Article Text

Abstract
Background QRS duration and morphology are known established predictors of cardiac resynchronisation therapy (CRT) response, whereas mechanical dyssynchrony is not. Our aim was to determine if mechanical dyssynchrony provides independent prognostic information on CRT response.
Methods We studied 369 consecutive patients with heart failure (HF) with low ejection fraction (EF) and widened QRS receiving CRT. Radial dyssynchrony (septal-posterior radial peak strain delay ≥130 ms by speckle tracking) assessment was possible in 318 patients (86%). Associations with left ventricular end-systolic volume (LVESV) changes were examined using linear regression, and clinical outcomes analysed using Cox regression adjusted for multiple established outcome correlates.
Results Patients with radial dyssynchrony before CRT (64%) had greater improvements in EF (8.8±9.4 vs 6.1±9.7 units, p=0.04) and LVESV (−30±41 vs −10±30 mL, p<0.01). Radial dyssynchrony was independently associated with reduction in LVESV (regression coefficient −10.5 mL, 95% CI −20.5 to −0.5, p=0.040) as was left bundle-branch block (−17.7 mL, −27.6 to −7.7, p=0.001). Patients with radial dyssynchrony had a 46% lower incidence of death, transplant or implantation of a left ventricular assist device (adjusted HR 0.54, 95% CI 0.31 to 0.92, p=0.02) and a 39% lower incidence of death or HF hospitalisation (0.61, 0.40 to 0.93, p=0.02) over 2 years.
Conclusions Radial dyssynchrony was associated with significant improvements in LVESV and clinical outcomes following CRT and is independent of QRS duration or morphology, and additive to current ECG selection criteria to predict response to CRT.
- HEART FAILURE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key Messages
What is already known about this subject?
Implantation of cardiac resynchronisation therapy (CRT) in patients with heart failure is often based on ECG criteria, reflecting recent guidelines. Clinical trials have shown the greatest benefit of CRT is achieved in patients with QRS ≥150 ms and left bundle-branch block (LBBB; class I recommendation). However, the overall non-responder rate is at least 25% and higher in those of class IIa or IIb indication, with non-LBBB morphologies or QRS duration 120–149 ms. Although QRS morphology and width are important determinants of CRT response, it is less clear how to select patients for CRT with QRS between 120 and 149 ms and/or non-LBBB morphology and we hypothesised that the presence of mechanical dyssynchrony may provide additional prognostic information. Radial mechanical dyssynchrony has been associated with better outcomes post-CRT in patients with wide QRS HF in single and multicentre studies, but cannot be successfully used to select patients for CRT with narrow QRS as shown in a large prospective randomised multicentre trial. In addition, the magnitude of the effect of baseline mechanical dyssynchrony on reverse remodelling response and outcomes following CRT, and whether the effect is independent of QRS duration and morphology is still controversial.
What does this study add?
We hypothesised that the presence of radial mechanical dyssynchrony may provide additional prognostic information, independent and additive to what standard ECG criteria provides. Using predefined dyssynchrony definitions, echocardiographic outcomes and clinical outcomes, we studied 318 patients in whom a determination of radial dyssynchrony could be made prior to CRT. We show that the presence of radial dyssynchrony is independent of QRS duration and morphology in predicting outcomes, resulting in significant beneficial decrease in left ventricular volume and incidence of death or HF hospitalisations after adjusting for multiple baseline variables.
How might this impact on clinical practice?
The analysis and use of mechanical dyssynchrony information, in conjunction with ECG information in selecting patients for CRT, could reduce the non-responder rate.
