Article Text

Abstract
Objectives To explore the ethnic differences in patients undergoing aortic valve (AV) intervention for severe aortic stenosis (AS) in Leicestershire, UK.
Methods Retrospective cohort study of all surgical aortic valve replacement (SAVR) and transcatheter aortic valve implantation (TAVI) at a single tertiary centre between April 2017 and March 2022, using local registry data.
Results Of the 1231 SAVR and 815 TAVI performed, 6.5% and 3.7% were in ethnic minority patients, respectively. Based on the 2011 Census data for those with a Leicestershire postcode, crude cumulative rate of SAVR (n=489) was 0.64 per 1000 population overall and 0.69, 0.46 and 0.36 in White, Asian and Black populations, respectively; and 0.50 per 1000 population overall for TAVI (n=383), with 0.59, 0.16 and 0.06 for White, Asian and Black populations, respectively. Asians undergoing SAVR and TAVI were 5 and 3 years younger, respectively, than white patients with more comorbidities and a worse functional status.
The age-adjusted cumulative rates for SAVR were 0.62 vs 0.72 per 1000 population for White and Asian patients and 0.51 vs 0.39 for TAVI. Asians were less likely to undergo SAVR and TAVI than White patients, with a risk ratio (RR) of 0.66 (0.50–0.87) and 0.27 (0.18–0.43), respectively, but the age-adjusted RR was not statistically significant.
Conclusion The crude rates of AV interventions are lower in Asian patients compared with the White population in Leicestershire, although age-adjusted rates were not statistically different. Further research to determine the sociodemographic differences in prevalence, incidence, mechanisms and treatment of AS across the UK is required.
- Aortic Valve Stenosis
- Transcatheter Aortic Valve Replacement
- Heart Valve Prosthesis Implantation
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Disparities in aortic valve (AV) intervention rates in ethnic minorities have been well described, predominantly in US-based studies that have shown under-utilisation of surgical aortic valve replacement (SAVR) and transcatheter aortic valve implantation (TAVI) in Black and Latino patients. However, little is known about intervention rates among ethnic minorities in the UK.
WHAT THIS STUDY ADDS
This is the first UK-based study to explore ethnic differences among patients undergoing AV intervention for aortic stenosis (AS). Our data shows that overall rate of AV intervention is lower in Asians, with more SAVR taking place at a younger age and very few TAVIs, compared with the White population residing in Leicestershire, UK. However, after age adjustment, these differences did not remain statistically significant.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The current data are not completely reassuring that ethnic variations in AV intervention do not exist in an ethnically diverse region of the UK. Further research to determine potential cultural differences in intervention rates and sociodemographic differences in prevalence, incidence, mechanisms and treatment of AS across the UK is required to identify potential health inequalities and tailor future research strategies and healthcare policies to address these.
Introduction
Aortic stenosis (AS) is the most common heart valve disease requiring intervention in high-income countries affecting ~2.7 million people in Europe and 4.9 million in North America.1 The only definitive treatments are either surgical aortic valve replacement (SAVR) or transcatheter aortic valve implantation (TAVI). Current guidelines recommend intervention once symptoms or left ventricular dysfunction develop, but there are variations in routine clinical practice.2 3 American studies have highlighted that Black and Asian patients are less likely to be diagnosed with AS or undergo aortic valve (AV) intervention than White patients.4–8 Ethnic minorities are also under-represented in clinical trials, with the recently published UK TAVI trial including only 3.5% ethnic minorities.9
In the UK, ethnic minorities make up 14% of the population,10 with the burden of cardiovascular disease being disproportionally higher in these groups.11 However, there are no data on the ethnic characteristics of patients being treated for AS in the UK. Leicestershire represents an ethnically diverse population, with 20% ethnic minorities and provides an opportunity to explore differences in the make-up of patients being treated for AS. Ethnic differences in the rates of other cardiovascular interventions have previously been highlighted in this population.12 13 Hence, the aim of the study was to explore the ethnic differences among patients undergoing AV intervention in the Leicestershire population.
