Article Text

Abstract
Objective Routine evaluation of performance measures for the system of care for patients with ST-elevation myocardial infarction (STEMI) is needed to improve the STEMI network. We sought to evaluate the current status of reperfusion therapy for STEMI in the capital city of a developing country where a STEMI network was introduced in 2010.
Methods Data were obtained from a local registry. A total of 28 812 patients admitted to the emergency department of a national cardiovascular hospital in three different periods (2007, 2010 and 2013) were retrospectively analysed; there were 2703 patients with STEMI.
Results In 2013 compared with 2007, there was a major increase in the number of primary percutaneous coronary interventions (PCIs) (35% vs 24%, p<0.001), and the proportion of non-reperfused patients fell (62.8% vs 67.7%, p<0.001). An improvement in the overall STEMI mortality rate was also observed (7.5% vs 11.7%, p<0.001).
Conclusions Implementation of a regional system of care for STEMI may improve utilisation of primary PCI. Future organisation of reperfusion therapy in a developing country such as Indonesia strongly calls for a strategy that focuses on prehospital care to minimise delay from the first medical contact to reperfusion therapy, and this may reduce the proportion of non-reperfused patients. These strategies are in concordance with guideline recommendations and may reduce or eliminate gaps in healthcare in developing countries, particularly the underutilisation of evidence-based therapies for patients with STEMI.
Trial registration number NCT 02319473, Clinicaltrials.gov.
- CORONARY ARTERY DISEASE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key Messages
What is already known about this subject?
An ST-elevation myocardial infarction (STEMI) network may overcome barriers to rapid reperfusion therapy in the community.
What does this study add?
This study adds knowledge about how to improve a STEMI system of care in a developing country.
How might this impact on clinical practice?
This study demonstrates that future organisation of reperfusion therapy in a developing country strongly calls for a strategy that focuses on prehospital care of STEMI patients to minimise delay from the first medical contact to reperfusion therapy.
Introduction
Despite advances in the pathophysiology and treatment of coronary artery disease, acute coronary syndromes (ACS) remain a major cause of morbidity and mortality in both industrialised and developing countries.1–3 Reperfusion therapy is the standard treatment for ST-segment elevation myocardial infarction (STEMI),4 ,5 but, in the real world, underutilisation of evidence-based therapies for patients with STEMI is common because real-world conditions do not allow us to perform rapid reperfusion therapy in all patients with STEMI.6–8 To overcome barriers to rapid reperfusion therapy in the community, a STEMI network has been introduced.4 ,5 However, despite the introduction of this network, barriers may still exist, limiting the utilisation of reperfusion therapy for STEMI patients.9
The existing barriers may differ between STEMI networks in industrialised countries such as Europe and the USA and developing countries such as Indonesia. Differences include the structure of the emergency medical services (EMS), utilisation of prehospital fibrinolysis, the number of cardiologists, the number of percutaneous coronary intervention (PCI) centres (receiving centres), and financial issues.
Furthermore, routine evaluation of performance measures for systems of care for STEMI is needed to improve STEMI networks. Therefore, we sought to evaluate the organisation of reperfusion therapy for STEMI in a developing country (Indonesia) where a STEMI network was introduced in the capital city (Jakarta) in 2010/2011,8 ,9 in order to analyse the current status of acute reperfusion therapy in that region.
Methods
Data source
Data were derived from the Jakarta Acute Coronary Syndrome (JAC) Registry database. The number of acute reperfusion therapies and the in-hospital mortality rate were taken from this database. In three one-year periods (2007, 2010 and 2013), a total of 28 812 patients admitted to the emergency department (ED) were retrospectively analysed; there were 2703 patients with STEMI. Patient distribution is shown in figure 1. STEMI was diagnosed on the basis of the presence of typical chest pain and ST-segment elevation (≥0.1 mV) in two or more contiguous leads on the initial ECG.