Cardiac resynchronisation therapy (CRT) is an established treatment for patients with advanced heart failure (HF) with depressed ejection fraction (EF) and widened QRS complexes.1–3 Recent guidelines have focused on ECG criteria for patient selection because patients with a left bundle-branch block (LBBB) and QRS ≥150 ms have the greatest benefit from CRT (class I recommendation).4 In patients with advanced HF symptoms without LBBB and QRS ≥150 ms or LBBB and QRS duration 120–149 ms, CRT is still recommended but considered class IIa or IIb indication, where there is less clinical certainty.4 Although QRS morphology and width are important determinants of CRT response, it is less clear how to select patients for CRT with QRS between 120 and 149 ms and/or non-LBBB morphology, and we hypothesised that the presence of mechanical dyssynchrony may provide additional prognostic information. Radial mechanical dyssynchrony has been associated with better outcomes post-CRT in patients with wide QRS HF in single and multicentre studies,5–7 but cannot be successfully used to select patients for CRT with narrow QRS as shown in a large prospective randomised multicentre trial.8 In addition, the magnitude of the effect of baseline mechanical dyssynchrony on reverse remodelling response and outcomes following CRT, and whether the effect is independent of QRS duration and morphology is still controversial. Therefore, the objective of this study was to test the hypothesis that mechanical dyssynchrony measured by radial strain provides independent prognostic information about the left ventricular (LV) reverse remodelling response and clinical outcomes in patients with advanced HF treated with CRT. This study utilised predefined dyssynchrony criteria, and predefined short-term and long-term clinical outcome variables.
Methods
Patient population
We studied 369 consecutive patients with advanced HF from two institutions (United Heart & Vascular Clinic, St Paul, Minnesota, USA, and University of Pittsburgh, Pittsburgh, Pennsylvania, USA). Inclusion criteria were: ambulatory New York Heart Association (NYHA) functional class III-IV, QRS ≥120 ms, on optimal pharmacological therapy (ACE inhibitor or angiotensin receptor blocker (ARB) >1 month and β-blocker >3 months, if tolerated), EF ≤35%, technically adequate pre-CRT echocardiograms, and successful CRT implantation. Patients with ischaemic disease had coronary revascularisation procedures prior to CRT. The majority of CRT patients (93%) also received defibrillators. All patients had routine biventricular pacing using a standard right ventricular apical or septal lead, and an LV lead in an epicardial vein targeting posterolateral or lateral branches. Patients were followed in clinic after CRT implantation, as has been previously described.9 Institutional Review Board approval was obtained consistent with the protocols at both institutions.
Echocardiography, ECG and clinical outcomes
Echocardiographic studies (GE Vivid 7 system, Horten, Norway) were analysed (GE EchoPAC BT11, Horten, Norway) by investigators blinded to all other patient data. LV end-diastolic and end-systolic volumes (LVEDV and LVESV) and EF were measured by the biplane Simpson's rule. Dyssynchrony analysis using speckle-tracking echocardiography (STE) was performed as recommended by the American Society of Echocardiography/Heart Rhythm Society.10 Radial strain was obtained from mid-LV short-axis images with endocardial and epicardial regions of interest adjusted for optimal time-strain curves. Radial dyssynchrony was defined as a septal to posterior peak strain opposite wall delay of ≥130 ms.5 Our intraobserver variability is 6±6% and interobserver variability is 8±7%. Changes in EF and LV volumes were determined approximately 1 year after CRT. ECG width and morphology were obtained from automated computer analysis of ECGs and review of electrophysiologist notes prior to CRT implantation. The predefined clinical outcomes were death, transplant or left ventricular assist device (LVAD), and a composite of death or first HF hospitalisation following CRT. Clinical events were adjudicated independently by two investigators blinded to all echocardiographic data.
Statistical analysis
Continuous variables were summarised as mean±SD as all key variables were without substantially skewed distributions. Linear regression analysis was performed to relate radial dyssynchrony, LBBB and QRS ≥150 ms to changes in LVESV. Analysis of LVESV change was performed unadjusted (except for baseline LVESV to account for regression to the mean), minimally adjusted (adjusted for baseline LVESV and baseline QRS duration, and morphology), and fully adjusted with the addition of age, gender, HF aetiology, systolic blood pressure, diabetic status, serum creatinine, β-blocker usage, ACE inhibitor or ARB usage, aldosterone-antagonist usage and EF. Kaplan-Meier curves were reported to summarise time from CRT to clinical events. Clinical outcomes were adjusted by Cox regression that included the same variables listed above. Groups were compared using the HR and 95% CIs. The proportional hazards assumption was tested using Schoenfeld residuals. Tests for interactions were performed to determine whether the effect of radial dyssynchrony depended on either the presence of LBBB or QRS ≥150 ms. STATA/SE software V.12.1 (StataCorp, College Station, Texas, USA) was used with p<0.05 considered statistically significant.