Methods
Study design and population
This was a retrospective cohort study of all SAVR and TAVI procedures carried out at a large single-centre (Glenfield Hospital, Leicester), the primary provider of tertiary cardiology services to the people of Leicestershire, between 1 April 2017 and 31 March 2022. The study population data was obtained from routinely collected, compulsory audit data, which includes all SAVR and TAVI procedures undertaken. The registry is up to date and regularly audited, and hence provides a complete reflection of all procedures undertaken. Procedures are also offered to patients from neighbouring counties, which overlaps with other tertiary centres. Therefore, only patients with a Leicestershire postcode undergoing SAVR or TAVI at Glenfield Hospital were used to calculate the procedure rates. The population at risk (exposed population) was the adult population of Leicestershire, the data for whom was obtained from the UK National Census of 2011, via the Office for National Statistics.10 This was the latest dataset available at the time of the analysis.
Baseline demographics, including age, sex, ethnicity, cardiovascular risk factors, comorbidities, functional status, operative risk, procedural characteristics and postprocedural outcome data, were extracted from the registry. Functional status was assessed, using the Katz Index of activities of daily living (ADL), on a scale of 0–6 (from 0=very dependent to 6=independent)14 and clinical frailty using the Canadian study of health and ageing clinical frailty scale.15 Operative risk was calculated using the European System for Cardiac Operative Risk II (EuroSCORE II) tool that is widely used in the clinical setting.16 All data were anonymised before analysis. We excluded patients with ethnicity not stated, previous AV intervention and those with mixed AV disease where the predominant lesion was aortic regurgitation. Only patients undergoing SAVR (with or without coronary artery bypass grafting (CABG)) or TAVI for severe native valve AS were included. We used the following ethnicity categories for coding17: White, Asian, Black, mixed and ‘other’; the latter three groups were excluded from the main analysis given the small numbers of patients undergoing intervention, but absolute numbers are presented.
Statistical analysis
Following determination of the absolute numbers of procedures for each ethnic group in the overall population, crude cumulative incidence rates of SAVR and TAVI per 1000 population in Leicestershire were calculated for White and Asian patients with a Leicestershire (‘LE…’) postcode. Patients were split into the following age groups: <55, 55–64, 65–74, 75–84 and 85 years or above. The crude incident rates were calculated for the overall population and each age group, where the numerator consisted of number of events for each procedure in each ethnic group and the denominator was the respective population of Leicestershire from the 2011 Census.
Due to differences in age structure between the White and Asian populations (Asians were on average younger), the rates of SAVR and TAVI were adjusted for age using indirect standardisation with Leicestershire population from the 2011 Census serving as a reference. Age-adjusted cumulative incidence rates were estimated for each procedure and each ethnic group within each age group and the overall population. The total age-adjusted rates for SAVR and TAVI were obtained from the sum of expected age-adjusted events for each ethnic group, divided by respective population.
Crude risk ratios (RRs) for Asian compared with the White population were calculated for each age group. The total age-adjusted RR for Asian compared with the White population was also calculated using Mantel-Haenszel method.18 Analyses were performed using STATA V.17.
