Article Text

Abstract
Background Structural changes caused by spinal curvature may impact the organs within the thoracic cage, including the heart. Cardiac abnormalities in patients with idiopathic scoliosis are often studied post-corrective surgery or secondary to diseases. To investigate cardiac structure, function and outcomes in participants with scoliosis, phenotype and imaging data of the UK Biobank (UKB) adult population cohort were analysed.
Methods Hospital episode statistics of 502 324 adults were analysed to identify participants with scoliosis. Summary 2D cardiac phenotypes from 39 559 cardiac MRI (CMR) scans were analysed alongside a 3D surface-to-surface (S2S) analysis.
Results A total of 4095 (0.8%, 1 in 120) UKB participants were identified to have all-cause scoliosis. These participants had an increased lifetime risk of major adverse cardiovascular events (MACEs) (HR=1.45, p<0.001), driven by heart failure (HR=1.58, p<0.001) and atrial fibrillation (HR=1.54, p<0.001). Increased radial and decreased longitudinal peak diastolic strain rates were identified in participants with scoliosis (+0.29, Padj <0.05; −0.25, Padj <0.05; respectively). Cardiac compression of the top and bottom of the heart and decompression of the sides was observed through S2S analysis. Additionally, associations between scoliosis and older age, female sex, heart failure, valve disease, hypercholesterolemia, hypertension and decreased enrolment for CMR were identified.
Conclusion The spinal curvature observed in participants with scoliosis alters the movement of the heart. The association with increased MACE may have clinical implications for whether to undertake surgical correction. This work identifies, in an adult population, evidence for altered cardiac function and an increased lifetime risk of MACE in participants with scoliosis.
- Magnetic Resonance Imaging
- Heart Failure
- Risk Factors
Data availability statement
UK Biobank (https://www.ukbiobank.ac.uk/) population reference datasets are publicly available. Analysis code is available on GitHub (https://github.com/ImperialCardioGenetics/Scoliosis).
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
What is already known on this topic
The majority of cardiac studies in patients with scoliosis surround investigations into congenital heart disease. Currently, studies are lacking on the impact of age-related and acquired scoliosis on the functioning of a developmentally normal heart.
What this study adds
This study is the first to investigate an interplay between scoliosis and cardiac manifestations in adults of the UK Biobank. We identified an increased lifetime risk of major adverse cardiovascular events, driven by heart failure and atrial fibrillation, and altered radial and longitudinal peak diastolic strain rates in participants with scoliosis.
How this study might affect research, practice or policy
Scoliosis may be an important modifier of cardiac strain and lifetime risk of major adverse cardiovascular event in the adult population. This has clinical implications for the consideration of undertaking scoliosis treatment surgery to alleviate the cardiac burden.
Introduction
Scoliosis is the lateral curvature of the spine with a Cobb angle >10°, primarily diagnosed in adolescents.1 There are multiple aetiologies of scoliosis including neuromuscular, congenital, syndromic or secondary to other diseases such as muscular dystrophy or Friedreich’s ataxia.2 However, the most common type is idiopathic scoliosis, with a prevalence of 8% in adults aged over 40 years old.3–5 In later life, scoliosis can result from skeletal muscle diseases such as sarcopenia. Sarcopenia is the loss of muscle mass associated with age that may cause imbalance and alteration on the supportive muscles of the spine, contributing to the progression of degenerative scoliosis in elderly patients.6 7 Degenerative scoliosis is observed in 68% of adults aged over 60 years old, as the joints and disks of the spine begin to deteriorate.7 Osteopenia, loss of bone density, is more frequently observed in women and contributes to the severity of the curvature of the spine.8 Furthermore, the coexistence of congenital heart disease (CHD) and spinal curvature is found in up to 12% of infant and juvenile patients with scoliosis presenting with CHD.9 10 This is likely due to shared developmental aetiology, whereas studies are lacking on the impact of age-related scoliosis on the functioning of a developmentally normal heart.
