Article Text

Abstract
Purpose Left atrial (LA) volume is a strong prognostic predictor in patients following ST-segment elevation myocardial infarction (STEMI). However, the change in LA volume over time (LA remodelling) following STEMI has been scarcely studied. We sought to identify predictors for LA remodelling and to evaluate the prognostic importance of LA remodelling.
Methods This is a subgroup analysis from a randomised clinical trial that evaluated the cardioprotective effect of exenatide treatment. A total of 160 patients with STEMI underwent a cardiovascular MR (CMR) 2 days after primary angioplasty and a second scan 3 months later. LA remodelling was defined as changes in LA volume or function from baseline to 3 months follow-up. Major adverse cardiac events were registered after a median of 5.2 years.
Results Adverse LA minimum volume (LAmin) remodelling was correlated to the presence of hypertension, larger infarct size by CMR, higher peak troponin T, larger area at risk and adverse left ventricular (LV) remodelling. LA maximum volume (LAmax) remodelling was correlated to larger infarct size by CMR, higher peak troponin T, larger area at risk, larger LV mass, impaired LV function and adverse LV remodelling. Kaplan-Meier and Log Rank analyses showed that patients in the highest tertiles of LAmin or LAmax remodelling are at higher risk (0.030 and p=0.018).
Conclusions After a myocardial infarction, LA remodelling reflects a parallel ventricular-atrial remodelling. Infarct size is a major determinant of LA remodelling following STEMI and adverse LA remodelling is associated with an unfavourable prognosis.
- HEART FAILURE
- STEMI < MYOCARDIAL ISCHAEMIA AND INFARCTION (IHD)
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Left atrium maximum volume is a well-known predictor in various diseases. Left atrium dilation over time after an acute myocardial infarction is affected by the same mechanisms as left ventricle diastolic function, such as hypertension, renal impairment, diabetes, ischaemia and left ventricle mass. Previous studies have also identified that adverse left atrium maximum volume remodelling following an acute myocardial infarction is related to impaired outcomes. Left atrium remodelling has mainly been studied using two-dimensional or M-mode echocardiography.
What does this study add?
We provide cardiovascular MR (CMR) imaging measures of left atrial volume and function remodelling after an acute myocardial infarction. We evaluate predictors of left atrial volume and function remodelling. In the present paper, we demonstrate that a larger final infarct size measured by CMR and troponin T results in adverse left atrium volume remodelling. In addition, we find that both adverse left atrium minimum volume and left atrium maximum volume remodelling is associated with an unfavourable prognosis.
How might this impact on clinical practice?
We have shown that left atrial volume is affected by infarct severity after an acute myocardial infarction, and the larger the left atrium, the worse the outcome. Owing to costs of MRI, it is unlikely that MRI scanning of patients with STEMI will be implemented as part of routine risk stratification of patients. This study adds to our understanding of cardiac pathophysiology and remodelling after an acute myocardial infarction and adds parameters that affect left atrium volume and function.
Introduction
Left atrial (LA) volume is a prognostic predictor across a wide spectrum of cardiac and non-cardiac diseases.1–10 During diastole, the mitral valve opens and the pressure in the LA and left ventricular (LV) cavities is equalised. Increased LA pressure will cause LA dilation over time (also known as LA remodelling).11–14 LA remodelling is basically influenced by the same mechanisms as LV diastolic function.15 LV relaxation and filling pressure after an acute myocardial infarction may be related to the formation of scar tissue. Therefore, following an acute myocardial infarction, the LA dilates over time.11–14 Thus, we hypothesise that a larger infarct size may lead to reduced LV compliance and consequently increased LV and LA pressures and thereby result in LA enlargement over time.