Results
Baseline characteristics in the overall population of 369 patients with HF and in the patients with speckle tracking data available (separated by the presence or absence of radial dyssynchrony) are shown in table 1.
Baseline characteristics
There were 318 (86.2%) patients with echocardiographic images of adequate quality for measuring speckle tracking radial strain. Of these, 204 (64%) patients had radial dyssynchrony. Patients with radial dyssynchrony differed in baseline characteristics from those without radial dyssynchrony, with a lower percentage having an ischaemic aetiology of HF, and a higher percentage having LBBB. The QRS duration was wider, EF was lower and LV volumes larger in patients with radial dyssynchrony. Figure 1 shows a Venn diagram with circles representing the number of patients categorised by radial dyssynchrony, LBBB and QRS ≥150 ms. The areas enclosed within each geometric shape are proportional to the number of patients within each subgroup. Although there is considerable overlap of the three circles, this diagram demonstrates that radial dyssynchrony was present alone, with LBBB and with QRS ≥150 ms. Each grouping had a substantial number of patients, showing that radial dyssynchrony was not simply a marker of LBBB or wider QRS. Forty-three patients (14%) had radial dyssynchrony in the absence of LBBB and QRS ≥150 ms. In addition, 30% of patients had radial dyssynchrony with both LBBB and QRS >150 ms, whereas 13% of patients had no radial dyssynchrony, LBBB or QRS >150 ms.
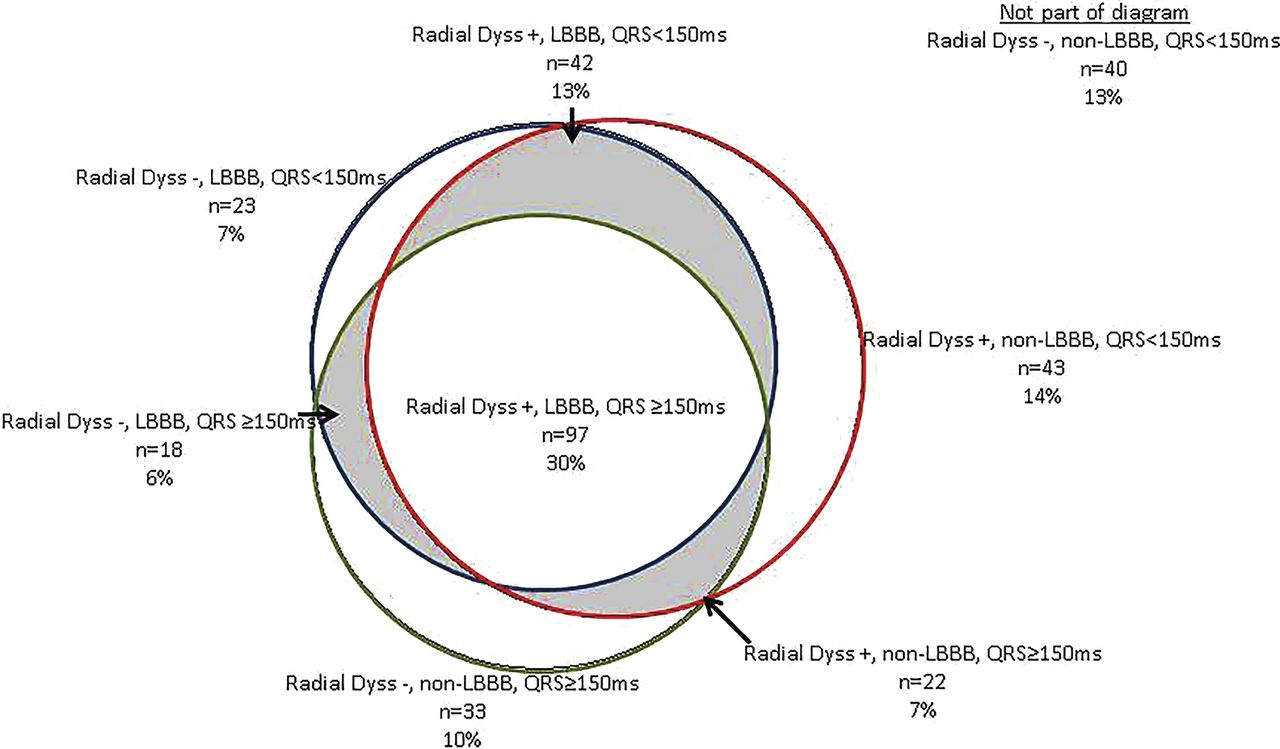
Venn diagram of patients with paired pre-cardiac resynchronisation therapy (CRT) and post-CRT echocardiograms. Red circle: patients with radial dyssynchrony (Dyss). Blue circle: patients with left bundle-branch block (LBBB). Green circle: patients with QRS ≥150 ms. The area within each geometric shape is proportional to the number of patients within each group. Shaded areas represent patients with two of the three variables present.
Relationship of radial dyssynchrony to reverse remodelling