In addition to impacting physical day-to-day activities, structural disruption of the thoracic cage (pectus deformity) can influence the organs within, such as the heart.11 Pectus deformities lead to the displacement of the heart towards the left side of the body which can result in right-sided spinal curvatures as the beating heart pushes the thoracic vertebrae to the right.7 11 Furthermore, the degree of curvature of the spine can greatly increase the risk of restrictive lung disease, which in conjunction with intrathoracic organ displacement, increases the risk of comorbidities with high mortality rates, such as right heart failure.3 12
The impact of scoliosis on adult cardiac function has not been extensively studied and the relationship between scoliosis and non-congenital cardiac manifestations is not well characterised. In the UK Biobank (UKB) adult population cohort, we explored whether all-cause scoliosis has an impact on or relationship with cardiac phenotypes of the matured adult heart. We identify altered radial and longitudinal peak diastolic strain rates and an increased lifetime risk of major adverse cardiovascular events (MACEs) in participants with scoliosis in the UKB. In addition, we observed associations between scoliosis and older age, female sex, heart failure, valve disease, hypercholesterolemia, diagnosis of hypertension and decreased enrolment for cardiac MRI (CMR).
Methods
The UKB population cohort
The UKB recruited over 500 000 participants aged 40–69 years across the UK between 2006 and 2010 (National Research Ethics Service, 11/NW/0382, 21/NW/0157).13 This project was conducted under the UKB applications 47602 and 40616. All participants provided written informed consent.14
UKB codes for identification of scoliosis
A diagnosis of scoliosis was identified for UKB participants through the first occurrence of scoliosis trait (M41*), a composite trait of the first reported date derived by the UKB that incorporates data from primary care, hospital inpatient admissions, death records and self-reported medical conditions (table 1).
Codes used for identification of all-cause scoliosis
CMR data
Among all UKB participants, 39 559 participants had CMR data available.15 Imaging was performed using a 1.5 Tesla machine (MAGNETOM Aera, Siemens Healthcare, Erlangen, Germany),15 and 2D summary CMR traits were analysed for an association with scoliosis. This includes left ventricular ejection fraction, left ventricular end systolic volume, left ventricular end diastolic volume and measures of cardiac strain: Eulerian radial strain, Eulerian longitudinal strain, Eulerian circumferential strain, radial peak diastolic strain rate (PDSRrr) and longitudinal peak diastolic strain rate (PDSRll). All CMR traits were adjusted for age at the time of imaging, sex, white British ancestry, systolic blood pressure (SBP) and body surface area (BSA).
Surface to surface analysis
A mass univariate regression was used to explore associations between the three-dimensional (3D) mesh-derived phenotype and scoliosis.16–19 The underlying principle of this approach is the implementation of a linear regression at each vertex of the 3D atlas to derive a regression coefficient associated with the variable of interest, which results in a map of beta-coefficients showing the strength and direction of these associations. The analysis was adjusted for age at the time of imaging, sex, white British ancestry, BSA, diastolic blood pressure (DBP) and SBP.
Lifetime risk and survival analyses
Lifetime risk of disease, from birth month to January 2021, was assessed using the first occurrence of scoliosis trait (M41*). The first occurrence of health outcomes summary data in the UKB is reported using ICD10 codes.13 The fields analysed for the MACEs composite trait were as follows: cardiac arrest, I46*; atrial fibrillation and flutter/arrhythmia, I48* and I49*; heart failure, I50* and stroke, I64*, as previously published.20 The survival analysis was conducted using MACE and death as the primary outcome. Survival and survminer R packages were used to estimate HRs.
Statistical analysis
R programming language (V.3.6.0) and RStudio software (V.1.3.1073) were used for analyses. Categorical variables were assessed using χ2 test or Fisher’s exact test and expressed as percentages. Continuous variables were assessed using Student’s t-test and expressed as mean±SD. All p values were adjusted using Bonferroni correction for multiple comparisons where Padj <0.05 was deemed significant.
In the association of disease analysis, all variables were adjusted for age at recruitment (UKB ID: 21022-0.0) and genetic data-derived sex (UKB ID: 22001-0.0) using a multiple linear regression model. A separate multiple linear regression model for CMR traits was used to adjust for covariates at the time of imaging: age, sex, white British ancestry, SBP and BSA.
Results
Prevalence of scoliosis in the UKB
The prevalence of all-cause scoliosis in 502 324 participants of the UKB was 1 in 120 (n=4095; 0.8%). Of the 4095 participants with scoliosis, 1489 (37%) were diagnosed with scoliosis prior to recruitment. Of the total participants with scoliosis, 10 (0.2%) reported congenital scoliosis, 23 (0.6%) reported childhood scoliosis (infantile and juvenile) and the rest reported scoliosis due to other causes later in life. The most common scoliosis subtype was unspecified scoliosis reported by 2685 (65.6%) participants (table 1).