In terms of LA remodelling, previous studies have focused on LA maximum volume (LAmax). We have recently demonstrated that LA minimum volume (LAmin) and LA fractional change (LAfc) measured immediately after an ST-segment elevation myocardial infarction (STEMI) are better correlated to LV function and infarct size than LAmax and may also be stronger prognostic predictors.16 This has been confirmed in a non-STEMI population.8 However, the remodelling of LAmin volume and LA function following STEMI has not been studied previously. Also, LAmax remodelling has mainly been studied using two-dimensional or M-mode echocardiography.7 ,17 ,18 Owing to the excellent spatial resolution, accuracy and reproducibility of cardiovascular MR (CMR), it is an ideal method for studying remodelling of LA volumes and LA function over time.19–21 CMR also allows for accurate assessment of LV infarct size, area at risk and myocardial salvage.22–26
Thus, using CMR, we sought to evaluate (1) the predictors for LA volume (LAmin and LAmax) remodelling and LA function (LAfc) remodelling after STEMI, to improve our knowledge of the dynamics of postinfarction cardiac remodelling, (2) the impact of infarct size on LA remodelling; and (3) the prognostic importance of adaptations in LAmin, LAmax and LAfc.
Materials and methods
Study population
The present study included 160 patients with a first STEMI and symptom duration≤12 h included in a previously published randomised study evaluating the cardioprotective effect of exenatide treatment.27 ,28 STEMI was defined as ST-segment elevation in two contiguous ECG leads of 0.1 mV in V4—V6 or limb leads II, III and augmented vector foot (aVF), or 0.2 mV in leads V1–V3. Patients were not considered for enrolment if they presented with cardiogenic shock or were unconscious. Patients with acute stent thrombosis, known renal insufficiency, atrial fibrillation or previous coronary artery bypass graft surgery were also excluded. All patients eligible for primary percutaneous coronary intervention (PCI) were pretreated with aspirin (300 mg orally or 500 mg intravenously), clopidogrel (600 mg orally) and unfractionated heparin (10.000 U intravenously) administered before the PCI.
On arrival at the catheterisation laboratory, a coronary angiography was performed to identify the culprit lesion, and primary PCI was performed according to international guidelines. Glycoprotein IIb/IIIa receptor antagonists were administered if no contraindications were present. All patients were treated with clopidogrel 75 mg daily for 12 months and aspirin 75 mg daily indefinitely. Cardiac biomarkers (troponin T) were obtained before intervention, immediately after and at 6 and 12–18 h. All patients were informed verbally and in writing and all gave their written consent before inclusion. The study was performed according to the Helsinki declaration of good clinical practice and The Danish National Committee on Biomedical Research Ethics approved the protocol. Only patients with two full CMR scans (one at baseline CMR 2 days after STEMI and another after 3 months) were included in the present analysis. No patients had moderate or severe mitral regurgitation evaluated using echocardiography.
CMR acquisition and analysis
CMR was performed twice; the first scan was performed within a median of 2 days after STEMI (IQR 1–3 days) and the follow-up scan within a median of 89 (IQR 80–93) days after index STEMI on a 1.5 T scanner (Avanto scanner, Siemens, Erlangen, Germany). LV and LA volumes were assessed using a steady-state free precession cine sequence (slice thickness 8 mm, slice gap 0 mm, echo time 1.5 ms, field of view 300–360 mm, phases 25). Multiple slices in the short-axis image plane were obtained covering the entire cardiac fossa. The area at risk was assessed on the first scan as oedema using a T2-weighted short tau inversion recovery sequence (slice thickness 15 mm, field of view 300–360 mm, inversion time 180 ms, repetition time 2 R–R intervals, time to echo 65 ms, slice gap 0 mm). Final infarct size was assessed on the follow-up CMR scan using a delayed enhancement inversion-recovery sequence (slice thickness 8 mm, slice gap 0 mm, echo time 1.4 ms, field of view 300–360 mm, slice gap 0 mm). Images were obtained 10 min after administration of diethylenetriamine pentaacetic acid (0.1 mL/kg; Gadovist, Bayer Schering, Berlin, Germany).
