Article Text

Abstract
The ischaemic cascade is the concept that progressive myocardial oxygen supply–demand mismatch causes a consistent sequence of events, starting with metabolic alterations and followed sequentially by myocardial perfusion abnormalities, wall motion abnormalities, ECG changes, and angina. This concept would suggest that investigations that detect expressions of ischaemia earlier in the cascade should be more sensitive tests of ischaemia than those that detect expressions appearing later in the cascade. However, careful review of the studies on which the ischaemic cascade is based suggests that the ischaemic cascade concept may be less well supported by the literature than assumed. In this review we explore this, discuss an alternative method for conceptualising ischaemia, and discuss the potential implications of this new approach to clinical studies and clinical practice.
- CORONARY ARTERY DISEASE
- MYOCARDIAL ISCHAEMIA AND INFARCTION (IHD)
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
The ischaemic cascade was initially described over 20 years previously,1 based on experiments in animals2–9 and humans,10–20 and refers to a temporal sequence of pathophysiological events that occur with increasing myocardial oxygen supply–demand imbalance. The ischaemic cascade has been described as occurring in the following sequence: metabolic alterations, inducible changes of perfusion, diastolic dysfunction, regional systolic wall motion dysfunction, ischaemic ECG changes and finally angina.1
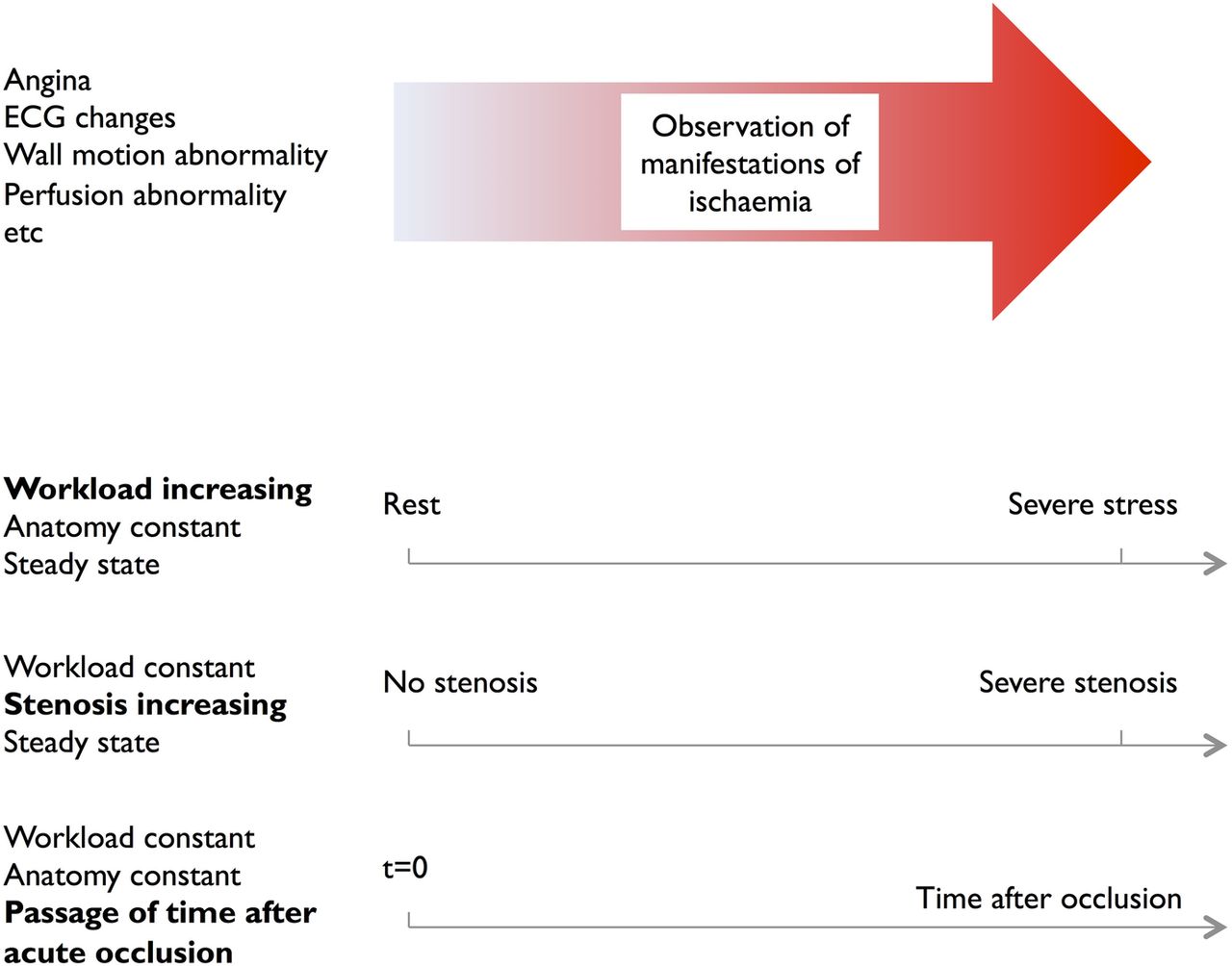
A cascade is a sequence of events, each of which triggers the next. Since causation is difficult to demonstrate directly, instead progression is demonstrated and causation inferred. To create progressively more intense ischaemia within an individual animal, so that the sequence of emergence of elements of the cascade can be identified, three broad approaches are possible (figure 1):
Progressively tighter stenosis, with workload kept constant and measured at steady state.