Results
Number of procedures
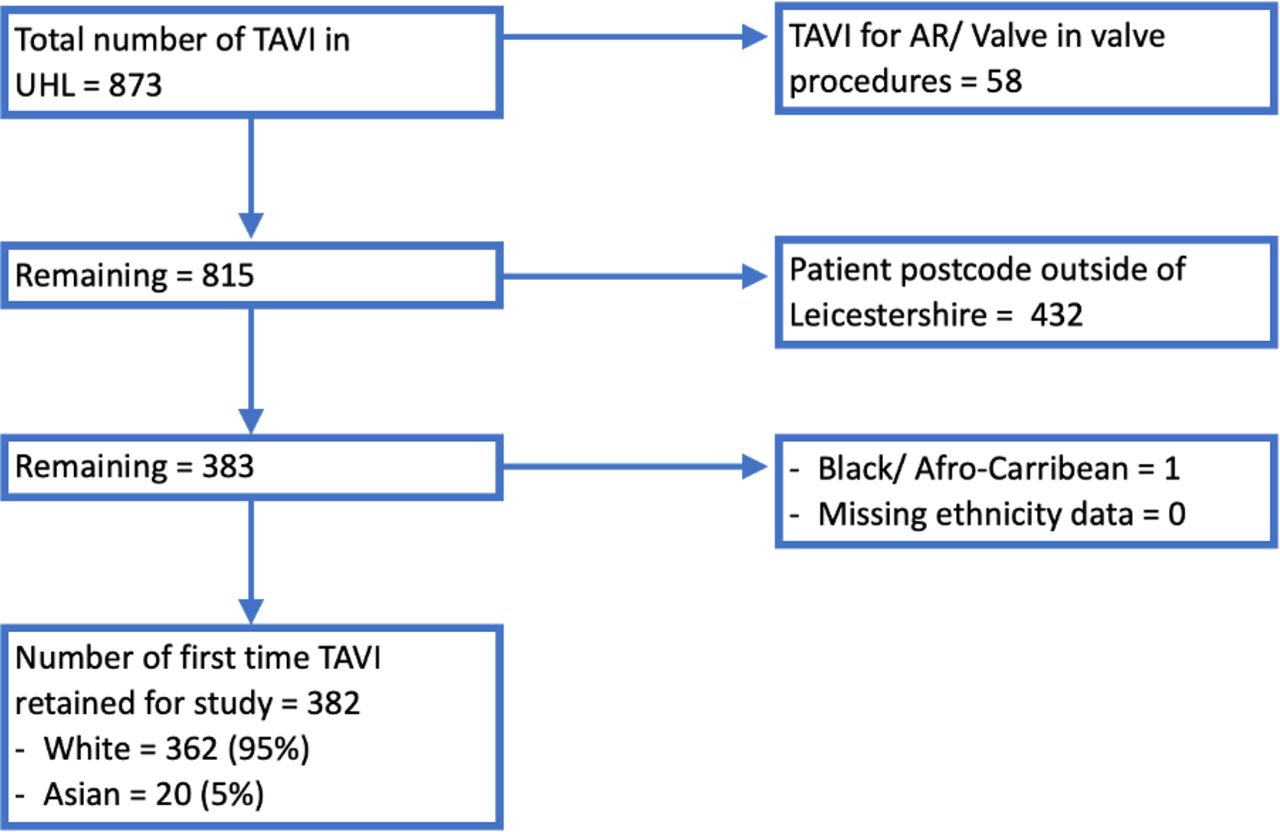
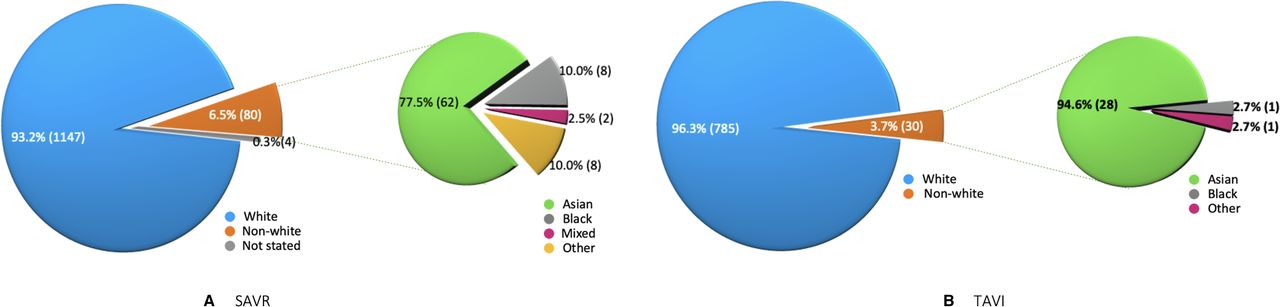
Between 1 April 2017 and 31 March 2022, a total of 1231 patients underwent SAVR (figure 1) and 815 underwent a TAVI (figure 2) for AS at Glenfield Hospital. Of those undergoing SAVR, 1147 (93.2%) were White, 62 (5%) Asian, 8 (0.6%) Black, 2 (0.2%) mixed and 8 (0.6%) other ethnicities (figure 3A). Ethnicity was not stated in four cases. Of those undergoing TAVI, 785 (96.3%) were White, 28 (3.4%) Asian, 1 (0.1%) Black and 1 (0.1%) other (figure 3B). When including only those with a Leicestershire postcode, the numbers were as follows for SAVR (n=489): White 421 (86.1%), Asian 56 (11.5%), Black 6 (1.2%), mixed 1 (0.2%), other 4 (0.8%), not stated 1 (0.2%); and for TAVI (n=383): hite 362 (94.5%), Asian 20 (5.2%), Black 1 (0.3%). After exclusion of individuals from Black, mixed and other ethnic minority groups due to low numbers, a total of 477 patients having SAVR and 382 patients having TAVI were included in further analysis.

Flowchart of the study population for SAVR at Glenfield Hospital, Leicester, from April 2017 to March 2022. AR, aortic regurgitation. UHL, University Hospitals of Leicestershire. SAVR, surgical aortic valve replacement.
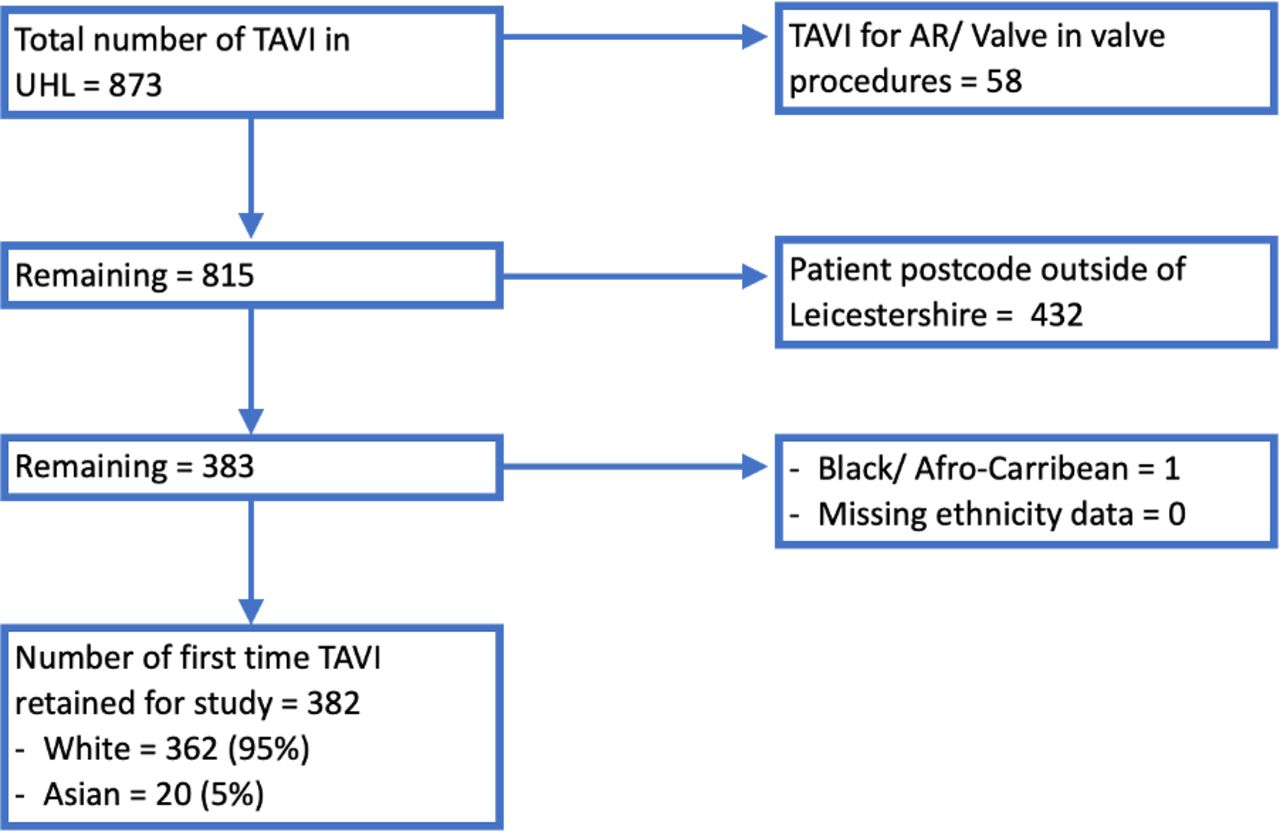
Flowchart of the study population for TAVI at Glenfield Hospital, Leicester, from April 2017 to March 2022. AR, aortic regurgitation, AS, aortic stenosis; TAVI, transcatheter aortic valve implantation.