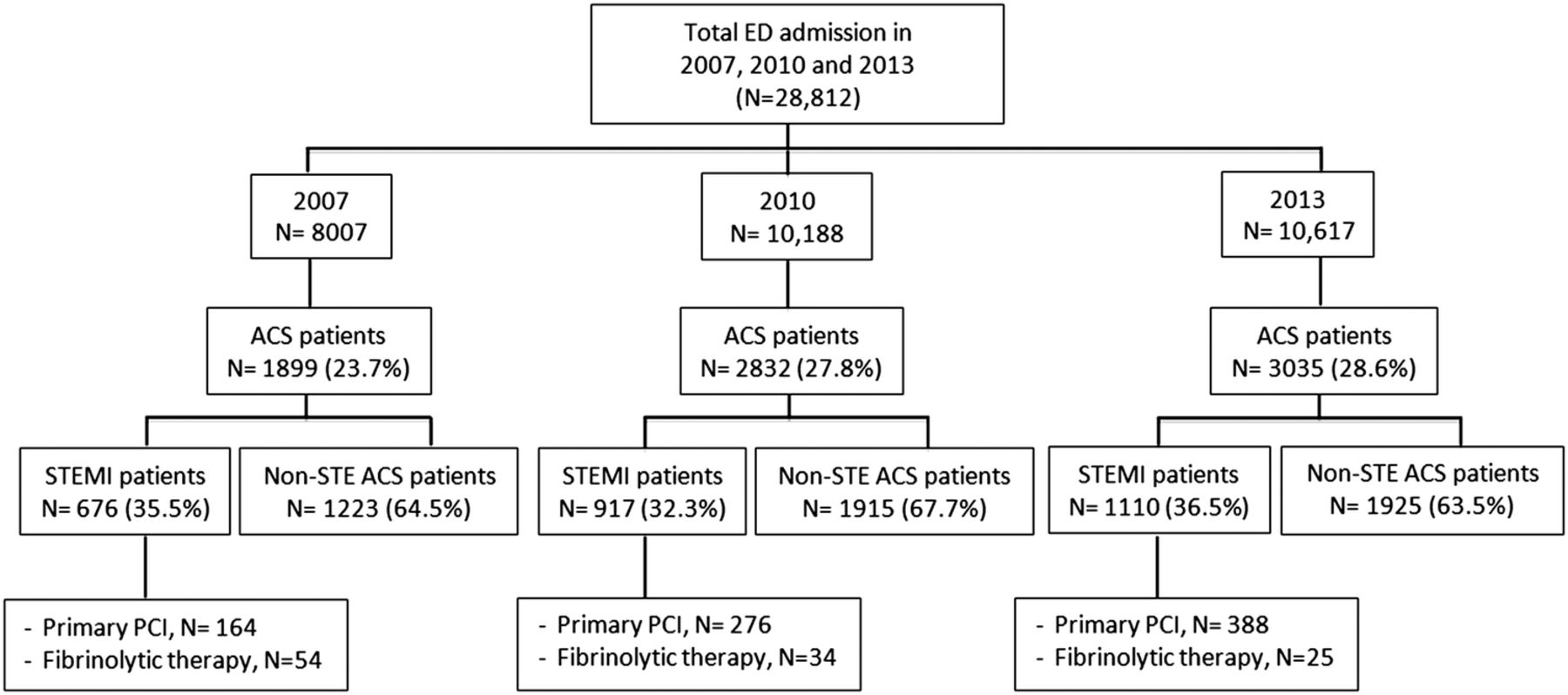
Patient distribution of the study population. ACS, acute coronary syndrome; ED, emergency department; Non-STE ACS, non-ST-elevation acute coronary syndrome; PCI, percutaneous coronary intervention; STEMI, ST-elevation myocardial infarction.
The ACS Registry and the Jakarta Cardiovascular Care Unit Network System
The JAC Registry is an ongoing prospective, single-centre, observational study that aims to enrol all patients with ACS admitted to the ED of the national cardiovascular referral hospital. The registry has been collecting data since 2007.
The JAC Registry is currently the main source of data for measuring the performance of the STEMI network in the region (Jakarta Cardiovascular Care Unit Network System). The STEMI network in Jakarta was introduced as an integral part of the government project in 2010/2011. It was built to improve the care of patients with STEMI in Jakarta. We found that, before introduction of the network, a large proportion of patients did not receive acute reperfusion therapy, and these patients had a significantly higher in-hospital mortality rate than those who received fibrinolytic therapy or primary PCI (13.3% vs 6.2% vs 5.3%, p<0.001).8 After introduction of the network, there were more interhospital referrals for STEMI patients (61% vs 56%, p<0.001), which led to more primary PCI procedures in our centre (83% vs 73%, p=0.005). However, the number of patients who presented very late (>12 h after symptom onset) was similar to that in the period before introduction of the network (53% vs 51%, p=NS).9
Study end points
Study end points are the proportion of patients with STEMI who received acute reperfusion therapy (primary PCI and fibrinolytic therapy) and the proportion of non-reperfused STEMI patients in three different periods (2007, 2010 and 2013). The overall in-hospital mortality rate was also assessed and compared between 2007 and 2013.
