Article Text

Abstract
Objective The training of interventional cardiologists (ICs), non-interventional cardiologists (NICs) and cardiac surgeons (CSs) differs, and this may be reflected in their interpretation of invasive coronary angiography (ICA) and management plan. Availability of systematic coronary physiology might result in more homogeneous interpretation and management strategy compared with ICA alone.
Methods 150 coronary angiograms from patients with stable chest pain were presented independently to three NICs, three ICs and three CSs. By consensus, each group graded (1) coronary disease severity and (2) management plan, using options: (a) optimal medical therapy alone, (b) percutaneous coronary intervention, (c) coronary artery bypass graft or (d) more investigation required. Each group was then provided with fractional flow reserve (FFR) from all major vessels and asked to repeat the analysis.
Results There was only ‘fair’ level of agreement of management plan among ICs, NICs and CSs (kappa 0.351, 95% CI 0.295–0.408, p<0.001) based on ICA alone (complete agreement in 35% of cases), which almost doubled to ‘good’ level (kappa 0.635, 95% CI 0.572–0.697, p<0.001) when comprehensive FFR was available (complete agreement in 66% of cases). Overall, the consensus management plan changed in 36.7%, 52% and 37.3% of cases for ICs, NICs and CSs, respectively, when FFR data were available.
Conclusions Compared with ICA alone, the availability of systematic FFR of all major coronary arteries produced a significantly more concordant interpretation and more homogeneous management plan among IC, NIC and CS specialists. Comprehensive physiological assessment may be of value in routine care for Heart Team decision-making.
Trial registration number NCT01070771.
- fractional flow reserve
- percutaneous coronary intervention
- coronary angiography
- coronary artery disease
- coronary artery bypass
Data availability statement
Data are available upon reasonable request. The datasets generated and analysed during the current study are available from the corresponding author upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- fractional flow reserve
- percutaneous coronary intervention
- coronary angiography
- coronary artery disease
- coronary artery bypass
WHAT IS ALREADY KNOWN ON THIS TOPIC
Training of the various specialists in the Heart Team is different, which can influence their interpretation of invasive coronary angiography and their recommended management plan.
WHAT THIS STUDY ADDS
Systematic coronary physiology produced a significantly more concordant interpretation and more homogeneous management plan among Heart Team specialists.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Angiogram-derived physiology with every invasive angiogram is on the horizon. In addition to supporting homogenised patient management across the various cardiac specialties with the use of coronary physiology, this study provides a basis for a more uniform discussion at multidisciplinary team meetings.
Introduction
Interpretation of invasive coronary angiography (ICA) is a common part of the pathway for managing patients who present with chronic coronary syndromes (CCSs) and can be undertaken by interventional cardiologists (ICs), non-interventional cardiologists (NICs) and cardiac surgeons (CSs). All such specialists contribute to the Heart Team which, according to clinical practice guidelines,1 makes recommendations on the management of these patients in terms of optimal medical therapy alone (OMT), percutaneous coronary intervention (PCI), coronary artery bypass graft (CABG) or that more investigation is required (MIR). In the UK, targets within the curriculum for training for different subspecialties within cardiology, and in cardiac surgery, are substantially different.2 3 In practical terms, this means that cardiology and cardiac surgery trainees have different teaching exposure to the interpretation of coronary angiograms and this may lead to variable management strategies.
Investigation of patients with stable chest pain may involve an assessment of the presence of ischaemia, but increasingly this is not the case, given the direction of National Institute for Health and Care Excellence (NICE) CG95 guidelines to employ CT coronary angiography (CTCA) as the default test for most of these patients.4 Many of these patients will then be referred for ICA with a view to further management, despite there being a large body of evidence showing that the use of invasive physiological assessment is associated with substantial changes in diagnosis and management5 6 as well as improved patient outcomes.7 Despite clinical guidelines,8 9 adoption of pressure wires in clinical practice remains low.10 Specifically, ICs employ pressure wire assessment in less than 20% of their PCI cases.7 Further, NICs perform a significant number of coronary angiograms in the UK (40 000 out of 250 000 per year are performed in non-interventional centres),11 and as such do not have access to invasive physiology.
