Article Text

Abstract
Introduction Interventional closure of the left atrial appendage (LAAC) has been established as an alternative treatment for patients with atrial fibrillation (AF) and an elevated risk of stroke. The WATCHMAN FLX (WM FLX) as the newest WATCHMAN LAAC device differs in several technical characteristics from its precursor, the WATCHMAN V.2.5 (WM V.2.5).
Methods The data presented here are derived from a retrospective single-centre study. All patients in which an LAAC was performed between February 2017 and March 2021 with either a WM V.2.5 or WM FLX device were included.
Results 169 patients were included in this study, of whom 95 had been treated with WM V.2.5 and 74 with WM FLX, respectively. Directly after implantation, only minor differences regarding membrane thickness and connector protrusion were noted, whereas no relevant differences were found regarding device sizing, device compression or peridevice leakage, respectively. However, at 3-month follow-up, device compression was significantly reduced in WM FLX indicating a continued device expansion which was paralleled by a reduced number of peridevice leakage in comparison to WM V.2.5. Additionally, the combined clinical endpoint of death, stroke/transistoric ischaemic attack, tamponade, device embolisation, device-related thrombosis or peridevice leakage was reduced in WM FLX.
Conclusion LAAC using the WM FLX device results in a continued device expansion over the first 3 months based on differences in radial force in comparison to WM V.2.5. This is accompanied by a reduction in adverse clinical endpoints.
- atrial fibrillation
- echocardiography
- stroke
Data availability statement
Data are available upon reasonable request. Data can be obtained from the authors on justified request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Closure of the left atrial appendage using the WATCHMAN device is an established treatment option for patients with atrial fibrillation who have an increased risk of stroke.
WHAT THIS STUDY ADDS
Within the last years, a transition from WATCHMAN V.2.5 to WATCHMAN FLX (WM FLX) has taken place. We report differences in the echocardiographic appearance as well as parameters linked to peridevice leakage.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Proper implantation of the WM FLX results in a continued device expansion over the first 3 months, which might improve patient outcomes.
Introduction
In patients with atrial fibrillation (AF) who had a stroke, at least 90% of underlying thrombi are originating from the left atrial appendage (LAA).1 2 Therefore, interventional closure of the left atrial appendage (LAAC) has been established as an alternative treatment within the last years—especially if contraindications regarding the use of oral anticoagulation (OAC) are existing.3 Nowadays, several manufacturers are offering various devices for LAAC (for review see Cruz-Gonzalez et al4), as the anatomy of appendages varies in shape, size and lobar structure. Among them, the WATCHMAN device is one of the most studied devices so far. WATCHMAN FLX (WM FLX) as the newest WATCHMAN LAAC device has been available within the EU since 2015, redesigned in 2019, and in the USA since 2020, respectively. The WM FLX differs in several technical characteristics from its precursor, the WATCHMAN V.2.5 (WM V.2.5), which is paralleled by changes in the handling instructions during the implantation procedure.5
Meanwhile, a number of clinical studies have shown the clinical performance of the WM FLX in patients with AF,5 6 indicating a further improvement of clinical endpoints in comparison to its precursor version. However, detailed information especially regarding differences in echocardiographic findings during follow-up examinations between the two devices are scarce so far.
Methods
The data presented here are derived from a retrospective single-centre study performed at the Catholic Hospital ‘St. Johann Nepomuk’, Erfurt, Germany. All patients in which an LAAC was performed between February 2017 and March 2021 were retrospectively identified from the hospitals’ database. Patients were included into the study if LAAC was performed with either a WM V.2.5 or WM FLX device and procedural and clinical data as well as transesophageal echocardiography (TEE) recordings were available. Pseudonymised data regarding demographics, medical history, implantation procedure and clinical outcomes were entered into the study database. All available echocardiographic recordings from the implantation procedure after release of the device as well as from 3-month follow-up were viewed and analysed by the study team and also entered into the database. The following TEE parameters (2D) were determined at 0°, 45°, 90° and 135°: device protrusion towards LA, device size (compression), device membrane thickness, device connector protrusion and peridevice leakage (PDL), respectively. From the measured device size (compression), the parameter ‘relative compression’ was calculated as relative compression (%)=(nominal device size–measured device size)/nominal device size)×100. Additionally, the occurrence of device-related thrombus (DRE) was recorded.