Statistical analysis
A descriptive analysis is provided based on the utilisation of reperfusion therapy in three different time periods (2007, 2010 and 2013). Categorical variables (proportion of patients receiving reperfusion therapy, proportion non-reperfused, and in-hospital mortality) are expressed as percentages or proportions, and differences between groups in two time periods (2007 and 2013) were compared by Pearson's χ2 test. The crude in-hospital mortality between STEMI patients treated with primary PCI and non-reperfused patients in the three periods (2007, 2010 and 2013) was also assessed and expressed as percentages. A p value <0.05 was considered to be significant. All computations were performed using the statistical package SPSS V.13.0.
Results
Study population
Of the total admissions to the ED, the proportion of ACS, as well as STEMI patients, had increased in 2013 compared with 2007 (28.6% vs 23.7% and 36.5% vs 35.5%, respectively) (figure 1). The number of ACS admissions to our hospital is high because it is the largest tertiary cardiac referral hospital in Jakarta and covers a population of about 11 million.
Acute reperfusion therapy
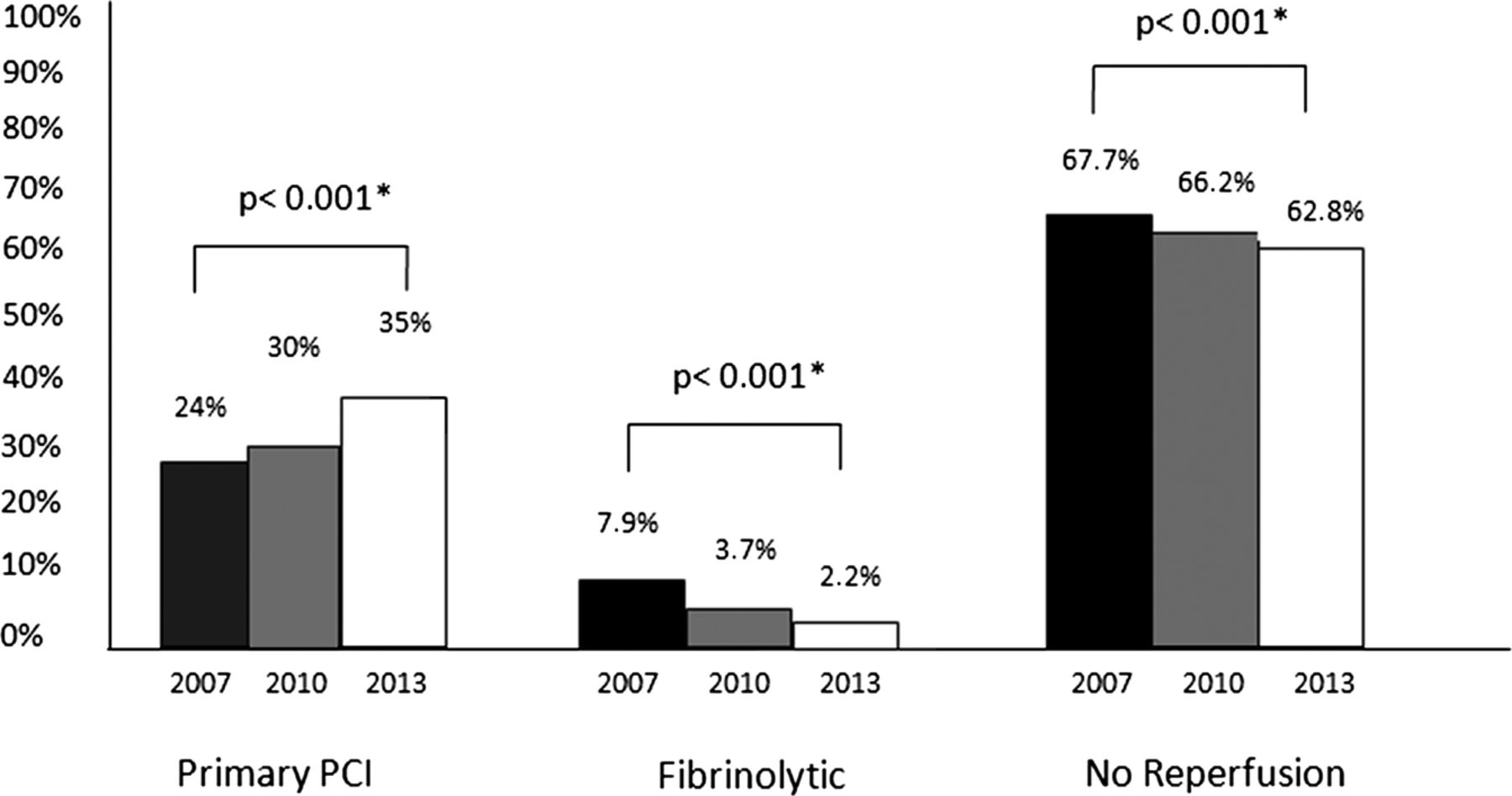
In 2013 compared with 2007, the number of STEMI patients receiving primary PCI had increased significantly (35% vs 24%, p<0.001), while the use of in-hospital fibrinolytic therapy had decreased (2.2% vs 7.9%, p<0.001). The proportion of patients who did not receive acute reperfusion therapy had fallen significantly in 2013 compared with 2007 (62.8% vs 67.7%, p<0.001). The distribution of acute reperfusion therapy is shown in figure 2.