Progressive passage of time after a fixed acute occlusion, with workload kept constant.
Progressively increasing workload, with stenosis kept constant and measured at steady state.

Three different ‘x axes’ along which to rank states for ischaemia. The underlying hypothesis behind the ischaemic cascade is that the order of development of the various manifestations of ischaemia is the same for all three main ways of producing the ischaemia phenomenon. One approach is to ligate a coronary artery and monitor carefully in the ensuing seconds, with the temporal sequence of events showing the cascade sequence. A second is to progressively increase stenosis. A third is to progressively increase workload. If these three methods of inducing progressively more severe ischaemia produce manifestations in conflicting sequences, the ischaemic cascade concept is imperilled.
Assembling data from experiments that use different possibilities from the three ways of spreading ischaemia intensity on a spectrum relies on the assumption that the three different meanings of increasing ischaemia are equivalent. If the ischaemic cascade model is accurate, the order of events should be the same in all three. For example, it might be metabolic alterations first, followed sequentially by myocardial perfusion abnormalities, wall motion abnormalities, ECG changes and angina. If this assumption is not correct then we should be much more thoughtful when displaying illustrations of the process of ischaemia.
Metabolic alterations consist of the conversion from aerobic to anaerobic myocardial cell metabolism, thus producing biochemical changes of lactate, and cellular polarity. At a single-cell level a cascade is feasible, however cellular events will not occur synchronously in all cells beyond a stenosis. It is the later stages of the ischaemic cascade concept that are of clinical interest, but these can be subject to confounding effects of concomitant medications and varying degrees of coronary disease.
If the ischaemic cascade is not as solid a sequence as is often portrayed, this article discusses how the process of ischaemia could be conceptualised, the implications this has on the development of new tests of ischaemia and the implications for clinical practice.
Some clinicians and scientists may have already rejected the ischaemic cascade for not being true; for them, our paper is attacking a ‘straw man’. Unfortunately however, figures and slides are commonly shown21–24 and clinical studies (that use a single ‘gold standard’ for ischaemia) continue to assume that the cascade is true. This implies that rejection of the ischaemic cascade is not yet universal, and therefore our paper may be a useful enumeration of information.
Methods
Literature search was performed in accordance to the PRISMA statement.25 Studies were identified by searching Medline (1946 to February 2015) and Embase (1974 to February 2015), using the search term ‘ischaemic cascade’ (both English and American spellings). The search was restricted to English language and case reports were excluded. Reference lists of the retrieved articles (including reviews and editorials) were hand-searched for additional publications. The methodological validity of each included study was assessed using criteria for minimisation of bias, including definition and measurement of outcome, blinding, presence of a control group, and sample size (figure 2).