There were 248 patients with paired pre-CRT and post-CRT echocardiograms where radial dyssynchrony could be assessed. On average, EF increased by 7.9±9.6% and LVESV decreased by 23±39 mL in the overall group. Patients with radial dyssynchrony had greater improvements in EF (8.8±9.4 vs 6.1±9.7 units, p=0.04), LVESV (−30±41 vs −10±31 mL, p<0.01) and LVEDV (−25±46 vs −4±36 mL, p<0.01) than those without dyssynchrony. Table 2 shows regression coefficients (changes in LVESV and LVESVi), and 95% CIs for the three main variables when unadjusted, minimally adjusted and fully adjusted by multivariable analysis.
Changes* in LVESV and LVESVi
Radial dyssynchrony and LBBB were significantly related to LVESV reduction in all analyses, whereas QRS >150 ms was related to LVESV reduction when unadjusted or minimally adjusted, but borderline (p=0.08) when fully adjusted. Similar results were obtained when LVESVi was used to assess reverse remodelling. The adjusted analyses indicate that radial dyssynchrony, LBBB and QRS duration (borderline) were independently related to improvement in LVESV.
Relationship of radial dyssynchrony to clinical outcomes
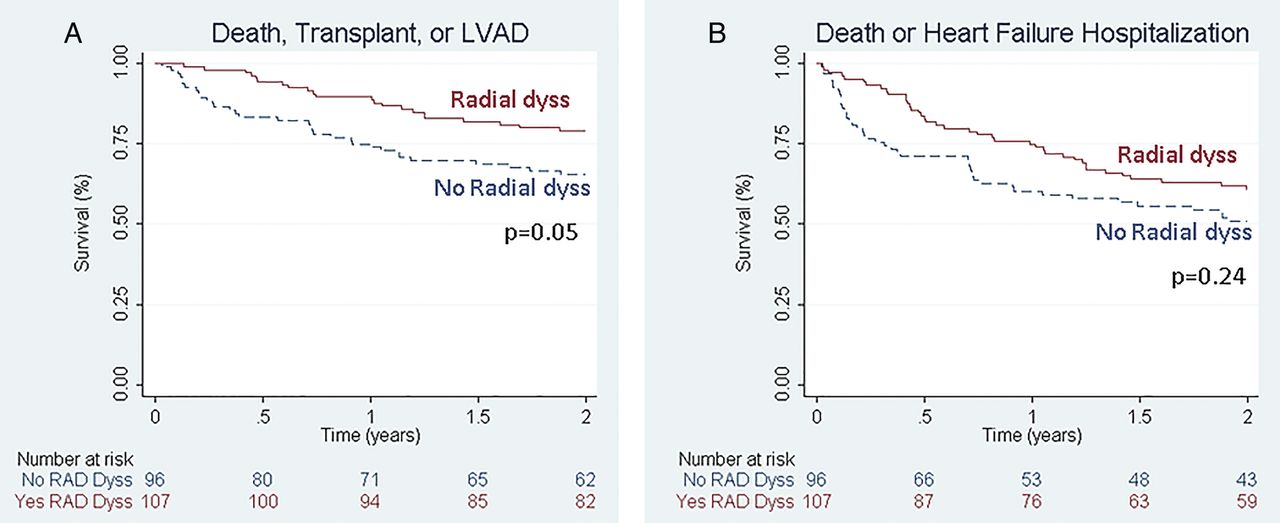
Baseline radial dyssynchrony (figure 2A) was associated with a 46% lower risk of death, transplant or LVAD (fully adjusted HR 0.54, 95% CI 0.31 to 0.92, p=0.02) and a 39% lower risk of death or HF hospitalisation (adjusted HR 0.61, 95% CI 0.40 to 0.93, p=0.02). In order to compare the effect of radial dyssynchrony on clinical outcomes with the effects of standard ECG baseline variables used in patient selection, Kaplan-Meier curves for patients dichotomised by LBBB and QRS width ≥150 ms were generated (figure 2B, C, respectively). The presence of LBBB was associated with a 58% lower risk of death, transplant or LVAD (adjusted HR 0.42, 95% CI 0.23 to 0.76, p<0.01) and a 55% lower risk of death or HF hospitalisation (adjusted HR 0.45, 95% CI 0.29 to 0.71, p<0.01). QRS width ≥150 ms was not significantly associated with lower risk of death, transplant or LVAD (adjusted HR 0.84, 95% CI 0.49 to 1.44, p=0.53) or lower risk of death or HF hospitalisation (adjusted HR 0.73, 95% CI 0.47 to 1.12, p=0.15).