All LV and LA volumes were calculated by manually tracing the endocardial border in all 25 time frames in each short axis slide. The papillary muscles were considered as part of the LV cavity.27 ,28 The LA appendage was considered as part of the LA volume. LAmax and LAmin were defined as the largest and smallest volumes. LAfc was calculated as follows: ((LAmax—LAmin)/LAmax).8 ,16 The analysis was performed with ARGUS, Siemens. All LV and LA volumes were standardised according to the body surface area. LV and LA remodelling was defined as an absolute volume change from the baseline scan to the follow-up CMR scan (LA follow-up—LA baseline). A decrease in LA volume was defined as reverse LA remodelling (negative values in the results section) and an increase as adverse LA remodelling (positive values in the results section). A single operator performed all CMR analyses, and all CMR analysis was performed blinded to clinical data as well as to results from the other CMR scan. Interobserver variability was assessed in 50 randomly selected patients with a mean percentage error of 3±10% for LAmin, 4±8% for LAmax and 1±11% for LAfc.16 ,21
The final infarct size was measured using Segment v1.8.25 Endocardial and epicardial borders were manually traced in short-axis images and the LV mass was calculated. The infarct size (defined as the hyper-enhanced myocardium on the delayed enhancement images) was measured using a semi-automated technique, which has been described previously.26 On the T2-weighted short-axis images, the area at risk was defined as the hyper-intensive myocardium with a signal intensity >2 SDs of the signal intensity in the normal myocardium.24 The salvage index (%) was calculated as follows: (area at risk—infarct size)/area at risk.23
Clinical end point
Major adverse cardiac events (MACE) were defined as all-cause mortality, reinfarction, admission for congestive heart failure (peripheral or pulmonary congestion) and implantation of an implantable cardioverter defibrillator. In Denmark, each person has a unique social security number that can be used to register hospital admittance and whether the person is alive. A reviewer blinded to all clinical data used this social security number to evaluate readmissions during the follow-up. Follow-up was defined at the time of the baseline scan.
Statistics
All continuous variables are expressed by their mean (SD) or median (IQR). Binomial variables are expressed as numbers (%). Study population characteristics are compared according to included and excluded patients (table 1) using χ2 and t tests. Continuous CMR variables were included in a linear regression to LAmin and LAmax remodelling (table 2). CMR determined baseline LAmax was compared with echocardiographic determined baseline LAmax using an xy-plot and a linear regression analysis (figure 3). Normal distribution was tested visually on a histogram. Graphing Kaplan-Meier survival function estimates were used to assess proportional hazards for categorical covariates.
Study population
Univariate linear regression
We assessed the discriminative power of LAmax, LAmin and LAfc remodelling to predict 5 year event rates of MACE by calculating the area under the curve of the receiver-operating-characteristic (ROC) curve. Further, we assessed the optimal cut-off point as a point on the ROC curve closest to the coordinate (0, 1), which can be calculated as  .29 All statistical analysis was performed using ‘R’ (V.3.0.3; R Development Core Team 2014, http://www.R-project.org/). A two-sided p value <0.05 was considered statistically significant.
.29 All statistical analysis was performed using ‘R’ (V.3.0.3; R Development Core Team 2014, http://www.R-project.org/). A two-sided p value <0.05 was considered statistically significant.