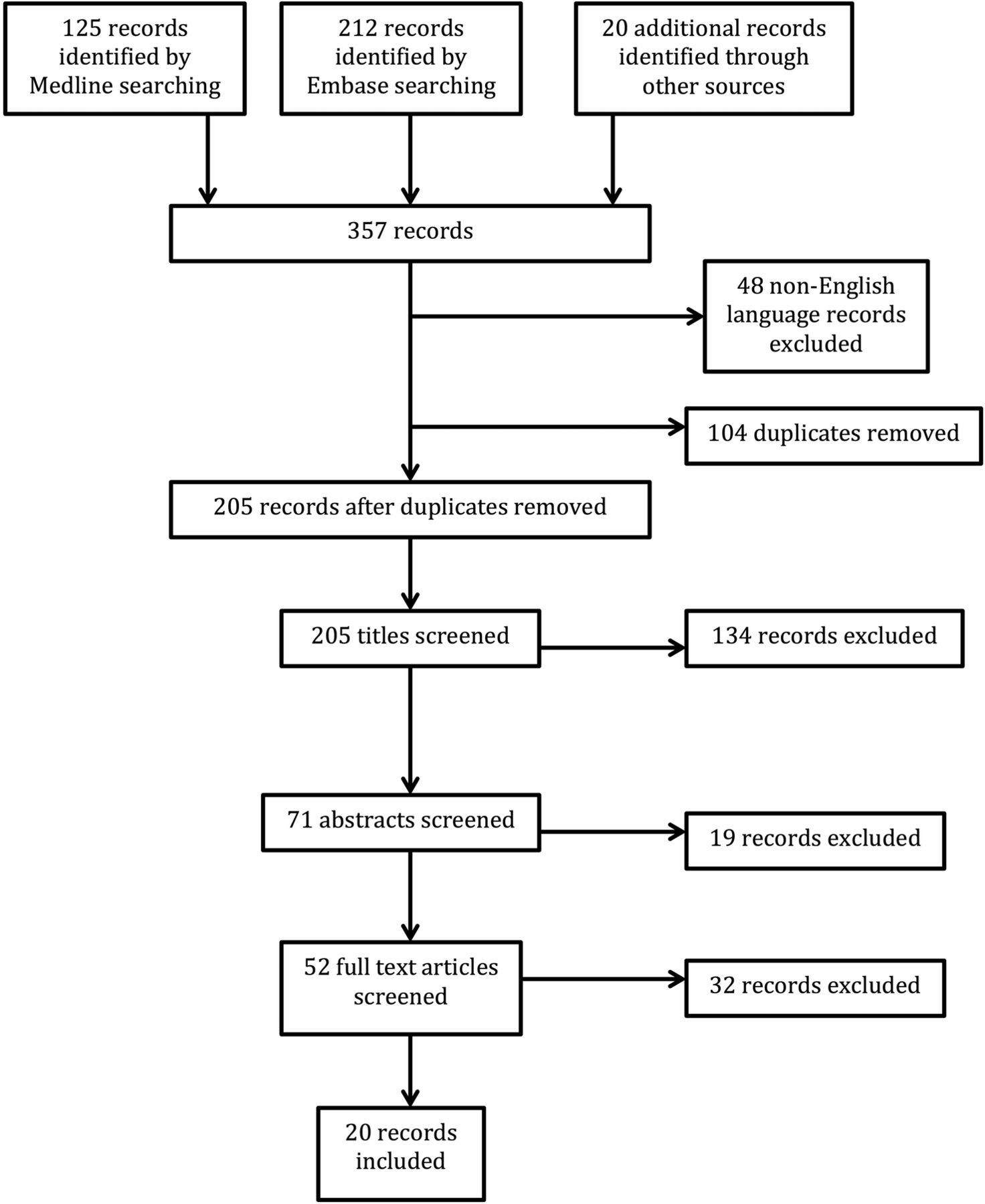
Flow diagram of literature search.
Foundations of the ischaemic cascade
The original paper,1 describing the ischaemic cascade, was based on human studies10–20 (table 1). The methods used to induce supply–demand mismatch were as follows: (1) coronary artery balloon occlusion,10–12 (2) atrial pacing tachycardia,13–15 (3) exercise testing16–19 and (4) spontaneous angina,20 that is, episodes of myocardial ischaemia at rest (either spontaneous or ergonovine induced) in patients with Prinzmetal's angina.