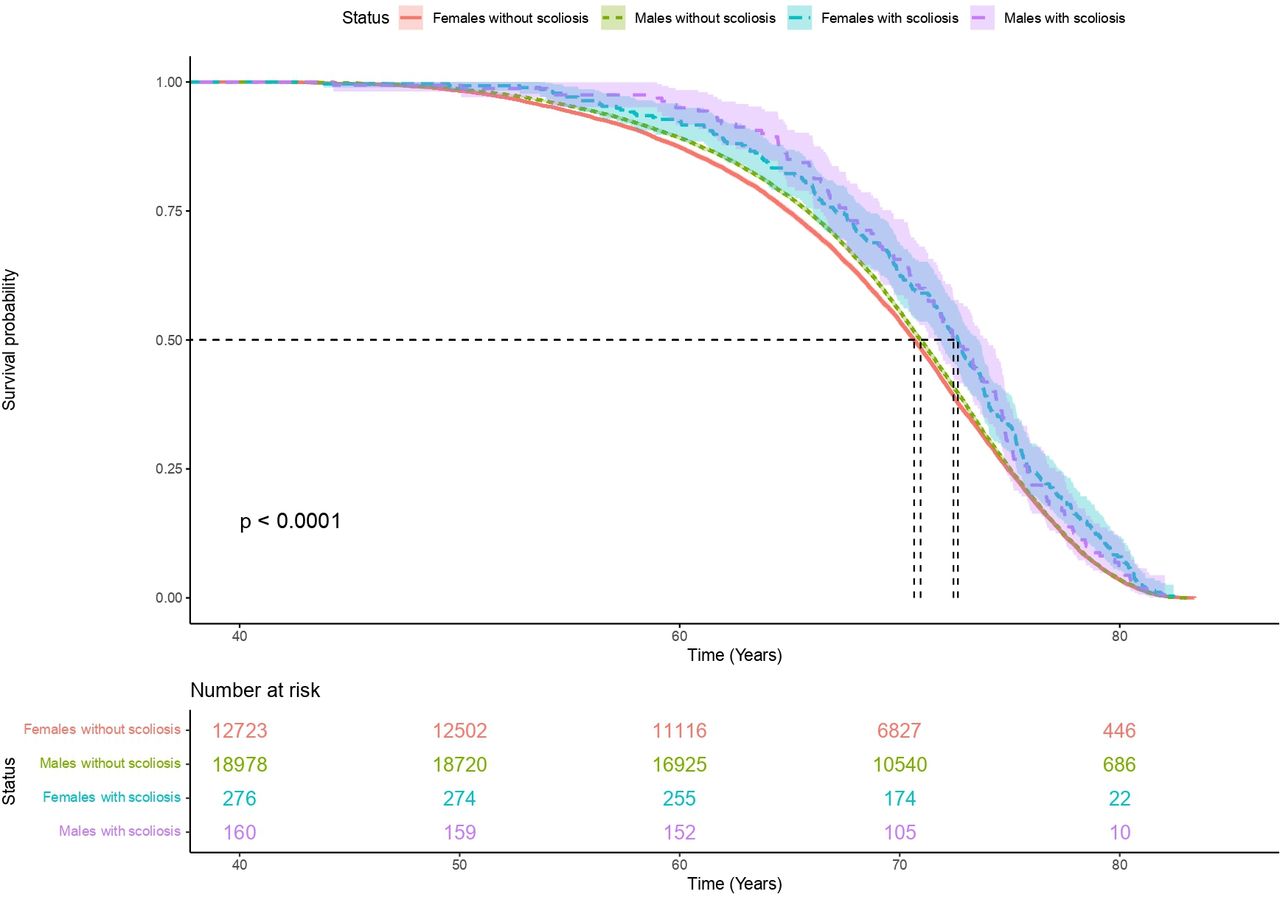
Participants with scoliosis were significantly older than the rest of the population (59.4 years old±7.58; mean age 56.5 years old±8.10; Padj <0.01) and were more female (69% women in scoliosis cohort; 55% women in the rest of the UKB population; Padj <0.01). Lifetime risk analysis showed that participants with scoliosis had significantly longer lives when compared with the rest of the population, regardless of sex (figure 1).