Results
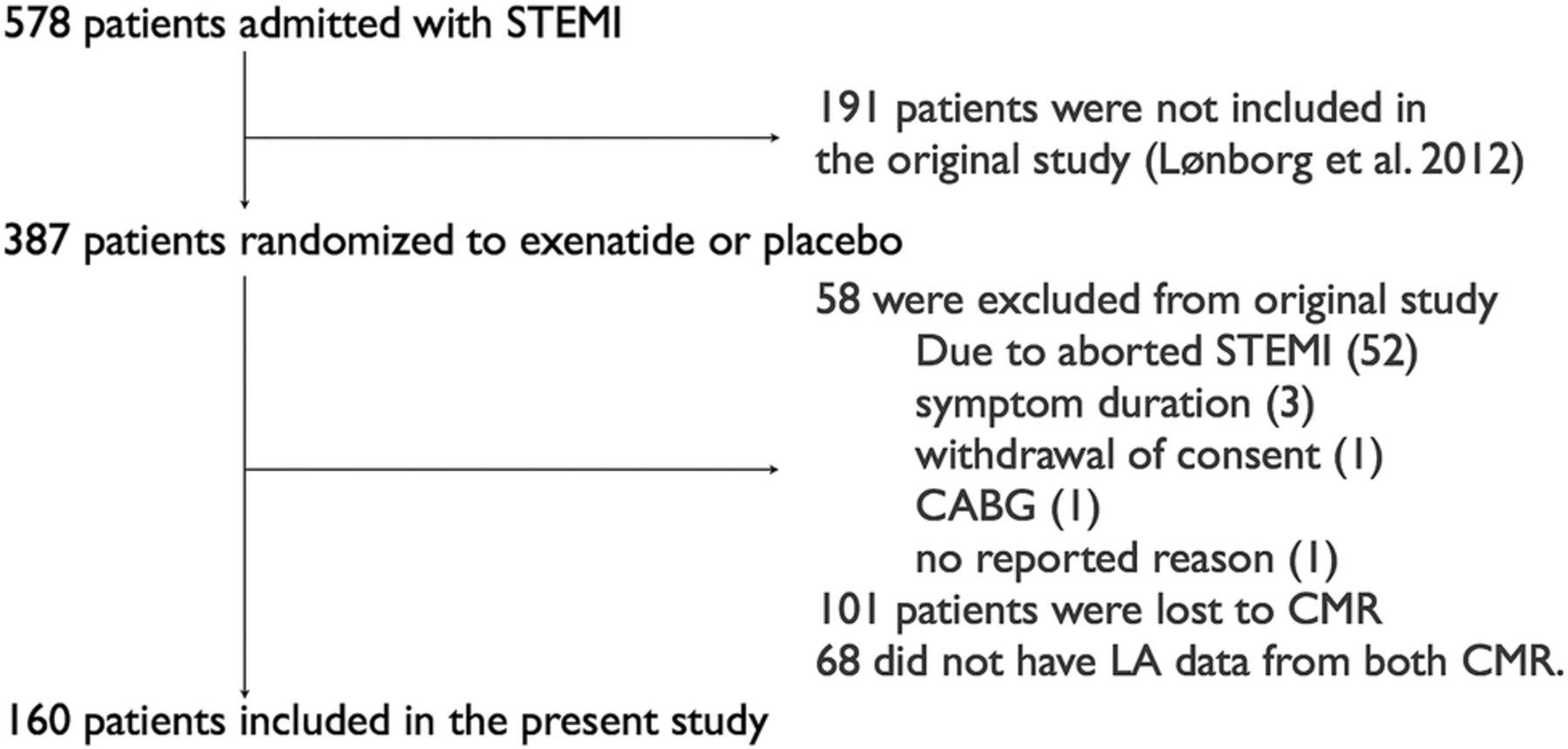
A total of 387 patients were included in the original study. Of these, 58 patients were excluded (due to aborted STEMI, symptoms duration >12 h, withdrawal of consent, or Coronary Artery Bypass Surgery Graft), 101 were lost to CMR (32 had contraindications, 30 refused, 12 either died, had reinfarction or stent-thrombosis, 18 refused or were incapable of completing MRI, 4 had a temporary pacemaker, 5 with no reason) and 68 were lost to follow-up or did not undergo the second CMR (figure 1). The excluded patients were older, had a higher incidence of hypertension and had shorter delay from first emergency contact to balloon. Table 1 shows the comparison between included and excluded patients.