We postulated that the specialists that make up the Heart Team would have more discordant opinions regarding (a) the extent of significant coronary disease and (b) subsequent patient management when they had access to ICA data alone, compared with when they had systematic data regarding vessel-specific physiology as well.
The aim of this study, therefore, was to determine whether, in patients with stable chest pain who are being investigated with ICA, the availability of systematic fractional flow reserve (FFR) data would produce a more concordant interpretation of presence and distribution of significant coronary stenoses, and a more homogeneous management plan among ICs, NICs and CSs, than is seen using angiography alone.
Methods
Study doctors
A group of three specialists in interventional cardiology, non-interventional cardiology and cardiac surgery specialties took part. All contributing physicians were either on the Specialist Register (holding the Certificate of Completion of Training), or within 12 months of achieving this milestone. The NIC group comprised two electrophysiologists and one imaging specialist.
Angiogram cases
This study employed ICA and invasive FFR data from 150 cases from the RIPCORD Study, whose methodology has been previously described in detail.5 In brief, 200 patients with CCS underwent clinically determined ICA by their supervising NIC, who then recorded the severity of the coronary disease (according to visual estimate of per cent diameter stenosis) and made a management plan. A second cardiologist then measured FFR in all main coronary arteries or side branches if they had a calibre consistent with potential revascularisation. The FFR readings were then shown to the original, supervising NIC who was asked to repeat their assessment of vessel severity and management plan. In 32% of vessels, a decision about their significance changed when FFR was available, leading to a change in management in 26% of cases.5 We used 150 of these cases for the current study, choosing this number based on the time availability of the nine specialists to commit to this experiment.
Data collection
The study was conducted at University Hospital Southampton National Health Service Foundation Trust between January 2022 and March 2022. Each group of three specialists (IC, NIC, CS) was presented with the data independently from the other groups, in multiple sessions in order to accommodate the time the experiment required. For the purposes of the experiment, the physicians were provided with the following information: the patients were above 18 years of age, with no severe valvular heart disease, on guideline-directed medical therapy including two antianginal agents, were referred for elective coronary angiography to investigate stable chest pain and considered good candidates for any of the proposed management options described below. The presence/absence of diabetes mellitus was disclosed at beginning of each case.
In each case, the full ICA was presented using large screens and the three physicians in each group were asked to reach a consensus on the presence and extent of significant coronary stenosis(es). Similarly, a management plan consensus was recorded chosen from the options: (1) OMT alone, (2) PCI, (3) CABG or (4) MIR. Where revascularisation was chosen, the target vessels were also recorded. Furthermore, after these data had been recorded, each group was presented with the FFR data that had been measured in that same case, which included FFR for all vessels of a diameter suitable for revascularisation, and then asked again for a consensus using the same criteria on coronary significance and one of the management options. The primary endpoint for the study was the agreement on management between the three groups when considering ICA data alone and when ICA plus FFR data were available. Secondary endpoints were: (a) the difference within the three groups between their interpretation of the disease significance and management when comparing ICA data alone versus ICA plus FFR; and (b) levels of agreement between ICA and FFR interpretation within and between the groups.
Statistical analysis
All statistical analyses were performed using SPSS V.26 (IBM Corporation). Overall level of agreement on management plan among IC, NIC and CS was measured using Fleiss’ kappa, as well as the agreement level on each management option.12 Analysis of intergroup agreement was conducted using Cohen’s kappa. The following kappa values were used to describe each agreement level: <0.20 poor, 0.21–0.40 fair, 0.41–0.60 moderate, 0.61–0.80 good, 0.81–1.00 very good.13 14 The significance of per group changes before and after FFR was assessed using Stuart-Maxwell test.