Effects of radial dyssynchrony, LBBB and QRS duration on clinical outcome. Kaplan-Meier curves with adjusted clinical outcomes. Clinical outcomes were significantly better in patients with radial dyssynchrony (A) or LBBB (B) versus those without, but not in patients with QRS ≥150 ms (C). LBBB, left bundle-branch block; LVAD, left ventricular assist device.
Since use of CRT in patients with QRS width 120–149 ms and patients with QRS >150 but no LBBB is recommended at class IIa and class IIb levels, we compared clinical outcomes in the 203 patients in our study with either of these baseline characteristics dichotomised by the presence or absence of radial dyssynchrony. The presence of radial dyssynchrony in these patients (figure 3) was associated with a 48% lower risk of death, transplant or LVAD (adjusted HR 0.52, 95% CI 0.28 to 0.99, p=0.047). The presence of radial dyssynchrony in these patients was not significantly associated with a lower risk of death or HF hospitalisation (adjusted HR 0.74, CI 0.45 to 1.21, p=0.236).

{kind=link}
{kind=link}
{kind=link}
Effect of radial dyssynchrony in patients with QRS <150 ms or QRS ≥150 ms and non-LBBB. LBBB, left bundle-branch block; LVAD, left ventricular assist device.
Effects of radial dyssynchrony in patients with and without LBBB or QRS ≥150 ms
To determine whether the presence or absence of LBBB or QRS >150 ms significantly modified the effect of radial dyssynchrony on LVESV or clinical outcomes, we performed additional analyses. Table 3 shows the fully adjusted effects of radial dyssynchrony on changes in LVESV in patients with and without LBBB, and patients with and without QRS >150 ms.
Effects* of radial dyssynchrony by LBBB and QRS ≥150 ms
Although the effects of radial dyssynchrony tended to be greater when patients had LBBB or QRS >150 ms compared with when they did not, the tests for interaction were not significant in these small subgroups. In addition, tests for three-way interactions of radial dyssynchrony, LBBB and QRS >150 ms were not statistically significant. Combining the LBBB and QRS >150 ms subgroups (last 2 lines of table 3) the overall fully adjusted estimated effects of radial dyssynchrony are shown.