Flow chart of study population. CMR, cardiovascular MR; LA, left atrium; ST-segment elevation myocardial infarction (STEMI), ST elevation myocardial infarction; CABG, coronary artery bypass graft surgery.
Among the included patients, the LAmin was 24.5 mL/m2 (IQR 18.8–29.0) at baseline and 24.8 mL/m2 (IQR 18.7–28.6) 3 months after STEMI (p=0.40). The LAmax was 48.3 mL/m2 (IQR 41.8–54.1) at baseline and 49.8 mL/m2 (IQR 40.4–57.2) 3 months after STEMI (p=0.014). The LAfc was 50.1% (IQR 45.4–54.7) at baseline and 50.9% (IQR 47.3–56.4) 3 months after STEMI (p=0.08). There was a wide distribution of LA change and individual patients experienced up to 92% LAmin remodelling, 61% LAmax remodelling and 57% LAfc remodelling during the 3 months following their STEMI (LA remodelling distributions are shown in figure 2). Table 2 shows the linear regression analyses of predictors for LAmin, LAmax and LAfc remodelling. The presence of hypertension is associated with adverse LAmin remodelling, but the LV mass index did only impact LAmax remodelling. Interestingly, the linear regression analyses showed significant association between the final infarct size and adverse LAmin and LAmax remodelling. Similar peak troponin T was associated with LAmin, LAmax and LAfc remodelling, but area at risk was only associated to LAmin and LAmax remodelling. Left ventricular ejection fraction at baseline was related to LAmax remodelling, but had no association with LAmin remodelling. In general, LA volume remodelling was associated with LV remodelling. Treatment with exenatide was not associated with remodelling of LAmin, LAmax or LAfc. We tested the correlation between CMR and echocardiography determined LA max and found that a linear correlation exists between the two (α=0.4, p<0.001, figure 3).

Distribution of left atrial (LA) remodel. Plot showing distribution of left atrium minimum volume (LAmin), LAmax and left atrium fractional change (LAfc) remodelling. Please notice that individual patients experience up to 92% LAmin remodelling, 61% LAmax remodelling and 57% LAfc remodelling during the 3 months following their ST-segment elevation myocardial infarction (STEMI).