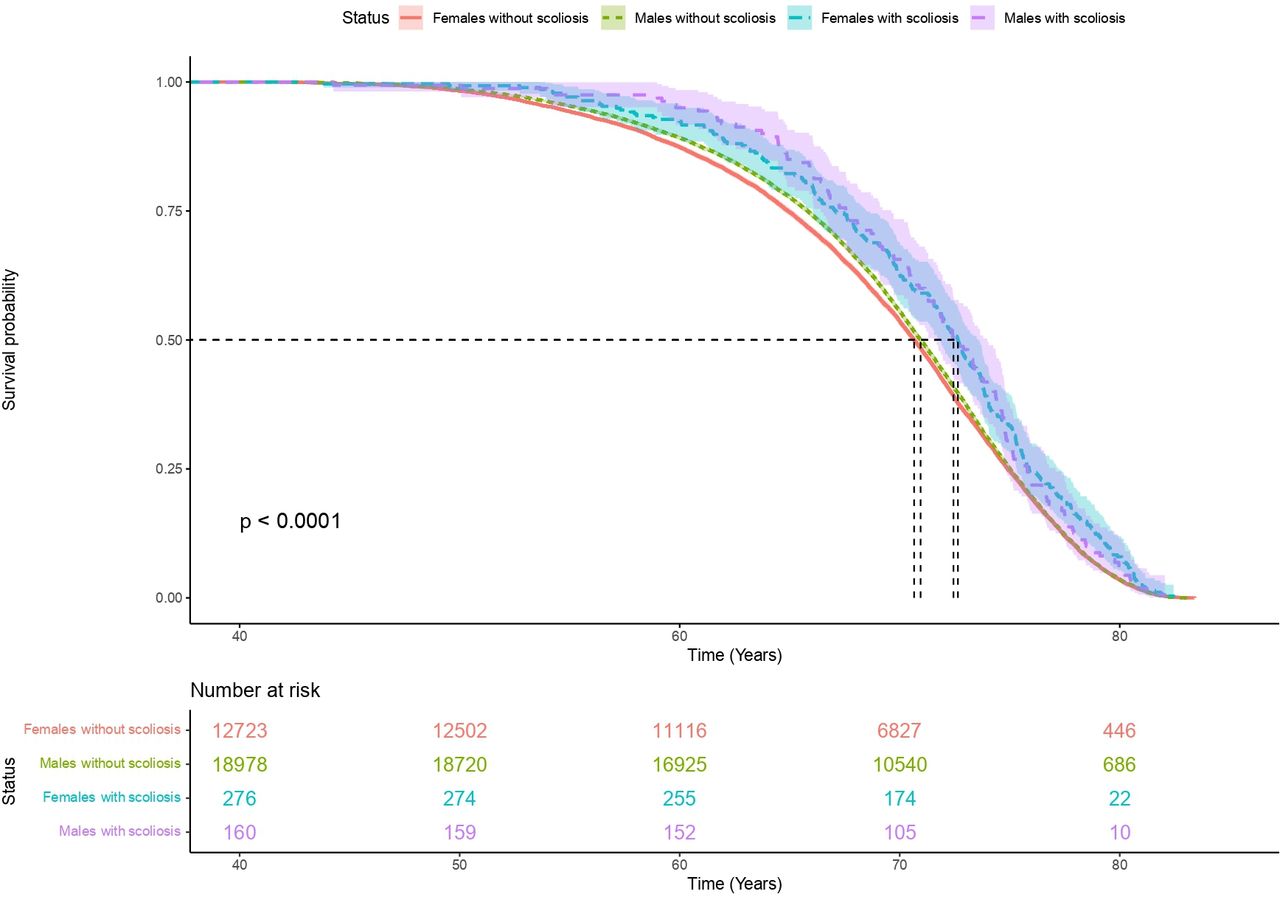
Scoliosis is associated with longer life compared with the rest of the UKB cohort, adjusted for sex. Years of life is shown on the x-axis from date of birth. Counts of UKB participants are shown in the box depicting number at risk. The median survival time (a survival probability of 0.5) was significantly increased in participants with scoliosis, regardless of sex. Median survival time for females with scoliosis versus females without scoliosis (2 years difference); median survival time for males with scoliosis versus males without scoliosis (1.5 years difference). UKB, UK Biobank.