Discussion
Selection of patients with HF with low EF for CRT has recently been focused exclusively on ECG criteria of QRS width and morphology, and uncertainties remain for the candidacy of many potential CRT recipients with narrower QRS (120–149 ms) or non-LBBB morphology. This study demonstrated that patients with baseline dyssynchrony measured by echocardiographic radial strain have a greater LV reverse remodelling response after CRT. Although radial dyssynchrony was more common in patients with QRS >150 ms and/or LBBB, the effect of radial dyssynchrony on LVESV response was independent and additive to the effects of QRS >150 and/or LBBB, predicting a 10.5 mL greater decrease in LVESV with CRT. In addition, radial dyssynchrony was associated with a 46% lower incidence of death, transplant or LVAD, and a 39% lower incidence of death or HF hospitalisation after adjusting for multiple baseline variables and comorbidities. In patients with class II indications for CRT (QRS 120–149 ms or non-LBBB but QRS >150 ms) radial dyssynchrony was associated with a 48% adjusted reduction in death, transplant or LVAD suggesting that this measure could potentially assist in selection of patients for CRT who currently are borderline candidates.
Adding radial dyssynchrony to assessments of QRS width and morphology
Multiple studies have assessed the prognostic value of QRS width and morphology on response to CRT. Most studies have shown that both LBBB and wide QRS are important independent predictors of LV reverse remodelling and/or clinical response in patients with QRS >120 ms;11–13 some have emphasised the relative importance of LBBB14–16 or QRS >150.17 However, the predictive value of QRS width and morphology on CRT response remains controversial. For example, a meta-analysis of five randomised trials utilising patient-level data of nearly 3800 patients suggested that QRS width, but not morphology (LBBB), provided important information on clinical response.18 In contrast, data from an analysis of nearly 1500 patients in Resynchronization-Defibrillation for Ambulatory Heart Failure Trial (RAFT) emphasised the primary importance of QRS morphology (LBBB), although QRS duration provided further predictive value for CRT response.19 Our study expands on these previous investigations by adding echocardiographic assessment of radial dyssynchrony to established ECG variables and other standard correlates of outcome. It is important to emphasise that LBBB or wide QRS are not reliable indicators of the presence of radial dyssynchrony although, as shown in the Venn diagram, patients with LBBB and patients with QRS >150 ms were more likely to have radial dyssynchrony. More importantly, radial dyssynchrony was independently associated with improvements in LVESV and better patient outcomes. Though the tests for interactions between radial dyssynchrony and LBBB or QRS >150 ms duration were not statistically significant, the magnitude of the effect of radial dyssynchrony on CRT outcomes tended to be greater when patients also had LBBB or a QRS >150 ms. The overall fully adjusted effect of radial dyssynchrony on change in LVESV was ∼10 mL, which was less than the effect of LBBB (∼18 mL) but greater than the effect of QRS ≥150 ms (∼8 mL), which was of borderline significance.
With respect to clinical outcomes (adjusted for multiple baseline differences), the dichotomous variables radial dyssynchrony and LBBB were predictors, whereas QRS >150 ms was not. Though other studies have shown QRS duration to be an important predictor of clinical response to CRT, radial dyssynchrony was not typically measured or adjusted for in those studies, as it was in this study. It is possible that some of the predictive value of QRS duration is due to the presence of increased radial dyssynchrony as QRS lengthens. Similar to the effects of radial dyssynchrony on LVESV, the effects of radial dyssynchrony on clinical outcomes did not differ significantly when LBBB or QRS ≥150 ms were absent or present although the effect tended to be greater were they were present.