Characteristics of reperfusion therapy for ST-elevation myocardial infarction (STEMI) patients in 2007, 2010 and 2013. PCI, percutaneous coronary intervention. *p Values given are based on differences between 2007 and 2013.
In-hospital mortality
Overall in-hospital mortality in STEMI patients had significantly decreased in 2013 compared with 2007 (84 (7.5%) vs 79 (11.7%), p<0.001). The non-reperfused STEMI patients had higher in-hospital mortality than STEMI patients treated with primary PCI (9.4% vs 2% in 2007; 4.8% vs 1.8% in 2010; and 4.9% vs 2.2% in 2013) (table 1).
Crude in-hospital mortality (%) of STEMI patients based on reperfusion status
Discussion
The presence of ST-elevation prompts the decision to proceed with rapid reperfusion therapy.4 ,5 However, in the real world, timely reperfusion therapy cannot be applied in all STEMI patients,6–8 particularly in a developing country where the STEMI network has been newly introduced in the capital city,8 ,9 with several barriers still in existence. Nevertheless, the use of primary PCI in our centre had increased significantly and the numbers of non-reperfused patients had fallen in the most recent year studied (figure 2).
Primary PCI
All primary PCI procedures reported in this article were performed in one hospital (the national cardiovascular centre), which is currently hosting the STEMI network in Jakarta, Indonesia. The hospital provides a 24/7 primary PCI service. There was a major increase in the number of primary PCIs performed in 2013 compared with 2007 (p<0.001). This result is in concordance with European data showing major increases in primary PCIs from 13 countries in recent years (2010/2011) compared with data from 2007.10 However, the primary PCI rate reported in the present study is lower than that in European networks such as in Belgium (86.4%)11 and Austria (92.4%).12 Although data for 2014 are not yet available, the use of primary PCI in our hospital is expected to reach 45% of STEMI patients admitted. This is similar to the rate obtained in small networks in Europe such as in Umbria, Italy (45.9%).13 The use of primary PCI is high in some European networks because many hospitals are involved and serve as receiving centres for primary PCI in each of the regional networks.11 ,12 ,14
Fibrinolytic therapy
None of the fibrinolytic therapy reported in this article was given in a prehospital setting. The main barrier to performing prehospital fibrinolytic therapy in Jakarta is the lack of highly trained physicians and nurses in this setting. In many European STEMI networks that are using a pharmaco-invasive approach, such as in Greece and Spain,10 paramedic ambulance personnel are trained to give lytic therapy en route to the nearest PCI centre. The benefit of prehospital fibrinolytic therapy as part of the pharmaco-invasive strategy for STEMI patients is demonstrated by the similar 1-year mortality rate of the pharmaco-invasive approach to that of primary PCI.15
STEMI patients without reperfusion therapy and prehospital protocol activation
Non-reperfused STEMI patients have a poor outcome.8 ,16 The proportion of non-reperfused STEMI patients in our centre had decreased significantly in 2013 compared with 2007 (p<0.001). However, the number of non-reperfused patients reported in this study is still high (62.8%). On the basis of our previous reports,8 ,9 the high proportion of non-reperfused patients is due to a high percentage of patients who present very late to the ED (>12 h after symptom onset). From our day-to-day experiences, we can identify several causes of system-related delay in the prehospital setting: delay in making the diagnosis; delay in administration processes at the primary hospital; late arrival of the ambulance; delay of ambulance departure; transportation delay due to traffic jams. It is known that a prolonged door-in door-out (DI-DO) time in the primary hospital may worsen the outcome of the patient.17 Therefore, the prehospital care of STEMI patients in Jakarta needs be improved.