We observed a significantly increased burden of heart failure (+4%, Padj <0.001), valve disease (+1%, Padj <0.001), hypercholesterolemia (+7%, Padj <0.001) and diagnosis of hypertension (+13%, Padj <0.001) in participants with scoliosis, adjusted for age and sex (table 2). Although diagnosis of hypertension was significantly increased, no significant differences were found with SBP or DBP, which may be due to the correction of diagnosed hypertension through medication. Additionally, the proportion of participants with scoliosis and CMR available was significantly decreased (−3%, Padj <0.001) compared with the rest of the population.
Summary statistics of participants with scoliosis compared with the rest of the UK Biobank population cohort
CMR analysis of participants with scoliosis identifies altered cardiac diastolic strain
2D summary CMR traits were available for 39 559 participants.15 Two hundred and twenty-four participants with scoliosis and CMR available had significantly increased radial PDSR (Padj <0.05) and decreased longitudinal PDSR (Padj <0.05) compared to participants without a diagnosis of scoliosis (table 3). Adequate diastolic function is essential during ventricular filling and maintenance of optimum stroke volume. PDSR is a diastolic function trait, that has been previously associated with MACEs, increased mortality, increased blood pressure, and altered left atrial function.21 For example, decreased PDSRrr corresponds to stiffer ventricle, impairing relaxation and increasing the risk of heart failure.21 No additional significant associations were found with other CMR measures available for analysis and no association was observed between scoliosis and diabetes (table 2).
Altered cardiac PDSR in participants of the UKB with scoliosis
Surface to surface analysis of participants with scoliosis shows increased cardiac compression
A 3D surface-to-surface analysis was performed on 21 088 participants of the cohort. The 3D cardiac modelling of patients with scoliosis showed increased strain at the top and bottom of the heart (figure 2). Radial cardiac decompression (sides of the heart) was also observed in participants with scoliosis. However, these were not significant when adjusting for the number of comparisons and covariates.