Summary of human studies that support the sequence of events in the ischaemic cascade
It is far from clear whether the events after abrupt occlusion of a coronary artery, coronary vasospasm, or increased myocardial workload, match what happens in incremental ischaemia with chronic coronary artery stenosis. Nonetheless, these studies10–20 show that angina and/or ST segment depression does not consistently accompany ischaemia. More importantly, they show that when angina and/or ST segment depression do occur, their temporal relationship with other elements of the ischaemic cascade is not always what would be expected if the cascade is correct. Studies that support the sequence of events in the ischaemic cascade are summarised in table 1.10 ,11 ,13–15 ,17 ,19 ,20 ,26–31 Table 2 summarises studies that contradict the sequence of events described in the ischaemic cascade.12 ,16 ,18 ,32–34
Summary of human studies illustrating the concept of the ischaemic constellation
Sequence mismatches
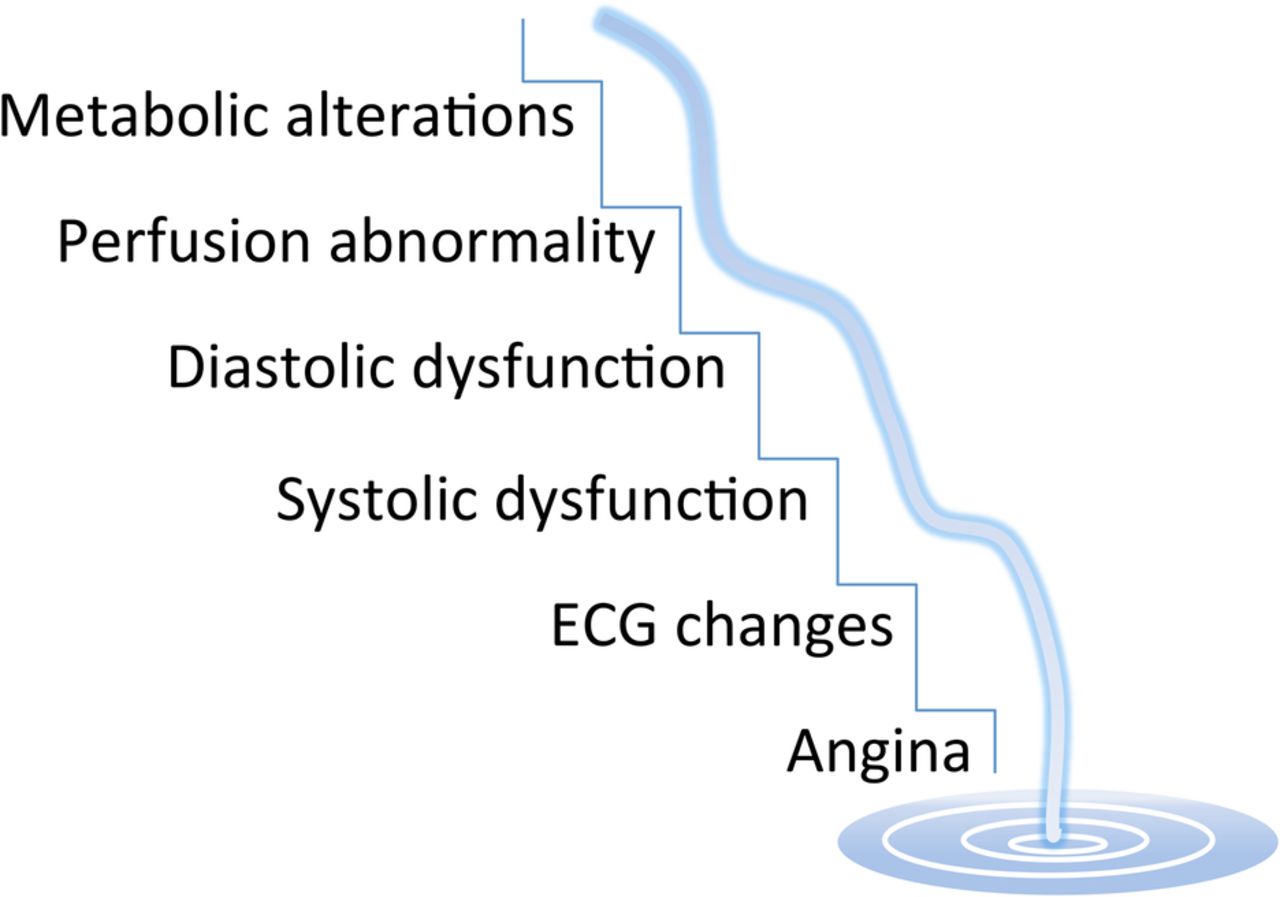
The term ‘cascade’ is a reference to a sequence of events, each triggering the next. It is used to describe waterfalls, where what falls to one level becomes available to fall to the next level down (figure 3). If, however, events are observed to occur out of sequence, then impression of causality (or at least ordering) conveyed by the term ‘cascade’ may not be secure.