Statistical analysis
Statistical data analysis was performed using SPSS Statistics (V.26). Differences in frequency of nominally scaled parameters were compared by means of Pearson’s χ2 test. Metric variables are expressed as mean±SD and were compared with Student’s t-test. A binary logistic regression was performed to analyse the combined clinical endpoint of death, stroke/transistoric ischaemic attack (TIA), tamponade, device embolisation, DRE or peridevice leakage.
Results
Baseline data and LAAC procedure
A total of 169 patients were included in this study, of whom 95 had been treated with WM V.2.5 and 74 with WM FLX, respectively (table 1). Data regarding the LAAC implantation procedures are given in table 2. The frequency of the different device sizes are shown in table 3. As seen from the tables, no significant differences can be found between the two groups in any of these parameters.
Demographic data at baseline
Left atrial appendage closure implantation procedure
Frequency of usage of the different device sizes
Echocardiographic assessment
Quantitative transoesophageal echocardiographic evaluation of the implantation result was done directly at the end of the implantation procedure after the release of the device as well as after 3 months, respectively. The corresponding findings are given in table 4. At the time of implantation, no relevant differences regarding device positioning or degree of compression could be noticed. However, the echocardiographic appearance of the covering membrane as well as the protrusion of the connector are slightly different between the two devices.
Quantitative transoesophageal echocardiographic assessment
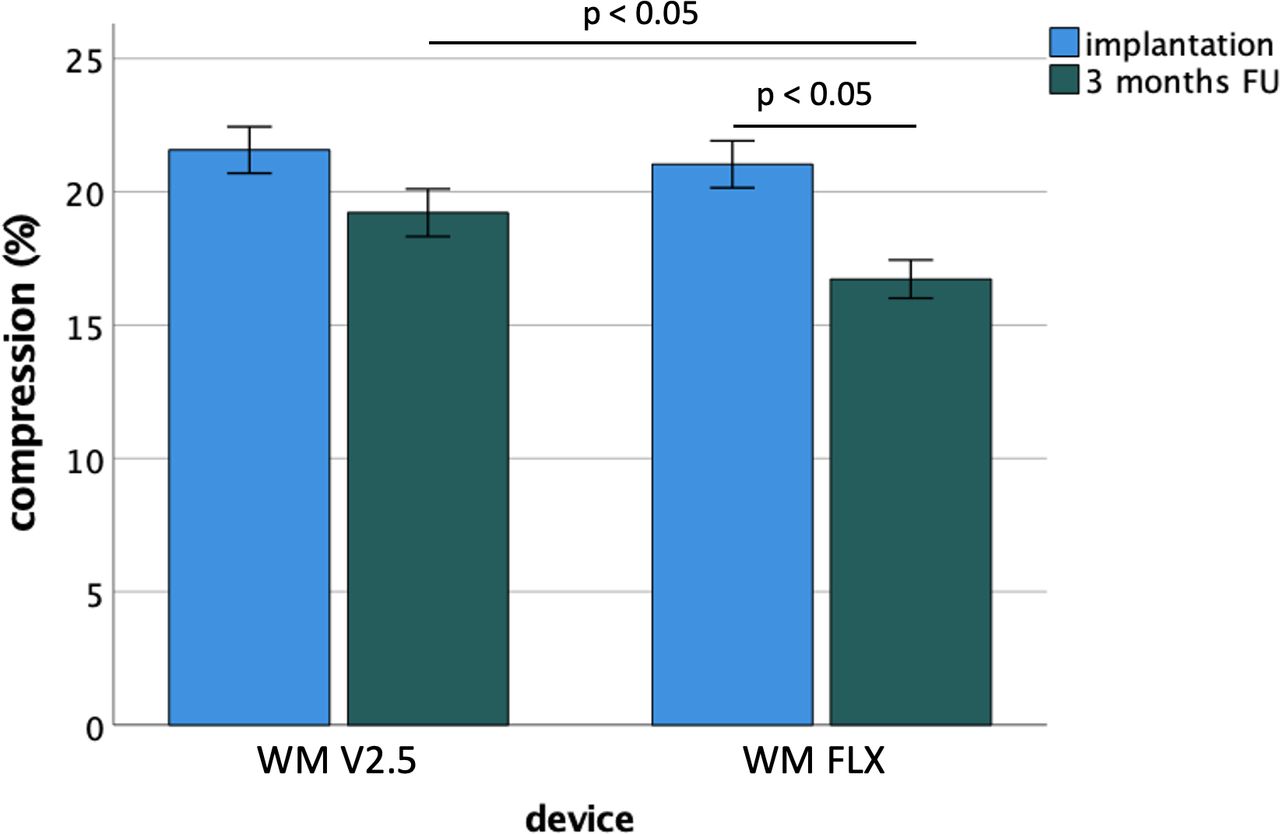
After 3 months, the degree of compression was numerically reduced in both devices indicating a delayed expansion of the LAA implants. Interestingly, this reduction of device compression was significantly more pronounced in the WM FLX devices (figure 1).