Previous studies of radial mechanical dyssynchrony
A number of different echocardiographic measures have been assessed in single or multicentre studies of responses to CRT. We chose to measure mechanical dyssynchrony using STE radial opposing wall delay for several reasons. First, this methodology has potential benefits over tissue Doppler imaging, including angle independence, measurement of active myocardial shortening and improved reproducibility.10 Second, retrospective20–22 and prospective6 studies in patients with wide QRS HF have demonstrated important benefit in predicting response to CRT. Three independent studies have associated the absence of dyssynchrony by radial strain with worse clinical outcomes of HF hospitalisation, death, heart transplant or LVAD.5 ,22 ,23 Although radial dyssynchrony (measured as we did in this study) was used in the ECHO-CRT study and did not show value in selecting narrow QRS patients who would benefit from CRT,8 the role of radial dyssynchrony in selection of wide QRS patients for CRT may be quite different. Finally, mechanical dyssynchrony information measured by radial strain STE has been shown to be useful at selecting LV lead position in a prospective randomised study.24
Clinical implications
The presence or absence of radial dyssynchrony, as measured by STE, is unlikely to significantly affect the decision to implant CRT in patients with a QRS ≥150 ms and a LBBB (as these patients have a high probability of response to CRT), although its presence predicts a greater remodelling and clinical effect. In patients with QRS 120–150 ms and in patients with QRS ≥150 ms but without a LBBB, radial dyssynchrony assessment may be of greater clinical utility. In our study, patients with one of these class II indications for CRT implantation comprised the majority (64%, 203 of 318) of patients with HF in whom radial dyssynchrony was able to be measured. This large group of patients on average have a smaller remodelling and clinical response to CRT than patients with a class I indication, and a test such as radial dyssynchrony measurement that provides independent prognostic information may help clinicians in deciding the risk/benefit ratio for implantation in a given patient.
Limitations
This was an observational longitudinal study, not a randomised controlled clinical trial. Accordingly, we did not have a control group of patients with advanced HF without CRT implantation for comparison. Additionally, we did not randomise patients to CRT based on dyssynchrony criteria. Thus, we could only relate radial dyssynchrony to the variation in outcome measures. Randomised controlled trials are needed to demonstrate the benefit of CRT when patients are selected based on assessment of radial dyssynchrony. Another important issue relates to our measurement of radial dyssynchrony. High-quality STE measurements cannot be made in all patients and have been criticised as being too variable.25 However, radial dyssynchrony has been shown to have acceptable agreement in 90% (κ coefficient 0.79) in a large multicentre clinical trial.8 To minimise bias, all echocardiograms were read by experienced personnel blinded to baseline characteristics, clinical outcomes, and irrespective of whether echocardiograms were performed pre-CRT or post-CRT. We did not assess myocardial scar or LV lead location, both of which have been shown to impact response to CRT.24 ,26 ,27 Finally, our data are based on radial dyssynchrony measurements and outcomes from two high-volume, experienced centres with echo core laboratories and may not be representative of CRT results at other institutions.
Conclusions
The presence of radial dyssynchrony, adjusted for multiple baseline variables, was associated with an approximately 10 mL decrease in LVESV, a 46% lower incidence of death, transplant or LVAD placement and a 39% lower incidence of death or HF hospitalisation in patients with advanced HF treated with CRT for standard indications. These effects were independent of LBBB and QRS ≥150 ms. We conclude that radial dyssynchrony may be useful, in addition to QRS duration and morphology, for identifying patients who are more likely to benefit from CRT.
References
Footnotes
Contributors AJB, JJM, TO, KVB, JG and RMG contributed substantially to the design, acquisition, analysis and interpretation of the data. AJB, JJM, TO, KVB, JG, DS, SS and RMG contributed substantially to the drafting and revising of the manuscript for important intellectual content. AJB, JJM, TO, KVB, JG, DS, SS and RMG provided final approval of the version published.
Funding Supported in part by a grant from Biotronik, Inc.
Competing interests AJB has received research grant support from Biotronik, Medtronic and Boston Scientific. JG has received research grant support from Biotronik, GE, Toshiba, Medtronic and St. Jude Medical. SS and DS have received research support from Medtronic and Boston Scientific.
Ethics approval Allina Health Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.