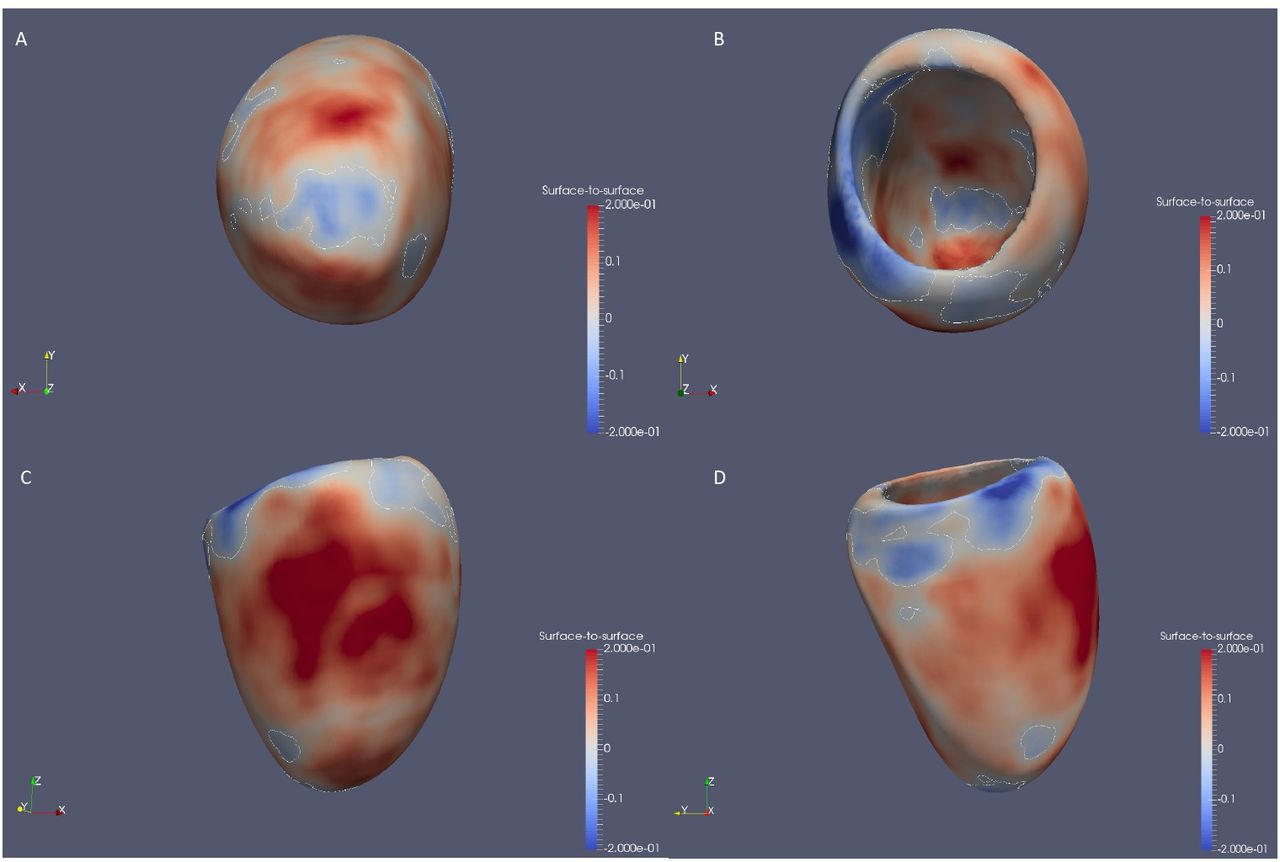
Surface to surface analysis suggests a compressed heart in participants with scoliosis. 3D models of left ventricle geometry with standardised beta-coefficients which show the association between scoliosis and regional surface-to-surface distance. Blue, increased inward pressure; red, increased outwards pressure. 3D, three-dimensional.
Lifetime risk of MACEs is increased in participants with scoliosis
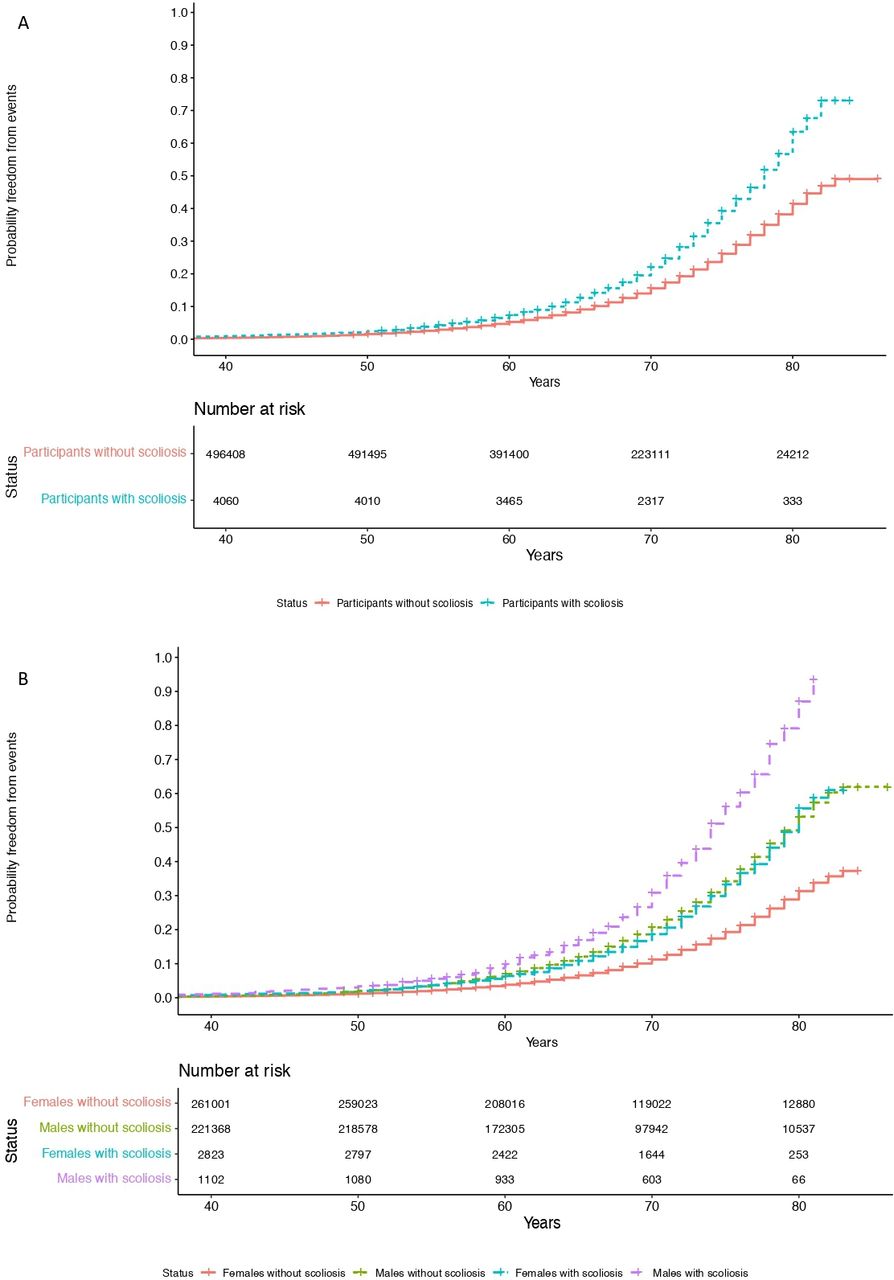
A significantly increased lifetime risk of MACEs was observed for UKB participants with scoliosis (figure 3; HR=1.45, p<0.001; stratified by sex, HR=1.63, p<0.001), mainly driven by heart failure (HR=1.58, p<0.001) and atrial fibrillation (HR=1.54, p<0.001). The probability of MACE doubled in men into older age (from 60 years of age). This may be caused through the altered cardiac diastolic strain rates observed in participants with scoliosis. However, we emphasise caution regarding the causality of this association of scoliosis and MACEs at this stage.
{kind=link}
{kind=link}
{kind=link}
Increased lifetime risk of MACEs in UKB participants with scoliosis. Cumulative incidence curves depict (A) an increase in lifetime risk of MACE in participants with scoliosis over time (HR=1.45, p<0.001) and (B) stratified by sex (HR=1.63, p<0.001). MACEs, major adverse cardiovascular events; UKB, UK Biobank.
Discussion
Participants with scoliosis have an increased lifetime risk of MACEs
To the best of our knowledge, this is the first study to identify an increased lifetime risk of MACEs, through atrial fibrillation and heart failure, in participants with scoliosis. This may be through the identified, significantly increased PDSRrr and decreased PDSRll. The abnormal curvature of the spine can increase mechanical constraint on the heart which may result in diastolic dysfunction22 and the severity of the spinal deformity has been shown to aggravate ventricular and right atrial pressure.3