Left atrium maximum volume (LAmax) for echocardiography and cardiovascular magnetic resonance (CMR). Plot comparing echocardiography with cardiovascular MR (CMR) for measurements of left atrial (LA) max volume at baseline. The red lines indicate cut-off values for enlarged LAmax. There is a linear relation between echocardiography and CMR, but please notice that α <1. The size of each point is determined by the degree of remodelling during follow-up.
LA remodelling and outcome
During the follow-up period of a median of 5.2 years (IQR 4.7–5.8), a total of 36 patients (23%) experienced MACE (3 patients died due to a cardiac cause, 6 patients died of a non-cardiac cause, 15 patients were admitted due to heart failure, 9 patients suffered a reinfarction and 3 patients had an implantable cardioverter defibrillator). Kaplan-Meier curves of MACE rates stratified by tertiles of LAmin, LAmax and LAfc remodelling are displayed in figure 4. Patients in the highest tertile of LAmin remodelling (>1.6 mL/m2) and LAmax remodelling (>4.6 mL/m2) were at a higher risk of suffering a subsequent clinical event (p=0.030 and p=0.018, respectively), while LAfc remodelling was not associated with MACE (p=0.90). Kaplan-Meier survival function estimates, stratified by the limits of agreement for LAmin, LAmax and LAfc, respectively, are displayed in figure 5. Patients with LAmin and LAmax remodelling above the 95% limits of agreement were at a higher risk of suffering a subsequent clinical event (p=0.010 and p=0.013, respectively), while LAfc remodelling was not associated with an unfavourable outcome (p=0.18)
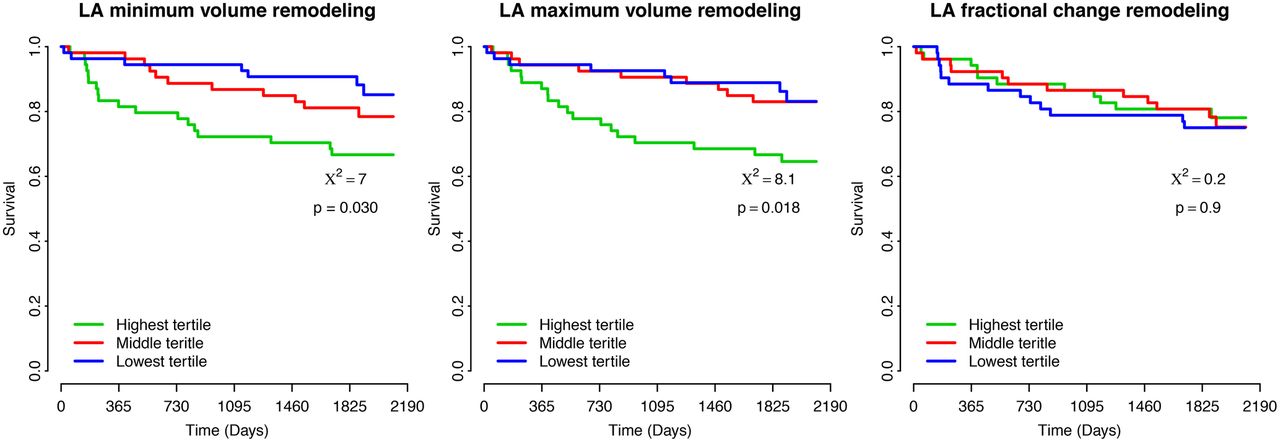
Outcome according to left atrial (LA) remodelling. Outcome stratified by tertile of left atrium minimum volume (LAmin) remodelling, LAmax remodelling and left atrium fractional change (LAfc) remodelling. The curves illustrate the event-free survival from the composite end point.

Outcome according to left atrial (LA) remodelling. Outcome stratified by the limits of agreement for left atrium minimum volume (LAmin), left atrium maximum volume (LAmax) and left atrium fractional change (LAfc), respectively. The curves illustrate the event-free survival from the composite end point.