Relative device compression (%) in transoesophageal echocardiography directly after the implantation procedure and after 3 months, respectively. FU, follow-up; WM V.2.5, WATCHMAN V.2.5; WM FLX, WATCHMAN FLX.
Information regarding the occurrence of PDL is given in tables 5 and 6. At the time of implantation, there was no relevant difference between the two occluder types in this regard with only one patient presenting with a small PDL in each of the groups. At 3-month follow-up, the number of patients with signs of PDL in TEE was increased in both groups. As seen in table 6 in the group of patients treated with the WM V.2.5, both the total number of patients with any proven PDL (20% vs 9.6%) and leakage severity were higher than in the WM FLX group.
Quantitative echocardiographic assessment of peridevice leakage
Quantitative echocardiographic assessment of peridevice leakage at 3-month follow-up (p=0.11)
From a pathophysiological perspective, it seemed reasonable to assume that there might be a link between relative device compression after implantation and the occurrence of peridevice leakage at 3-month follow-up. Therefore, we analysed the connection of device compression and PDL occurrence in a receiver operator analysis (ROC). It turned out that especially minimal relative device compression (rather than mean or maximum of compression) was associated with the occurrence of PDL (area under the curve (AUC): 0.67; p=0.027). When analysing the influence of the size of the LAA orifice as determined by TEE on the occurrence of PDL, no significant effect was observed. Despite this, the size of the implanted LAA occluder (as a surrogate of the size of the LAA ostium) was significantly linked to the occurrence of PDL at 3 months in ROC analysis (AUC: 0.67; p=0.014). However, when the two variables were combined in a model of logistic regression, only minimal relative device compression but not LAA occluder size remained significantly associated with PDL (Exp(B)=0.87; p=0.03).