Results
Baseline characteristics
Baseline characteristics for this population are shown in online supplemental table 1. The mean age was 63 years with the majority being male (74%). Hypertension and hyperlipidaemia were common (58% and 78%, respectively), while diabetes mellitus was present in 12%. The frequency of previous myocardial infarction was 18.7% and PCI was 18.7%.
Supplemental material
Angiographic assessment alone
The distribution of angiographically significant coronary disease (defined as chronic total occlusion or severe stenosis of more than 70% in any major coronary artery or its branches of ≥2.25 mm diameter) is presented in online supplemental table 2. IC specialists reported most of the cases as having single-vessel disease (46.7%), followed by two-vessel disease (26%), no significant disease (19.3%) and three-vessel disease (8%). On the other hand, NIC and CS described most of the cases as having single-vessel disease (47.3% and 46%, respectively), followed by no significant disease (29.3% and 26.7%, respectively), two-vessel disease (18.7% and 21.3%, respectively) and three-vessel disease (4.7% and 6%, respectively).
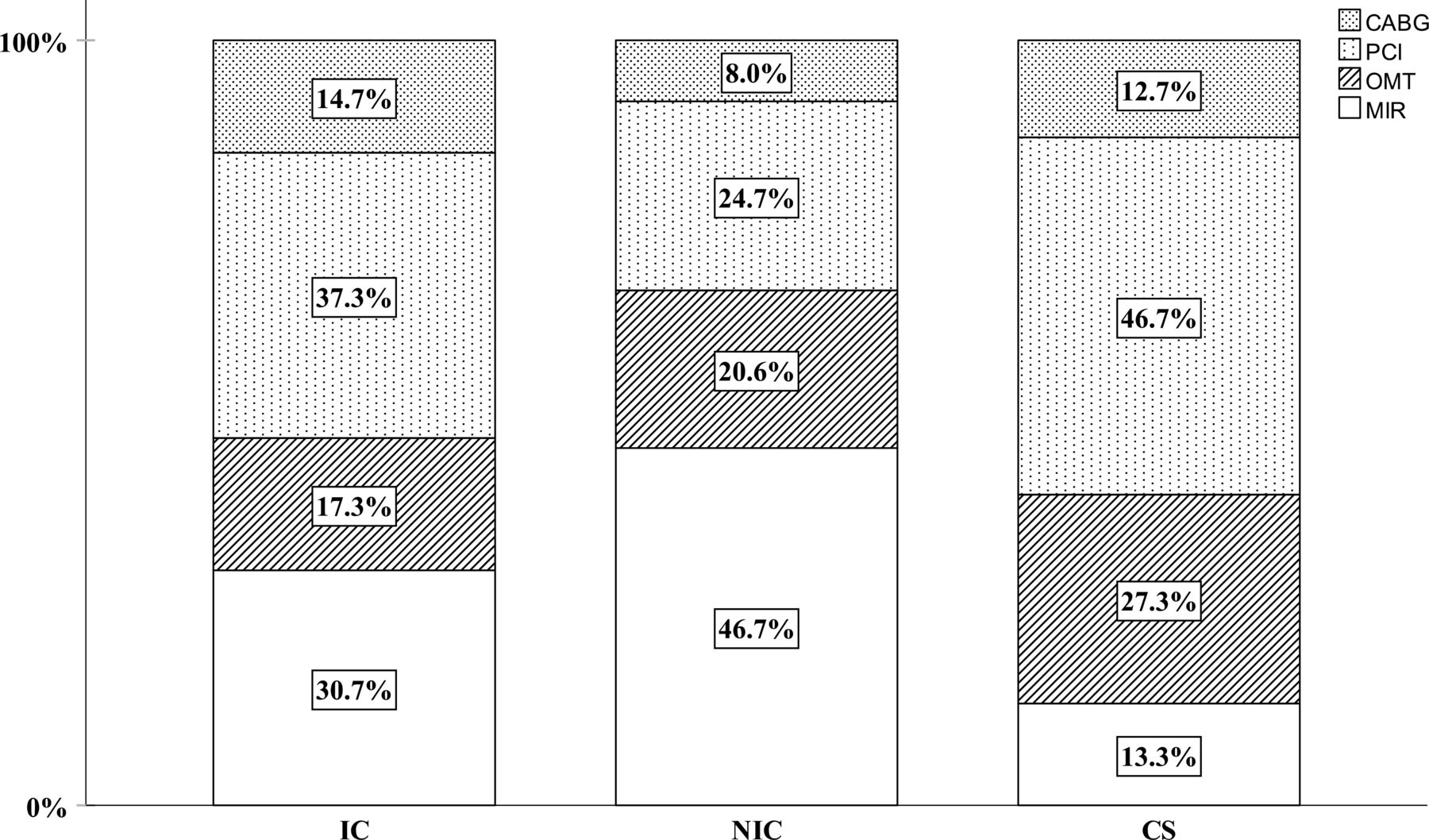