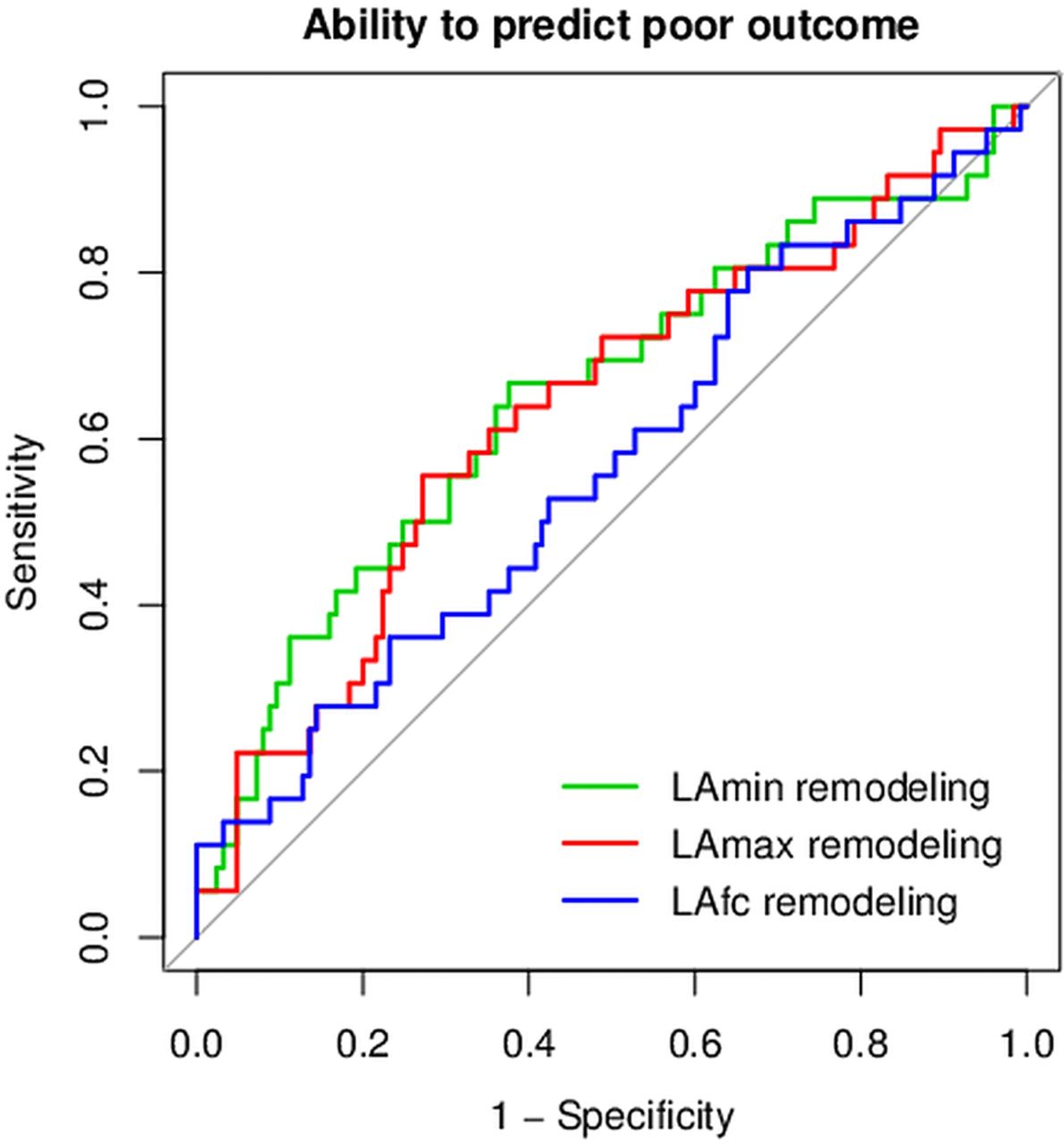
Receiver-operating characteristic curves are displayed in figure 6. The area under the curve was 0.66 (p=0.002) for LAmin remodelling, 0.64 (p=0.004) for LAmax remodelling and 0.57 (p=0.11) for LAfc remodelling. The optimal cut-off value for LAmin remodelling to predict a poor outcome defined by MACE was a 0.8 mL/m2 increase in LAmin volume and for LAmax remodelling the optimal cut-off value was a 0.1 mL/m2 increase in LAmax volume.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Receiver operating characteristic curve. Receiver-operating characteristic curves for left atrium minimum volume (LAmin) remodelling, left atrium maximum volume (LAmax) remodelling and left atrium fractional change (LAfc) remodelling displaying the ability to predict major adverse cardiac events after 3 years of follow-up.
Discussion
In this study, we evaluate predictors for LAmin, LAmax and LAfc remodelling following STEMI and assess the impact of LA remodelling on long-term outcome. The main findings of this paper are that adverse LAmin and LAmax remodelling following STEMI are associated with poorer outcome and LA remodelling is determined by final infarct size, peak troponin T, area at risk, the presence of hypertension, LV mass and LV remodelling. The results are considered to increase our knowledge on pathophysiology in a post-STEMI population.
As mentioned, owing to equalisation of LA and LV pressures during diastole and opening of the mitral valve, LA dilation over time after an acute myocardial infarction is affected by the same mechanisms as LV diastolic function, such as hypertension, renal impairment, diabetes, ischaemia and LV mass.15 In this paper, we demonstrate that a larger final infarct size measured by CMR and troponin T results in adverse LA remodelling, probably through reduced LV compliance and consequently increased LA pressures. Thus, infarct size should be added to the list of predictors for LA remodelling following an acute myocardial infarction.