Clinical endpoints
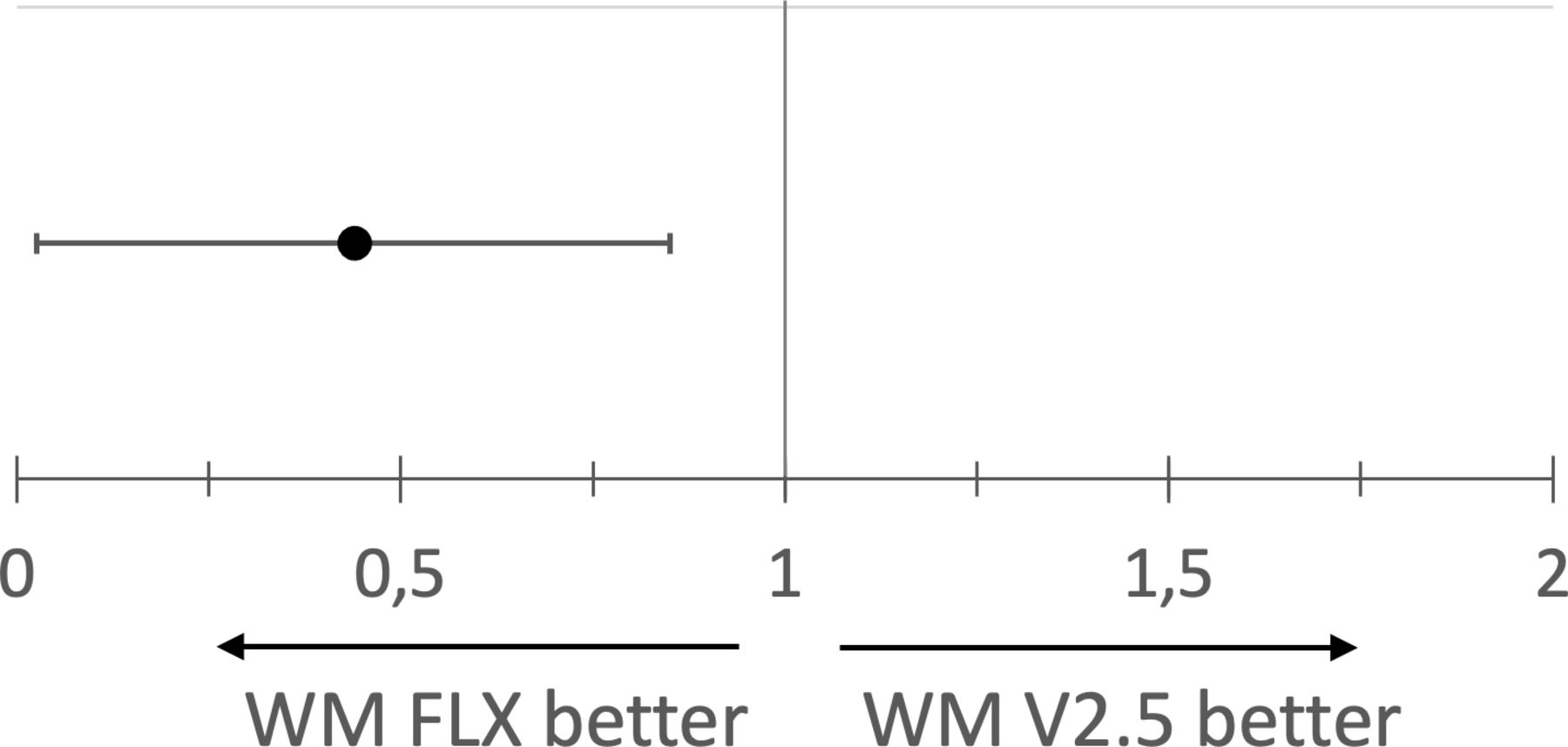
Between the LAAC implantation procedure and the 3-month follow-up, a number of clinical endpoints could be observed (table 7). Due to the limited number of events, no significant difference between the groups could be found for any of the individual endpoints. However, the combined clinical endpoint consisting of death, stroke/TIA, systemic embolism, pericardial tamponade, DRE or peridevice leakage was less frequently found in the WM FLX group of patients. In a binary logistic regression model, the risk of reaching this combined endpoint was reduced in the WM FLX group by 59% (figure 2).
{kind=link}
{kind=link}
Comparison of the two occluder types on the occurrence of the combined clinical endpoint of death, stroke/transistoric ischaemic attack/systemic embolism, pericardial tamponade, device-related thrombosis or paradevice leakage at 3-month follow-up (binary logistic regression, Exp(B)). WM V.2.5, WATCHMAN V.2.5; WM FLX, WATCHMAN FLX.