The management plans based on ICA data alone for IC, NIC and CS are illustrated in figure 1. Request for more investigation (MIR) was highest among the NIC (46.7%) followed by the IC (30.7%) and the CS (13.3%). A management choice of OMT was highest in the CS (27.3%), followed by NIC and IC (20.6% and 17.3%, respectively). PCI was chosen for 46.7% of patients by the CS group compared with 37.3% by IC and 24.7% by NIC. CABG was recommended in 14.7%, 12.7% and 8% of the cases by CS, IC and NIC, respectively.

The angiogram-based management plan distribution across the three cardiac specialties. CABG, coronary artery bypass graft; CS, cardiac surgeon; IC, interventional cardiologist; MIR, more investigation required; NIC, non-interventional cardiologist; OMT, optimal medical therapy; PCI, percutaneous coronary intervention.
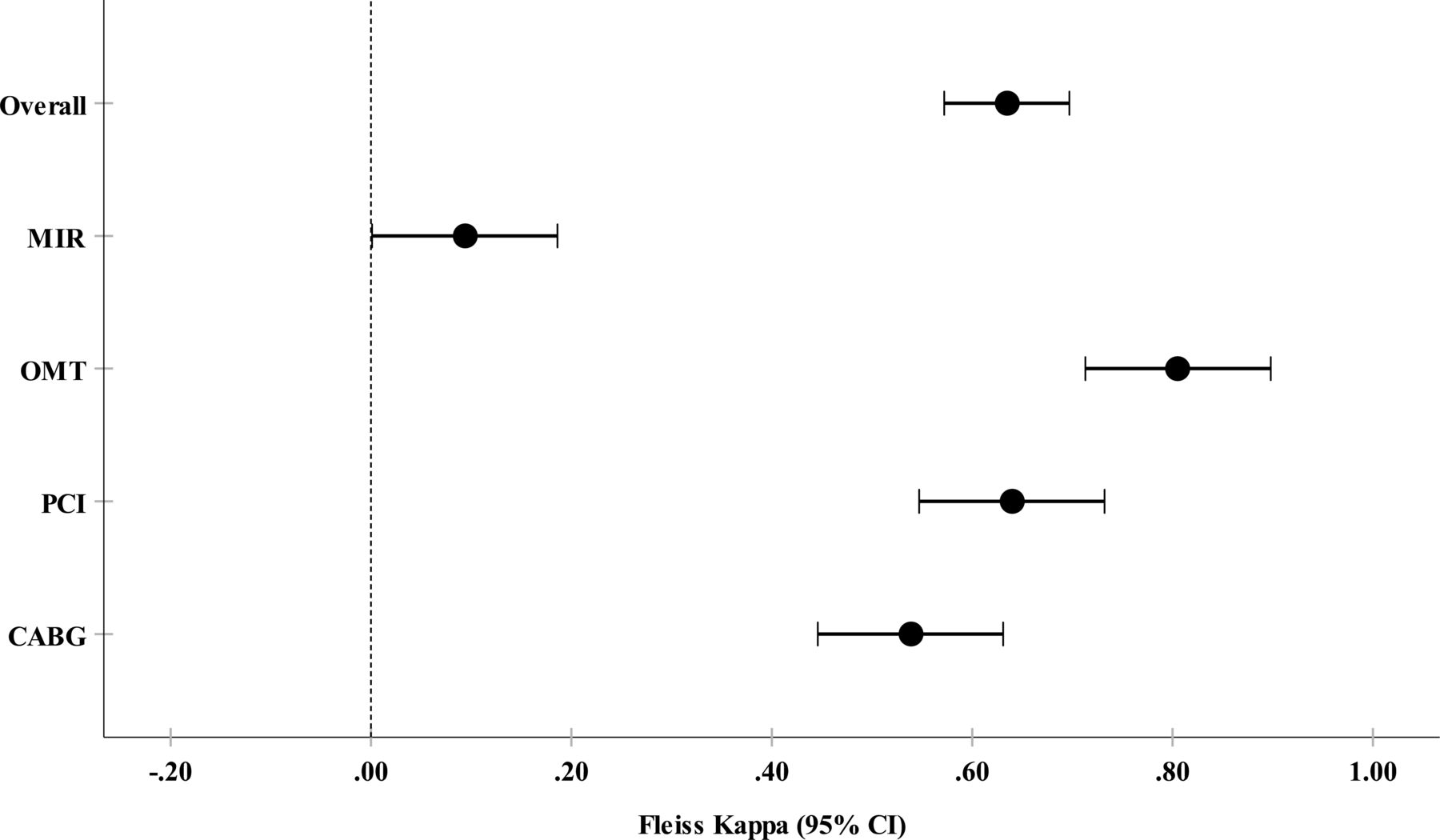
Total agreement on the management approach across all the three cardiac specialties was only observed in 35.3% of the cases (online supplemental table 3). The overall agreement level for the management plan based on the ICA data alone among IC, NIC and CS was fair (kappa 0.351, 95% CI 0.295–0.408, p<0.001) (figure 2). The level of agreement on each management plan option is presented in table 1.
The angiogram-based management agreement level among the three cardiac specialties

The angiogram-based management agreement level among the three cardiac specialties. CABG, coronary artery bypass graft; MIR, more investigation required; OMT, optimal medical therapy; PCI, percutaneous coronary intervention.
Angiography with FFR assessment of all vessels of a diameter suitable for revascularisation (ICA plus FFR)
The management choices for the three groups are shown in figure 3. Total agreement on the management plan between the three groups when FFR was available had almost doubled to 66% of the cases (online supplemental table 3). The overall agreement level on management plan using ICA plus FFR data among IC, NIC and CS improved to good (kappa 0.635, 95% CI 0.572–0.697, p<0.001) (figure 4). The agreement level on individual management plan option is shown in table 2.
The angiogram with FFR management agreement level among the three cardiac specialties

The angiogram with FFR management plan distribution across the three cardiac specialties. CABG, coronary artery bypass graft; CS, cardiac surgeon; FFR, fractional flow reserve; IC, interventional cardiologist; MIR, more investigation required; NIC, non-interventional cardiologist; OMT, optimal medical therapy; PCI, percutaneous coronary intervention.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
The angiogram with FFR management agreement level among the three cardiac specialties. CABG, coronary artery bypass graft; FFR, fractional flow reserve; MIR, more investigation required; OMT, optimal medical therapy; PCI, percutaneous coronary intervention.