A standardised prehospital triage form and a fibrinolysis checklist have previously been introduced9 and should be filled in by the EMS staff. The European STEMI networks in Germany,18 France19 and Vienna20 use a standard triage chart form extensively for all STEMI patients in the prehospital setting to increase awareness of EMS staff, to minimise time delays from the first medical contact to reperfusion therapy. From a patient-related-delay perspective, lack of awareness of signs and symptoms of a heart attack is the most common reason for late presentation of STEMI patients. Therefore, there is a need to increase public awareness that they should contact the regional emergency call centre on 119 if any symptom of myocardial infarction is suspected.
An established US national STEMI network has shown that door-to-device times met their previously defined national goals, but very few of the regions met current goals for first medical contact to device time.21 These findings suggest that focusing on prehospital care may be an important strategy for minimising reperfusion-related delay.
In-hospital mortality
The in-hospital mortality of STEMI patients in our centre has improved. The reported mortality is in concordance with recent results from observational studies in Europe.10 However, it should be noted that the reported mortality is the overall mortality in the population irrespective of reperfusion therapy choice.
Structure of the EMS
In the majority of STEMI networks in developing countries such as Indonesia, the EMS structure is made up of paramedics, and not all ambulances are staffed by doctors. A defibrillator or ECG monitor is not available in all ambulances. Ambulances cover other emergency conditions such as major trauma, stroke and evacuation processes and are coordinated by the local government.
Healthcare reform in Indonesia
