well-defined care pathways likely supports healthcare teams in implementing evidence-based key interventions and reduce clinical variations in everyday practice. As for other cardiovascular interventions, national cardiovascular professional societies should set up databases recording all valve implantations. Results of surgery should be readily available to patients, referrers and government agencies. This means that, ideally, universal entry onto national databases should be required. These data should include rates of residual regurgitation for mitral valve repairs and reoperation rates matched to the preoperative pathology and risk. Decisions about intervention at the ‘Heart Valve Centres of Excellence’ should thus be dependent on the centres’ publicly available mortality rates and operative outcomes4 (figure 1). Therefore, ‘Heart Valve Centres of Excellence’ may not necessarily have expertise in all valve problems. All this is consistent with the definition of best practices and the need for careful control of standards. In fact, the importance of quality control in healthcare is steadily increasing.12 Over the upcoming years, measurements of quality of care will likely become more and more a public product, used by patients, providers and official national institutions. This information should serve as an important guide for improvement, as well as a decision support tool for healthcare providers in charge of patients with valvular heart disease. The data capture should thus become integral to routine patient care. Common reporting systems could be used by national societies across Europe, which could serve to strengthen the missions of the ‘Heart Valve Centres of Excellence’ performing heart valve surgery. However, how to cross-fertilise the existing variety of national systems remains to be defined. The European Society of Cardiology Working Group on Valvular Heart Disease could become a major player in disseminating the concept of centres of excellence.
{kind=link}
Heart valve centre of excellence.
References
Footnotes
Contributors All the authors collaborated in writing, reading and amending this editorial and the figure.
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.