Analysis of intergroup agreement
The overall level of agreement on the management plan between IC and NIC was moderate using ICA data alone, which improved to a good agreement after FFR (kappa 0.640, 95% CI 0.542–0.738; p<0.001). Level of agreement in management overall using ICA alone between IC and CS was fair but changed to good when FFR was available (kappa 0.626, 95% CI 0.530–0.722; p<0.001). NIC and CS had only fair level of agreement based on ICA alone but a good level of agreement with FFR (kappa 0.641, 95% CI 0.545–0.737; p<0.001) (table 3).
Analysis of intergroup agreement
Per specialty analysis
Interventional cardiology
The management plan allocation before and after FFR is summarised in online supplemental table 4 and online supplemental figure 1. The availability of FFR changed the management plan in 55 cases (36.7%) (p<0.001). These were mainly related to change from MIR plan to OMT and PCI (14.7% and 8% of all cases, respectively). In addition, the availability of FFR data negated the need for PCI in 12 cases (8%) in favour of OMT alone.
Non-interventional cardiology
The management plan allocation before and after FFR is summarised in online supplemental table 5 and online supplemental figure 2. The availability of FFR changed the management plan in 78 cases (52%) (p<0.001). These were mainly related to change from MIR plan to OMT, PCI and CABG (22%, 19.3%, 4.7% of all cases, in order). In addition, FFR negated the need for PCI in four cases (2.7%) in favour of continuing OMT.
Cardiac surgery
The management plan allocation before and after FFR is summarised in online supplemental table 6 and online supplemental figure 3. The management plan changed in 56 cases (37.3%) (p=0.053). Plan changes from PCI to OMT accounted for the majority (14 cases, 9.3%), followed by those from MIR to PCI and CABG (4.7% and 4% of all cases, respectively).
Correlation between angiographic and FFR vessel assessment
A total of 480 vessels had FFR measurements. Overall, a discrepancy was seen between the angiographic and FFR assessment of vessel significance in 20.4% of vessels on average across the three groups, using the definition of significance described above. There were two broad types of discrepancy: (a) type A—where the angiographic assessment was of significant stenosis, but the FFR was above 0.80; and (b) type B—angiographic assessment indicated that a lesion was not significant and the FFR was <0.80 (online supplemental figures 4 and 5). Overall, for all lesions, IC, NIC and CS had rates of type A discrepancy of 13.3%, 9.0% and 12.3%, and of type B in 6.9%, 9.2% and 10.4%, respectively.
Discussion
There are several key findings from this study. First, it has proven the hypothesis that in patients with CCS who are being investigated with ICA, the availability of systematic FFR data did produce a significantly more concordant interpretation and more homogeneous management among IC, NIC and CS. Second, the availability of systematic FFR changes the coronary significance assessment and management plan in all the specialties, and almost doubles the consensus level between them on how these patients should be managed. Third, that the angiographic and FFR assessment of vessel significance were discordant in 20.4% of vessels.
The doctors in this study are either on the Specialist Register or are within 12 months of achieving that target. The current study has confirmed that the angiographic assessment of patients with CCS is indeed different between these specialty groups and that this results in significant differences in the management plan suggested for patients. This observation is of concern, raising the possibility that the same patients may be managed differently according to the background training of the specialist. This reinforces the value of a Heart Team approach, in which such interspecialty differences may be incorporated into a multidisciplinary consensus.1 The high level of observed discordance between angiographic assessment and that after comprehensive vessel physiology is available would, however, not necessarily be overcome by the Heart Team approach.