In January 2014, the Ministry of Health of the Republic of Indonesia launched universal healthcare coverage in Indonesia where all costs related to acute reperfusion therapy (fibrinolytic and primary PCI) are covered by the government healthcare insurance system. This insurance programme may be the solution to the financial barrier to giving acute reperfusion therapy in the community.
Current situation and future perspectives of the STEMI network in Jakarta and Indonesia
The EMS is managed centrally at the Health Department of the Jakarta Metropolitan Government call centre (119) and works in close collaboration with the Heart Line team. The Heart Line is located in the ED of our hospital and is manned 24 h a day and 7 days a week. A pharmaco-invasive strategy is adopted in the network.8 The flow chart of the network is shown in figure 3.
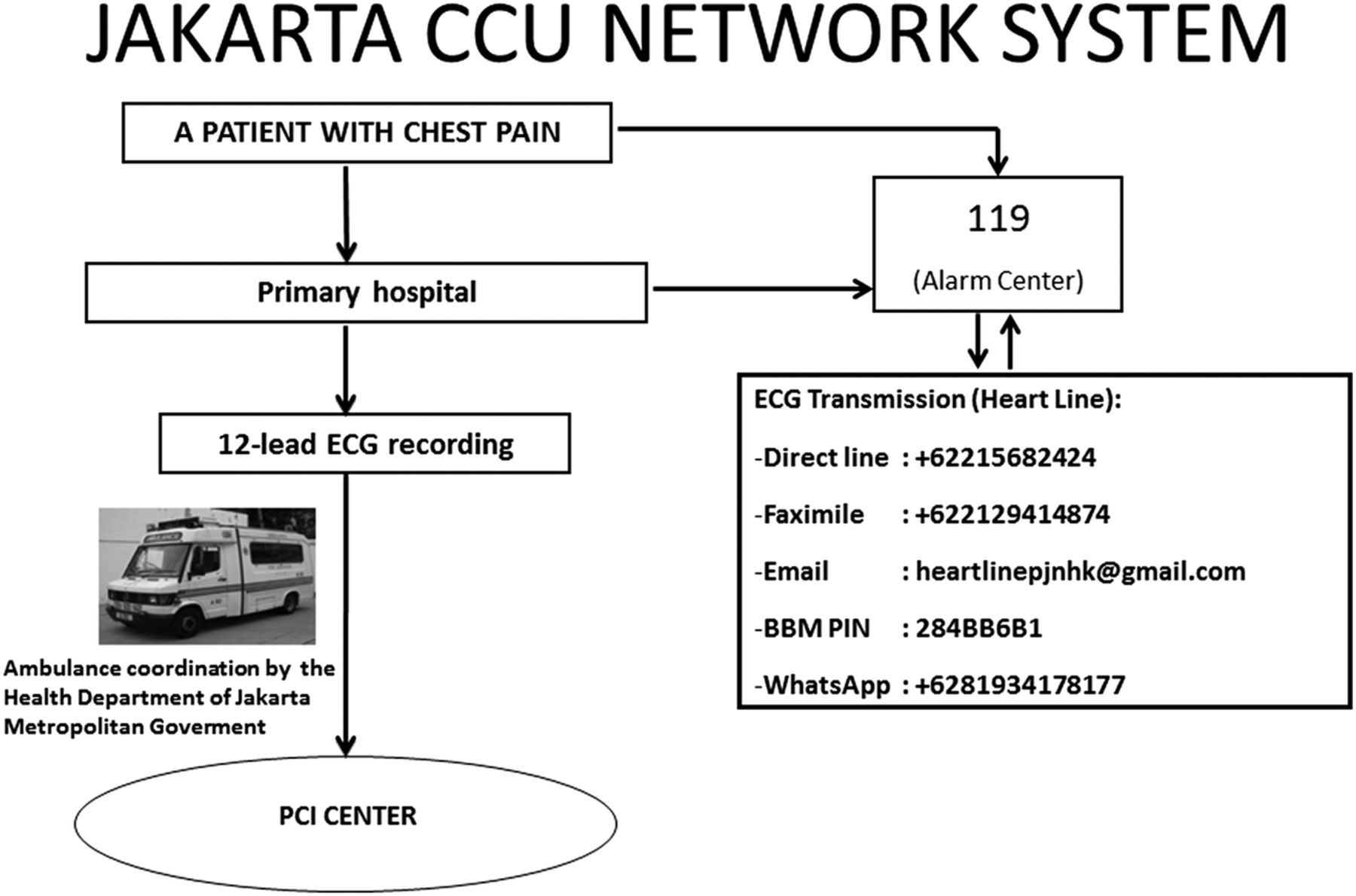
Flow chart of the Jakarta Cardiovascular Care Unit (CCU) Network System. There are four methods of ECG transmission to the Heart Line: faximile system, email, blackberry messenger and WhatsApp. After an ST-elevation myocardial infarction (STEMI) case has been identified by the cardiologist on duty at the Heart Line and the patient needs reperfusion therapy, the call centre staff will send an ambulance to transfer the patient to the nearest percutaneous coronary intervention (PCI) centre. BBM PIN, blackberry messenger personal identification number.
In some European STEMI networks such as in Germany18 and Denmark,22 network organisation is managed by the EMS staff. The EMS staff communicate directly with the PCI centre staff. The direct communication system reduces system delay by more than 1 h by bypassing local hospitals.23
To improve the care of STEMI patients in Jakarta, several coordinated plans have been proposed and discussed among other PCI centres, local government and the Ministry of Health of the Republic of Indonesia. The consensus is described below.