Clinical end points at 3-month follow-up
Discussion
AF is the most common cardiac arrhythmia in advanced age and is associated with the risk of intracardiac thrombus formation and the occurrence of stroke. OAC is still the standard therapy for patients with AF who have an increased risk of stroke.3 However, a number of patients with AF develop bleeding complications that require discontinuation of OAC. In this situation, interventional closure of the LAA represents an established treatment alternative.7
Since the early days of LAAC, a number of improvements have been implemented into new devices and interventional strategies so that the procedure of LAAC has become both more effective and safer.5 8 One of the most recent developments was the introduction of the WM FLX device, which has received Food and Drug Administration (FDA) approval in 2020. Data from the Protection Against Embolism for Nonvalvular AF Patients: Investigational Device Evaluation of the Watchman FLX LAA Closure Technology (PINNACLE) trial reported positive clinical data regarding the efficacy and safety of the new device.5
The aim of our study presented here was to describe which changes in procedural data as well as during echocardiographic follow-up can be observed when an implanting centre switches from using the WM V.2.5 to the WM FLX.
Although there are several differences in the implantation procedure between the two occluder types,5 this obviously does not translate into relevant changes in procedure time, use of contrast medium or radiation dose, respectively, which all were comparably between the two groups and within the range of previous reports.9 In parallel, positioning of the two devices directly after implantation was found to be very similar in TEE without any signs of systematic differences. This also applies for the depth of implantation, which is of prognostic importance with WATCHMAN devices in order to avoid an uncovered LAA neck, which otherwise might harbour a risk of embolic events. However, two details of the appearance of the WM FLX differ from its precursor, the covering membrane has a thicker echocardiographic appearance and the connector seems to be more protruding in respect to the front surface of the device. During 3-month follow-up, these two echocardiographic differences were found less pronounced.
Regarding clinical end points, the use of the WM FLX was associated with favourable outcomes in our study as the occurrence of the combined endpoint of death, stroke/TIA/systemic embolism, tamponade, device embolisation and peridevice leakage was reduced by 59% in comparison to WM V.2.5. In line with this, previous reports also described a numerically lower number of peridevice leakage in favour of WM FLX.10 11
Although especially for the WATCHMAN device, small leaks have been considered of no clinical relevance initially,12 there has been a large retrospective study recently which has found a modestly higher incidence of thromboembolic events in patients after LAAC with residual leaks <5 mm.13
So far, only limited data is available regarding risk factors that predict the occurrence of PDL after percutaneous LAAC.14–16 Previous studies were describing LAA size15 or eccentricity of the LAA14 as a major determinant in the development of PDL, which, however, are variables that cannot be influenced by the LAAC procedure itself. In contrast, our data indicates that minimal device compression at the time of implantation seems to be of special importance as this parameter was significantly linked to leaks at 3-month follow-up in a multivariate regression model whereas LAA size was not, a finding that had been described in a similar way before.16 Additionally, the data shows that after 3 months there were less PDL in the WM FLX group where we consistently found evidence of a more pronounced delayed device expansion as a potential explanation. Taken together, these findings argue for the importance of the radial force of the LAA occluder towards the surrounding tissue as an important factor to avoid the development of PDL.
Limitations
Our study consists only of 169 LAAC cases which limits the statistical strength especially regarding clinical outcomes. Additionally, TEE was not available in all patients at both time points in part caused by the ongoing COVID-19 pandemic. According to the study protocol, only procedures with the WATCHMAN were included into the trial so that no comparison between different LAAC devices can be given.
Data availability statement
Data are available upon reasonable request. Data can be obtained from the authors on justified request.
Ethics statements
Patient consent for publication
Footnotes
Contributors All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by CS, HE, AS, MH and PR. The first draft of the manuscript was written by CS and HE and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript. HE is acting as guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests HE has received consulting fees/honoraria for lectures from Pfizer, Boehringer Ingelheim and Boston Scientific. HE has received research grants from Boston Scientific and Siemens Healthcare.
Provenance and peer review Not commissioned; externally peer reviewed.