The primary outcome from this study is that the availability of systematic FFR data from all coronary arteries of stentable/graftable diameter significantly improved the level of agreement in management plan across the three specialty groups when compared with ICA data alone. This is an important observation and has potential implications for routine clinical practice. Specifically, the result indicates that a more concordant level of assessment and management can be achieved if routine and systematic data about vessel-specific physiology are available on top of angiographic data alone. While it is unlikely, given the relatively low uptake of pressure wire use in everyday cardiology practice, that physicians will perform such comprehensive invasive assessment as a routine, these results do support the concept that comprehensive physiological data would be of value. Furthermore, these data have particular relevance given that systematic coronary artery physiology can be obtained both non-invasively, particularly using CTCA with FFRCT,15–17 and also using novel angiogram-derived physiology software, which is likely to become widely available in catheter laboratories in the near future.18 19 Our study suggests that there may be clinical benefit in the future in employing these tests on a routine basis in order to facilitate a more consistent assessment and management of patients with CCS.
The outcome in this study must be analysed in the context of contemporary literature. First, in the recent RIPCORD2 randomised trial, 1100 patients with either CCS or non-ST-elevation myocardial infarction were randomised to assessment and treatment based on ICA alone or ICA plus invasive FFR measurement in all vessels of a diameter suitable for revascularisation.20 RIPCORD2 failed to show any difference in overall resource utilisation, quality of life or clinical events between the two groups. In that trial, however, all the supervising physicians were ICs and no interspecialty differences would have had relevance, in contrast to the current study. Second, current NICE Clinical Guidance CG95 recommends that the vast majority of patients with recent-onset chest pain should undergo CTCA as their default first test.4 Although the supervising cardiologist (who might be IC or NIC) normally receives a report of the CTCA result derived from a trained independent radiologist or cardiologist, their interpretation of such data, and the interpretation of CS, may be modified by their specialty-specific training. The results of the current study lend some support to the concept that management may be most consistent if FFRCT data were to be available in such cases. Balanced against this, the FORECAST trial, which randomised patients with new-onset stable chest pain to CTCA with FFRCT versus routine testing, did not show any difference in resource utilisation or clinical outcome.21
The current results also add weight to the potential appeal of having real-time angiography-derived coronary physiology, which thereby would provide a comprehensive assessment of coronary physiology at the time of ICA, as a routine adjunct, although this hypothesis requires further assessment.
This study has a number of limitations. First, that the number of cases included is relatively small. Second, that the cases were from a previous study and that the decision-making was based on the same hypothetical clinical scenario in each case. Third, there was no assessment of reproducibility of the interpretation of the presented data. Finally, the choice of doctors in each group was based on local availability, and there is no way of assessing the degree to which they represent typical opinions of their subspecialty.
In conclusion, the availability of comprehensive FFR data substantially changes interpretation of coronary significance and management in all three specialist groups, and thereby significantly improves the level of agreement between IC, NIC and CS with regard to the management of CCS when compared with ICA alone. These results suggest that comprehensive physiological data may improve treatment consistency between specialties, if available routinely in the future, for example, using angiography-derived coronary physiology.
Data availability statement
Data are available upon reasonable request. The datasets generated and analysed during the current study are available from the corresponding author upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The ethical approval of this study was included in the original RIPCORD Study.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Original concept, design, analysis, drafting manuscript and overall responsibility for all data/guarantor- NC. Design, data collection, analysis, drafting manuscript- BH. Data collection and checking manuscript AS, OA, DG, JH, DK, GK, SO, EO, MP, AZ, ZN, PG. Analysis, editing manuscript JE, ZA.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests JE reports receiving consulting fees and lecture fees from Abbott, Philips and Boston Scientific, and lecture fees from Abiomed, Terumo, Medtronic and Biosensors. ZA reports institutional research grants to St Francis Hospital from Abbott, Philips, Boston Scientific, Abiomed, Acist Medical, Medtronic and Cardiovascular Systems; being a consultant to Amgen, AstraZeneca and Philips; and having equity in Shockwave Medical. NC reports unrestricted grants from Boston Scientific, HeartFlow, Haemonetics and Beckmann Coulter; speaker fees from Abbott, Boston and Edwards; and travel sponsorship from Abbott, Biosensors, Medtronic and Shockwave. All other authors declare no conflict of interest.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.