Jakarta has a population of around 11 million people with a density of 15 000 people/km2.8 Currently, the number of board-certified cardiologists in this city is 208. There are 128 non-PCI hospitals, 28 PCI hospitals (18%) and 44 public health centres (primary healthcare centre) (table 2). The mean number of cardiologist per million people in Jakarta is 18.9; this is lower than in Belgium (73), for example, which has a similar population to Jakarta.10
Demographic data on population and number of cardiologists and PCI centres
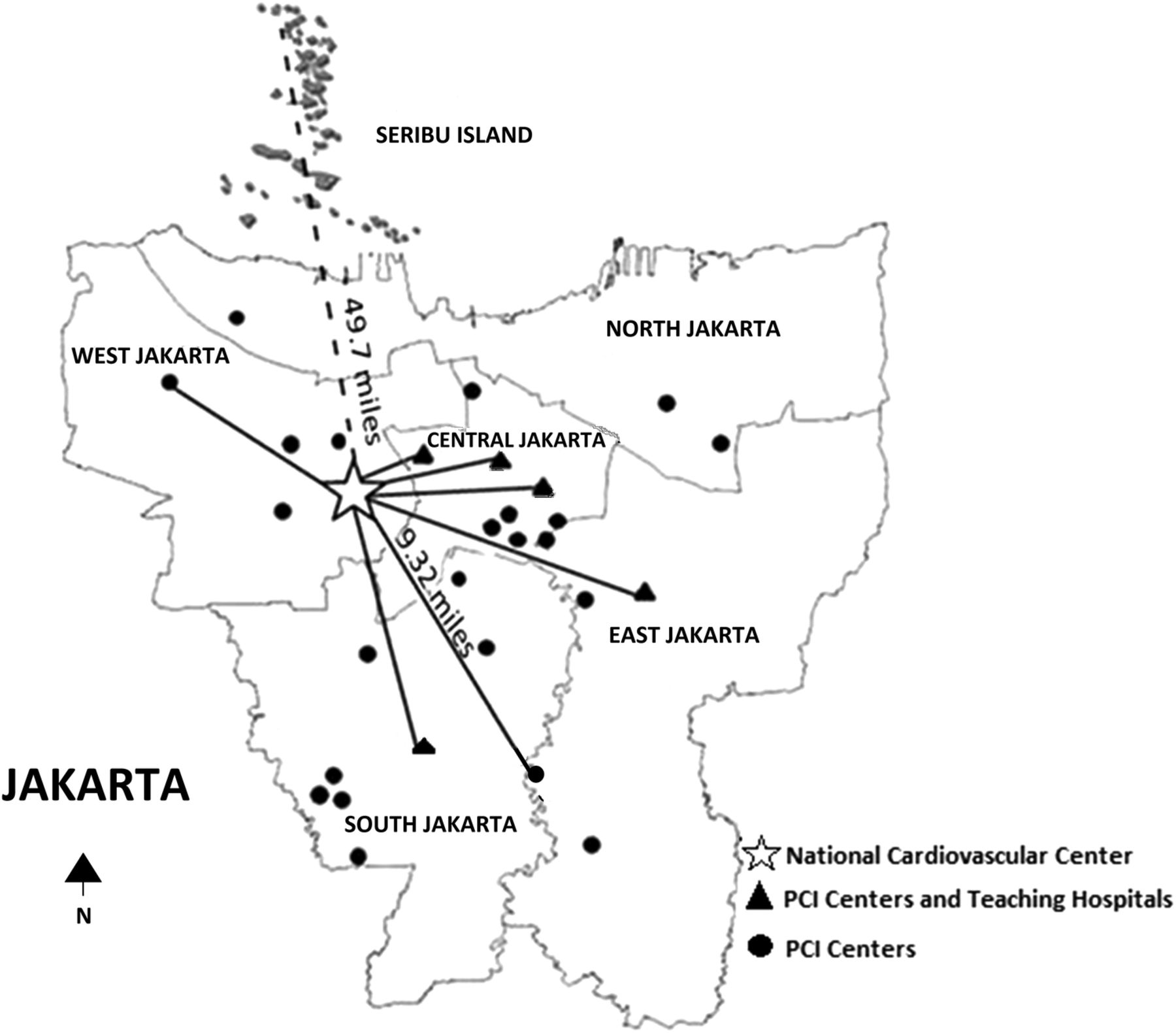
Although the number of primary PCIs carried out in our centre has increased, the overall primary PCI rate is still low. To increase access of primary PCI to the majority of STEMI patients within a reasonable time delay as recommended by the guidelines,4 ,5 other PCI centres in Jakarta need to be encouraged to become receiving centres for primary PCI. If a STEMI case is identified, the patient will be transferred to the nearest catheterisation laboratory. The longest distance from a PCI centre in Jakarta to our hospital is 9.32 miles, which can be covered in 3 h by road during office hours, while the longest distance from a primary healthcare facility to our hospital is 49.7 miles (4–6 h of transportation by water and road during office hours) (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Future ST-elevation myocardial infarction (STEMI) network programme in Jakarta.
Currently, only our hospital has a 24/7 service for primary PCI covered by the universal healthcare insurance system. In the future, other hospitals in Jakarta need to be encouraged to have a 24 h primary PCI service, especially the teaching hospitals, which might have higher primary PCI utilisation as reported by the Global Registry of Acute Coronary Events (GRACE).24 Figure 4 shows the future STEMI network programme in Jakarta involving eight PCI centres (government hospitals) which are currently covered by the universal government healthcare insurance system. Gradually, the government insurance system should be applied in other hospitals that provide a PCI service, and these hospitals may become receiving centres for primary PCI as part of the STEMI network programme.