{kind=link}
{kind=link}
{kind=link}
Pie charts showing the ethnic split of all patients undergoing surgical aortic valve replacement (SAVR) (A, left) and transcatheter aortic valve implantation (TAVI) (B, right) at Glenfield Hospital, Leicester, UK between April 2017 to March 2022.
Patient characteristics
The baseline characteristics of patients undergoing AV intervention, stratified by ethnicity, are shown in table 1. Asians undergoing SAVR were significantly younger by 5 years, had significantly higher rates of diabetes mellitus and stroke and lower body mass index and rates of smoking, compared with the White group. There was no difference in EuroSCORE II. Asians undergoing TAVI were also younger by 3 years and had significantly higher rates of diabetes mellitus and coronary artery disease, with lower rates of stroke and smoking compared with White patients. Asian patients had a significantly worse functional status compared with White patients demonstrated by the Katz Index of ADL Score (4.8±0.7 vs 5.4±0.7, p=0.0002); however, there was no difference in frailty.
Demographic, clinical and procedural characteristics
Procedural characteristics are also presented in table 1. Procedural urgency for SAVR was similar for both ethnicities. Asians were more likely to require TAVI in the context of an urgent presentation than Whites (20% vs 10%), even though this did not reach statistical significance, given the low numbers in the Asian subgroup (n=4). Concomitant CABG performed with SAVR tended to be more frequent in Asian than White patients (41% vs 28%, p=0.061).
Cumulative rates of SAVR/TAVI by ethnicity
In the 2011 Census, adult (≥18 years) Leicestershire population of 768 357 consisted of 611 058 (80%) White individuals, 122 892 (16%) Asian and 16 473 (2.1%) Black ethnic groups. The crude cumulative SAVR rate for the overall Leicestershire population during the study period was 0.64 per 1000 population, with the rate being 0.69, 0.46 and 0.36 per 1000 for White, Asian and Black populations, respectively. For TAVI, the crude cumulative procedure rate was 0.50 per 1000 for the overall Leicestershire population, with the rate being 0.59, 0.16 and 0.06 per 1000 for white, Asian and Black populations, respectively.
The crude cumulative rates of both procedures were adjusted for age due to the differences in the age structure of the White and Asian populations, with the Asians being younger. Due to smaller numbers in the Black and other subgroups, this was only done for the White and Asian subgroups. The age-adjusted procedure rates for SAVR were 0.62 per 1000 population for white and 0.72 per 1000 population for Asian subgroups. The age-adjusted procedure rates for TAVI were 0.51 per 1000 population for White and 0.39 per 1000 population for Asian subgroups. The crude and age-adjusted cumulative rates for different age groups are also shown in tables 2 and 3.