Waterfall analogy of the ischaemic cascade. In a cascade the water falling down one step is the water that is available to later fall down the next step. The water must fall down the steps in sequence. If water was found to be moving out of sequence, that is, up and down between steps in an unpredictable way, then it is not a cascade.
Close inspection and comparison of the results of different studies, included in the original ischaemic cascade concept paper,1 suggests that the sequence of events described is not conserved across patients (table 2). For instance, one study18 found that when diastolic dysfunction was measured using pulmonary artery pressure during exercise, the onset of ST segment depression occurred before diastolic dysfunction in 38% of episodes, was simultaneous with it in 38% of episodes, and followed it in only 24% of episodes.
In another study of patients with angina who underwent continuous ECG and echocardiographic monitoring during dipyridamole infusion, the sequence of ischaemic events observed were markedly variable.33 Of those patients who developed echocardiographic and ECG changes/angina, only about half exhibited regional wall motion abnormalities first, while the remaining half exhibited ECG changes and or angina first.
In a further study of 707 consecutive patients screened after dobutamine or bicycle ergometer stress echocardiography, only 12% of patients followed the classical ischaemic cascade.32 Only 30% had regional perfusion defects prior to the onset of abnormal wall motion, whereas 22% had perfusion defects seen during or after the onset of abnormal wall motion.32 These findings and those of others33 ,34 contradict the sequence of events described in the ischaemic cascade.
The ischaemic constellation
In light of the data conflicting with the concept of any single ischaemic cascade, perhaps the concept of a single sequence of stepwise causality needs to be re-evaluated.
In a true cascade, where each event leads to the next in succession, there is no doubt regarding the causal sequence of events. For example, in the complement cascade of the immune system each stage is necessary for the next to occur.
In contrast to a cascade model of ischaemia, we propose that a more befitting model of myocardial ischaemia may be the ‘ischaemic constellation’; a collection of observations that may occur in a variety of sequences. An ischaemic constellation would include all clinical aspects of the cascade, including angina, myocardial perfusion abnormalities, ST segment depression and wall motion abnormalities, without the artificial prerequisite of a need to occur in a particular preordained order. Such a constellation would explain the similar rate of positivity of tests of ischaemia and their variable ordering of apparent sensitivity in different patients.35
Conceptualising ischaemia in this way would perhaps be more consistent with clinical practice. Currently, clinicians who would otherwise be restricted by the concept of the ischaemic cascade tend to adopt an approach to ischaemia testing that is driven by an underlying pretest suspicion as to the likelihood of ischaemia. For example a negative ischaemia test in a patient with typical angina will trigger a further investigation, with a test that may not necessarily be upstream the cascade. This behaviour is not consistent with trust in an ischaemic cascade. It suggests that physicians are ready to accept that it is biologically plausible that both tests are ‘correct’ but having different results. Clinically this means that physicians may tailor the use of specific ischaemia tests to specific populations.36 However, this contrasts with clinical trials comparing ischaemia tests in which investigators appoint a ‘gold standard’, which is assumed to be the most sensitive test in all patients.37 ,38 Such an approach does not appreciate variation between individuals and therefore squanders an opportunity to understand which tests are most appropriate for specific populations.
Scientific and clinical implications
The scientific and clinical implications of a ‘constellation’ model of ischaemia, rather than the ‘cascade’ model, are pertinent to the key question of whether ischaemia is present when two tests have conflicting results. This is a common challenge in the interpretation of validation studies of new tests of ischaemia. Currently any disagreement of the new test with the test appointed as ‘gold standard’ is interpreted as an inaccuracy of the new test. Recently this approach has been demonstrated to be flawed.35 ,39
A ‘constellation’ model of ischaemia could provide a solution to the problem of how to interpret investigations when conflicting test results coexist in the same patient and thereby resolve a crisis for those relying on the ischaemic cascade as a schema for interpretation of events. The constellation would suggest that in such a situation both tests may be correct, but one biological event may have occurred at a lower degree of ischaemia than the other event in that particular individual. Importantly, the converse may be true in another individual—a possibility that cannot be encompassed with a cascade.