It is unlikely that the observed heart failure is due to blood pressure abnormalities as no significant differences were found in measured SBP and DBP between participants with scoliosis and the rest of the population. However, it is possible that pulmonary dysfunction may be eliciting cardiac dysfunction alongside atrial fibrillation, in patients with advanced scoliosis.3 11 23 These findings suggest that early medical intervention in patients with scoliosis through surgery may decrease the risk of a future MACEs, however, future validation of this finding is needed in a scoliosis case cohort. It may be possible that scoliosis develops secondary to other diseases that could also increase the risk of MACEs. Future genetic analyses would be beneficial to assess causality through Mendelian randomisation techniques. Likewise, future studies are required to determine whether the cardiovascular changes observed are reversible with scoliosis treatment surgery.
A previous study assessed 201 patients with scoliosis for cardiopulmonary changes following corrective scoliosis surgeries and suggested that untreated scoliosis can result in pulmonary dysfunction and subsequently lead to right heart failure, increasing mortality.3 Postoperative normalisation of cardiac measures was observed in this study, highlighting the potential benefits of surgical correction of scoliosis on cardiac function.3 Additionally, a long-term follow-up study showed increased risk of pulmonary limitations such as shortness of breath in patients with untreated scoliosis, aggravated by spinal curvature.24
It is challenging to accurately assess the cardiac function of patients with scoliosis, due to the heart being displaced22 and participants with scoliosis in the UKB had significantly less CMR scans available, possibly due to lack of comfort for prolonged periods of time in MRI machines. Adaptations may be required to allow patients with scoliosis to undergo MRI scans more comfortably and to further assess any alteration in cardiac function in patients with scoliosis.