Crude and age-adjusted cumulative rates of SAVR for overall population and by age groups
Crude and age-adjusted cumulative rates of TAVI for overall population and by age groups.
RRs for AV intervention by ethnicity
The RRs for incidence rates of SAVR and TAVI are shown in tables 2 and 3, respectively. For the overall population, Asians were less likely to undergo AV intervention compared with Whites with an RR of 0.66 (95% CI 0.50 to 0.87) and 0.27 (95% CI 0.18 to 0.43) for SAVR and TAVI, respectively. However, the age-adjusted RRs were not statistically significant: 1.19 (95% CI 0.90 to 1.58) for SAVR and 0.77 (95% CI 0.51 to 1.26) for TAVI.
Discussion
This is the first UK-based study to explore the ethnic differences in the rates of SAVR and TAVI for AS and has a number of novel findings. First, our data shows that the overall number of procedures, in particular TAVI, is disproportionately lower in ethnic minority patients, accounting for only 3.7% of all TAVIs over the last 5 years. Second, this study highlights some important differences in the patient characteristics of Asian and White patients undergoing SAVR and TAVI. Asian patients undergoing SAVR were on average 5 years younger than their White counterparts with higher percentages of diabetes and stroke and with a trend towards more concomitant CABG (41% vs 28%). Asian patients undergoing TAVI were on average 3 years younger than White patients, had a greater prevalence of diabetes and coronary artery disease and a worse functional status. However, the rate of TAVI procedures in Asians>85 years age group was nearly half of that in the White patients.
Asians are the largest ethnic group within the UK at 7% and in Leicestershire they constitute a much larger proportion of the population at 16%.10 Hence, the crude rates from our data suggest that TAVI is either being offered, performed or is required less frequently in ethnic minority patients. Possible reasons for fewer TAVIs in Asians may be the earlier presentation with severe AS at a younger age, leading to more SAVR being performed. Alternatively, given the greater comorbidity burden and the higher perceived risks, the possibility of not being offered TAVI and being more likely to opt for medical management, as well as patients declining intervention at an older age could also play a role.
Referral patterns for TAVI in ethnic minorities explored in a previous study subanalysis showed that 20.5% of ethnic minority patients were hospitalised for heart failure or AS related symptoms at the time of referral.6 Similarly, in our cohort, 4 (20%) of 16 Asian patients (vs 10% of White patients) underwent an urgent TAVI. This may be suggestive of delayed presentation and diagnosis, or alternatively, delayed referral for consideration of TAVI. However, this is speculation as the exact reasons for procedural indication were not explored. Furthermore, studies have shown that postprocedural mortality remains similar among ethnic groups but procedural outcomes, by ethnicity varies. For example, Black patients may require prolonged ventilation and hospitalisation, have renal failure, bleeding complications that require reintervention and higher rates of rehospitalisation post-SAVR.4 5 Data for other ethnic groups is limited and requires further investigation.