The ‘constellation’ does not provide a solution to the problem of how to differentiate a false-positive test from the situation of conflicting results from two tests in the same patient. One way to resolve this would be a study design that doesn't simply compare one test to another, but evaluates the test's ability to predict improvement of symptoms when the patient receives appropriate therapy, such as antianginal medications. For example, a trial design that may help evaluate the clinical accuracy of a test may involve randomising patients, who test negative or positive for an investigation of ischaemia, to antianginal medications or placebo, and measuring symptomatic and or functional outcomes (figure 4). An objective assessment of patient functional status such as cardiopulmonary exercise testing could be used to assess the patient's symptoms and functional capacity, thus providing an objective, reproducible and quantifiable measure. The most reliable test would be that which most consistently predicts whether the patient will improve symptomatically, or functionally (in patients with ‘silent’ ischaemia), with treatment versus placebo. Such an approach uses the patient's symptoms and functional capacity (with placebo control) as the reference standard.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Illustration of a trial design to help evaluate the clinical accuracy of a test of ischaemia. The best test would result in improved symptoms in those patients who test positive and are randomised to antianginal treatment, with no change in symptoms in those who test positive and are randomised to placebo, or after treatment for those who test negative.
It should be noted that there are several different causes of ischaemia and therefore, the treatment success of individual pharmacological agents will vary according to the cause of ischaemia. Our study design would therefore require identification of the predominant cause of ischaemia prior to enrollment of the patients into the study. For example, separating those with angina and epicardial coronary disease from those with angina and ‘normal’ epicardial arteries. This is not unusual in this field, for example the fractional flow reserve (FFR) studies have routinely stipulated a minimum amount of epicardial disease that patients must have prior to enrollment.40–42
The external applicability of a clinical trial result to different patient populations applies to all clinical studies. The efficacy of any given treatment will vary according to the individual characteristics of the population being treated. While our study design addresses the concept of an ischaemic constellation the external applicability of its results to different patient populations will be vulnerable to the limitations of any clinical trial. While this has been commonly acknowledged in pharmacology studies (eg, ACE inhibitors in black vs white populations43) it is only now being more widely acknowledged in the ischaemia diagnostic domain. Recent studies have confirmed that the accuracy of diagnostic tests will vary according to the underlying distribution of stenoses in differing populations.44 Furthermore, the treatment threshold of certain diagnostic tests may vary according to age and gender.45 ,46
Despite the above limitations, which are shared with existing trial design, the constellation model begins the process of acceptance that a single gold standard test for ischaemia may not be possible. The reasoning above suggests that there may well be multiple tests, each individually accurate in describing one facet of the constellation, but mutually conflicting without any necessarily being erroneous. Explicit public recognition of this might open the way for clinicians to interpret studies comparing ischaemia tests in a more rational manner. A first step to permitting this personalised and integrative cardiology would be to recognise that information from these quantitative tests is continuous rather than dichotomous.
Summary
In this review we have indicated that (1) it is unwise to describe the clinical manifestations of ischaemia as a cascade, (2) it may be unwise to speak of the sensitivity or specificity of a test for ischaemia, since there may be no true gold standard and (3) when the results of clinical tests differ we may need to take a more sophisticated approach than saying one is right and the other is wrong.
Conclusion
For decades the ischaemic cascade has been at the foundations of teaching regarding diagnosis of ischaemia. Review of the source literature suggests, however, that it is not correct, with components of the cascade often occurring out of sequence. Presenting information known to be incorrect may be convenient for the short-term aim of providing educational content, but does not necessarily help the long-term aim of improving scientific knowledge about important processes in humans.
We propose the ‘ischaemic constellation’, a paradigm that recognises no single gold standard test for ischaemia and that different markers of ischaemia may become abnormal at different stages depending on the individual, the nature of stimulus to ischaemia, and other factors, and that results may vary between one episode and another. This ‘constellation concept’ calls for a new way of evaluating ischaemia tests that places the patient as the ‘gold standard’.
References
Footnotes
Contributors All the authors have read and approved the manuscript. AM reviewed the literature and wrote the manuscript. SS designed the concept, wrote the manuscript and revised it critically for important intellectual content. CC edited the manuscript. DPF designed the concept for the review and wrote the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.