Participants with scoliosis have altered cardiac diastolic strain rates
In the UKB, participants with scoliosis showed increased pressure at the top and bottom of the heart, as well as elongation of the sides of the heart. These results concur with the 2D-derived CMR findings of significantly increased PDSRrr and decreased PDSRll. A reduced PDSRll has been previously associated with reduced left atrial function.21 No significant associations were found with the other studied CMR traits, suggesting that this compression does not alter blood flow through the heart. This altered cardiac strain may be explained by the deformity of the thoracic cage in scoliosis limiting cardiac diastolic movement. The mechanical abnormalities of the thoracic spine as well as the impact on the pulmonary system may be the primary cause of the heart involvement.25 26 Secondary involvement via altered pulmonary haemodynamics may be possible, where spinal curvature impacts pulmonary pressures leading to pulmonary hypertension. Likewise, direct compression of the myocardium could occur in conjunction with pulmonary involvement. These events can contribute to the development of cardiac consequences in patients with scoliosis.27 It would be beneficial to include cardiac follow-ups in patients with scoliosis to observe any cardiac alterations as scoliosis progresses, ensuring early intervention.
Prevalence of scoliosis in the UKB
We report a prevalence of scoliosis of 0.8% in the UKB population cohort. Previous literature has reported a scoliosis prevalence of 8% in adult volunteers aged over 40 years old.5 Patients included in the previous clinical study were recruited on evaluation of bone mineral density and thus were likely at increased risk of scoliosis compared to the UKB population cohort. Additionally, this discrepancy may be due to the limitations of the UKB cohort (see the Limitations section).
Participants with scoliosis in the UKB are more elderly compared with the rest of the population, regardless of sex. Scoliosis occurs alongside other diseases such as osteoporosis or degenerative spine disorders with increasing age.5
In the UKB cohort, scoliosis is more commonly found in women than men (2.5:1), which agrees with a previous scoliosis case cohort study of adolescents and adults that reported a ratio of scoliosis in women to men as 2:1.28 Although not fully understood, there are different theories linking the higher prevalence of scoliosis in women, including the implication of the autonomic nervous system in skeletal growth and/or puberty through leptin hormone, which has been found decreased in female patients with idiopathic scoliosis.1 29 30 Analyses to determine causality would aid our current understanding of the mechanisms behind scoliosis. Furthermore, it has been reported that approximately 30% of women (n=324) suffer from systemic osteopenia which strongly contributes to the progression of spinal curvature in adolescent females following skeletal maturity.8
Limitations
The participants in the UKB cohort were recruited at 40–69 years of age and most participants are of European ancestry. Selection bias for inclusion in CMR subcohort may have excluded participants with more severe scoliosis from the study. In addition, discrimination of scoliosis aetiology was mostly unspecified and information was not available on measures of scoliosis severity.
Conclusions
This work describes for the first time in an adult population, evidence for altered cardiac function in adult participants with scoliosis. We identified altered diastolic strain, increased lifetime risk of MACE driven by heart failure and atrial fibrillation, and observed cardiac compression in the UKB participants with scoliosis. Further research is required to follow-up the role of scoliosis in cardiac manifestations in a clinical setting.
Supplemental material
Data availability statement
UK Biobank (https://www.ukbiobank.ac.uk/) population reference datasets are publicly available. Analysis code is available on GitHub (https://github.com/ImperialCardioGenetics/Scoliosis).
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the UK Biobank (UKB). The UKB recruited over 500 000 participants aged 40–69 years across the UK between 2006 and 2010 (National Research Ethics Service, 11/NW/0382, 21/NW/0157). This project was conducted under the UK Biobank applications 47602 and 40616. All participants provided written informed consent. Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @quintero_val, @DrDeclanORegan, @drjamesware, @KathrynMcGurk
Contributors KAM is the guarantor and conceptualised the project. KAM and VQS contributed to methodology. VQS and AC contributed to formal analysis. JSW and DPO’R contributed to resources. KAM and VQS contributed to data curation. VQS wrote the original draft. AC, DPO’R, JSW and KAM contributed to writing–review & editing. VQS and AC contributed to visualisation. KAM and JSW contributed to supervision.
Funding This work was supported by the British Heart Foundation (RG/19/6/34387, RE/18/4/34215, FS/IPBSRF/22/27059),Wellcome Trust (107469/Z/15/Z; 200990/A/A/16/Z), Medical Research Council (UK), and the NIHR Imperial College Biomedical Research Centre. The views expressed in this work are those of the authors and not necessarily those of the funders. For open access, the authors have applied a CC BY public copyright license to any Author Accepted Manuscript version arising from this submission.
Competing interests JSW has consulted for MyoKardia, Foresite Labs and Pfizer. DPO has consulted for Bayer.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.