Potential reasons for these disparities are thought to be complex and multifactorial, such as lower referral rates and higher rates of patients declining intervention.5 7 19 Lower socioeconomic status including education level and employment status may also impact a patient’s understanding of the need to seek medical attention and accept treatment. Furthermore, socioeconomic status and ethnicity may also influence physicians’ perception of patients, affecting the consultation dynamics.20 Language barrier and cultural differences21 may be a further hindrance for patients to express their symptoms or seek healthcare in the first place. In the US, Black and Latinos are relatively under-represented in the primary healthcare system and less likely to be referred to cardiologists or cardiac surgeons. However, a review of cardiovascular care delivered in the National Health Service (NHS) in the UK has shown that Asians have higher levels of presentation and better access to secondary care management22 but not necessarily primary care than other ethnic minority groups.23
Some studies have suggested that the lower rates of intervention in ethnic minorities may represent a lower prevalence of AS in these groups.5 However, there is no conclusive data on the true prevalence or incidence of AS by ethnicity in the UK. OxValve, a large echocardiographic screening study identified 1.3% of individuals>65 years, had undiagnosed AS. However, this cohort comprised of predominantly white patients (99%) in an affluent setting, which is not reflective of the ethnically diverse UK population.24 In a US-based echocardiographic study that included 272 429 patients, the prevalence of severe AS was estimated as 0.91% in white patients and 0.29% in black patients.25 Data on AS prevalence from low-income countries or South Asia is very limited.26 Two Indian studies including a total of 17 017 patients estimated a prevalence of isolated AS at 4.8%–7.3%, of which 58%–65% was attributable to degenerative (trileaflet) AS. Clinical presentation for AS was approximately a decade earlier in these two South Asian studies in comparison to Western data.27 28 This may be attributable to an accelerated process of disease progression due to the higher burden of cardiovascular risk factors. In the UK, cardiovascular mortality is the leading cause of death among Asians, but despite this, their life expectancy is on average 3 years higher than the white population.29 Hence, the presumption of a lower life expectancy among ethnic minorities to be a contributing factor to a lower prevalence of AS or the need for SAVR/TAVI is unlikely to be the case, at least in the UK population. The Multi-Ethnic Study of Atherosclerosis adjusted analyses have also shown no difference in AV calcification prevalence and progression among whites, blacks, Hispanics and Chinese.30
Ethnic minorities are known to be under-represented in cardiovascular research including studies in AS, despite having a high burden of cardiovascular risk factors and disease. Hence, the understanding of pathophysiology, epidemiology, presentation and management of AS in ethnic minorities is limited. Existing guidelines may not be generalisable to these patient groups. Therefore, sociodemographic differences in the incidence, prevalence, treatment and outcomes of patients with AS need to be investigated on a national level within the diverse UK population.
Limitations
These are results from a single-centre observational study that may not be generalisable to the rest of the UK population or other ethnicities, but significant variance is unlikely given the uniform provision of the NHS services across the UK. As analysis was limited to those with a Leicestershire postcode, data related to 57% of the procedures was excluded, the remaining 43% of patients were further divided into age groups leading to very small number of procedures in certain subgroups, as reflected by the wide confidence intervals, which may affect the precision of estimates and limit the statistical power of comparisons and conclusions. In addition, it was not possible to assess for differences by sex or correct for confounders other than age due to small sample size. AV intervention rates in other ethnic groups than white and Asian were not explored due to small numbers that would preclude any reliable statistical comparison. Our data cannot take into consideration referral patterns or identify patients that were not offered or may have declined intervention. Ethnic demographics were self-reported and accurate categorisation of mixed ethnicities cannot be assumed. Ethnicity data by region from the UK Census 2021 was not available at the time of analysis.
Conclusions
The crude rates of AV interventions are lower in Asian patients compared with the White population in Leicestershire, although the age-adjusted rate was not statistically different. Further research to determine the sociodemographic differences in prevalence, incidence, mechanisms and treatment of AS across the UK is required to identify potential health inequalities and tailor future strategies for research and healthcare policies to address these.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants. The study was approved by the institution’s review board and conducted as an audit. According to the Health Research Authority (HRA) decision algorithm, the study was not classified as research requiring formal HRA or a research ethics committee review. As data was obtained from local registry data/audit, individual patient consent was not obtained in accordance with local institutional review board.
References
Footnotes
Twitter @DrSaadiaAslam
Contributors AS conceived the research idea. SA and MAP contributed to data acquisition. SA, SS and CPN conducted the statistical analysis. SA and AS drafted the manuscript and are responsible for the overall content as guarantor and thereby accept full responsibility for the completed work and conduct of study. All the authors contributed to the critical revision of the manuscript for key intellectual content and approved the submitted version of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.