LAmax increased slightly over time in this study, which is in accordance with previous observations.7 ,30 This is the first study to evaluate LAmin remodelling following an acute myocardial infarction. LAmin did not change over time in the general study population. However, there are important differences between LAmin and LAmax that may explain this discrepancy. In STEMI patients, baseline LAmax volume is not associated with acute LV function but determined by pre-existing conditions, whereas LAmin volume at baseline is determined by acute changes in LV function, for example, acute stunning and infarct size as well as pre-existing conditions.16 LAmax volume is mainly related to long-standing increased LV filling pressure, and LAmax remodelling is attributed to increased filling pressure. LAmin volume is more sensitive towards sudden changes in LV filling than LAmax volume. Both increased LV end-diastolic filling pressure and impeded emptying of the LA due to the reduced longitudinal LV fibre shortening affect LAmin remodelling. This may be an important player immediately after STEMI and probably leads to instant changes in LAmin volume. It may therefore be speculated that change in LAmax after STEMI is a slow adaptation to changing LV filling pressure, whereas change in LAmin over time is affected in the very early phase following STEMI by reduced LV longitudinal fibre contraction and also by changing LV filling pressure over time. Even though we did only observe a small change in mean LAmax and no change in mean LAmin, there were large individual differences in remodelling, far exceeding the 95% limits of agreement (figure 2).
Previous studies have identified LV mass, known hypertension, baseline LAmax and baseline estimated glomerular filtration rate as predictors for adverse LAmax remodelling.7 ,30 This study confirms most of these findings, but also extends the predictors to include LV remodelling, area at risk and extent of myocardial damage and infarct size (peak troponin T and final infarct size by CMR). The previous studies measure LA volume using echocardiography, which is easier to obtain than CMR, but also underestimates the LA volume by 20–35%.8 ,31 In our study, there was a good correlation between echocardiography and CMR assessed LAmax at baseline, but echocardiography showed a tendency to underestimate LAmax. Further, it is seen from figure 3 that echocardiography misclassifies a significant amount of patients.
As mentioned, LAmax is a well-known predictor in various diseases.1–10 Previous studies have also identified that adverse LAmax remodelling following an acute myocardial infarction is also related to impaired outcomes.7 ,17 Thus, the findings in this study confirm these previous observations. In addition, this study demonstrates that adverse LAmin remodelling is related to poorer outcome. Finally, despite the fact that LAfc remodelling was not related to the outcome in this study, LAfc measured at baseline has been shown to be a strong prognostic predictor.16 This study increases our knowledge on the basic pathophysiology of LA remodelling following STEMI. It also suggests that when studying LA physiology, it is important to look beyond LAmax and assess LAmin and LA function.
Limitations
A substantial number of potentially eligible patients were not included in this study, which may introduce a selection bias. The excluded patients may represent some of the most critically ill patients. Importantly, there was no difference in peak troponin T between the included and excluded patients. The patients in this study were randomised to either placebo or exenatide, but exenatide treatment did not influence LA remodelling. The sample size is relatively small; thus, the survival analyses presented in this study should be read cautiously due to the limited number of events. Owing to the many statistical comparisons, some significant p values may be observed by chance, and the results must be interpreted with this in mind.
Conclusions
This study extends our pathophysiological understanding of the predictors of LA remodelling to include LV remodelling, area at risk and infarct size. The extent of myocardial damage is a major determinant of LA remodelling following STEMI, and adverse LA remodelling is associated with an unfavourable prognosis and is a poor omen following STEMI.
Acknowledgments
The Research Foundation of The Department of Cardiology, Rigshospitalet and The Danish Heart Foundation supported this study financially.
References
Footnotes
Competing interests None declared.
Ethics approval The Danish National Committee on Biomedical Research Ethics.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.