A primary PCI service in other hospitals in Jakarta could be started during office hours (08:00–16:00) from Monday to Friday and gradually converted to a 24 h service. This programme may be possible if the healthcare insurance system is applied in all PCI centres and the number of cardiologists (both general and interventional) in Jakarta is increased to facilitate a 24/7 primary PCI service. Simulation training in interventional cardiology for young cardiologists should be accelerated. It is known that the number of physicians is associated with the level of primary PCI utilisation.25
The regional call centre (119) should be the coordinator of the STEMI network in Jakarta. ECGs should be transmitted directly to the nearest PCI centre (receiving centre), and decisions about reperfusion therapy should be made directly by the cardiologist at that PCI centre. When such a pathway works efficiently, reperfusion times are usually within the recommended guidelines and may improve the prognosis of the patient.
The standard prehospital triage form for STEMI and the fibrinolysis checklist9 should be used extensively by the EMS staff and filled in the prehospital setting. This should lead to earlier STEMI diagnosis and shorten the DI-DO time in the primary hospital, thus reducing the time from first medical contact to reperfusion therapy. These forms should be collected and recorded in a dedicated database to measure the performance of the STEMI system of care.
Prehospital fibrinolysis by trained EMS paramedics reduces delay and mortality compared with in-hospital fibrinolysis.26 ,27 EMS staff in Jakarta should be encouraged to give fibrinolytic therapy in the prehospital setting, and therefore the prehospital team should be trained effectively as an integral part of the network programme. Professional collaboration between the Indonesian Heart Association, the Indonesian Medical Association, the Indonesian National Nurses Association and the local healthcare authorities is needed to organise the training. Furthermore, ambulances should be equipped with a defibrillator and an ECG monitor along with a standard telemedicine system.
The JAC Registry has up until now been the only STEMI registry in Jakarta (performed in our hospital), but now it is being expanded to all primary hospitals including public health centres (referral centres) and other PCI centres (receiving centres) in the city. The data will be shared and should report the characteristics of STEMI patients efficiently in the region.
The new healthcare system should be applied in all PCI centres in Jakarta. This system should reduce competition among the hospitals. It seems that the financial issues have now been solved and should not be a problem in the future.
The efforts of creating a STEMI network in Jakarta should be copied by other regions in Indonesia. The protocol may differ among the regions because of differences in geographic, EMS structure and STEMI characteristics. Each region can start to build a network by constructing a registry of STEMI patients admitted to the regional cardiovascular centre. The data will give an initial insight into the strategy of reperfusion therapy that should be applied to the region. The registry is also important to obtain a national dataset on STEMI, which is not currently available. Another priority is to increase the number of cardiologists in Indonesia.
Timely reperfusion improves survival of STEMI patients.4 ,5 Barriers to, and delay in, reperfusion therapy in Jakarta are primarily related to fragmentation of the health system and lack of coordination between EMS staff and hospitals. Therefore, shifting the focus from door to device (hospital care) to first medical contact to reperfusion time (prehospital care) identifies great opportunities to improve timely reperfusion therapy in Jakarta.
This report may reflect barriers to STEMI networks in other developing countries. Therefore, routine evaluation of STEMI network performance may improve care of STEMI patients in every region.
Strengths and limitations of the study
The major strength of the study is that we were able to include an analysis of all STEMI patients (100%) admitted to the hospital, reflecting the true STEMI characteristic of the centre. We also provide updated information on the number of hospitals with PCI facilities, as well as the number of cardiologists in Jakarta.
The major limitation of the study is that all STEMI patients analysed were from a single centre. To reflect the true STEMI characteristics of the city, other hospitals should be encouraged to create registries of STEMI patients, and the data should be shared. Furthermore, the reasons for delayed presentation of STEMI patients reported were based on expert opinion.
Conclusion
Implementation of a regional system of care for STEMI may increase utilisation of primary PCI. In the future, organisation of reperfusion therapy in a developing country such as Indonesia strongly calls for a strategy that focuses on prehospital care to minimise the delay from first medical contact to reperfusion therapy, and this may further reduce the proportion of non-reperfused STEMI patients. The strategies are in concordance with guideline recommendations and may reduce or eliminate gaps in healthcare, particularly the underutilisation of evidence-based therapies for patients with STEMI.
Acknowledgments
The authors thank the Indonesian Heart Association (Jakarta Branch) and the staff of the Health Department of Jakarta Metropolitan Government for providing the data on the number of cardiologists and hospitals.
References
Footnotes
Competing interests None declared.
Ethics approval Institutional Review Board of National Cardiovascular Center Harapan Kita, Jakarta, Indonesia.
Provenance and peer review Not commissioned; externally peer reviewed.