Article Text

Abstract
Objective Patients with stress-related disorders and anxiety are at increased risk of developing cardiovascular disease. However, the risk of out-of-hospital cardiac arrest (OHCA) is scarcely investigated. We aimed to establish whether long-term stress (post-traumatic stress disorder, adjustment disorder) or anxiety is associated with OHCA in the general population.
Methods We conducted a nested case–control study in a nationwide cohort of individuals between 1 June 2001 and 31 December 2015 in Denmark. Cases were OHCA patients with presumed cardiac causes. Each case was matched by age, sex and date of OHCA with 10 non-OHCA controls from the general population. HRs for OHCA were derived from Cox models after controlling for common OHCA risk factors. Stratified analyses were performed according to sex, age and pre-existing cardiovascular disease.
Results We included 35 195 OHCAs and 351 950 matched controls (median age 72 years; 66.8% male). Long-term stress conditions were diagnosed in 324 (0.92%) OHCA cases and 1577 (0.45%) non-OHCA controls, and were associated with higher rate of OHCA (HR 1.44, 95% CI 1.27 to 1.64). Anxiety was diagnosed in 299 (0.85%) OHCA cases and 1298 (0.37%) controls, and was associated with increased rate of OHCA (HR 1.56, 95% CI1.37 to 1.79). We found no interaction with sex, age or history of cardiovascular diseases.
Conclusion Patients with stress-related disorders or anxiety have an increased rate of OHCA. This association applies equally to men and women and is independent from the presence of cardiovascular disease. Awareness of the higher risks of OHCA in patients with stress-related disorders and anxiety is important when treating these patients.
- ANXIETY
- EPIDEMIOLOGY
- Arrhythmias, Cardiac
- Electronic Health Records
Data availability statement
No data are available. Data underlying the present article are not available to be shared publicly, as access to Danish registry raw data for research purposes must be granted individually by Danish authorities.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Patients with stress-related disorders and anxiety are at increased risk of developing cardiovascular disease. However, the risk of out-of-hospital cardiac arrest (OHCA) is scarcely investigated.
WHAT THIS STUDY ADDS
We estimated overall and stratified HRs of OHCA associated with long-term stress conditions (ie, post-traumatic stress disorder, adjustment disorder) or anxiety using a large cohort that was specifically designed to study OHCA in the general Danish population (total 35 195 cases with OHCA).
Stress-related disorders or anxiety are associated with an increased rate of OHCA. This association applies equally to men and women and is independent from the presence of cardiovascular disease.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study raises awareness of the higher risks of OHCA and early risk monitoring to prevent OHCA in patients with stress-related disorders and anxiety.
Introduction
Out-of-hospital cardiac arrest (OHCA) is a leading cause of mortality and is estimated to be accountable for 20% of all natural deaths and for up to 50% of all cardiovascular deaths in the affluent world.1 OHCA predominantly results from lethal cardiac arrhythmias (ventricular tachycardia/ventricular fibrillation) that occur most frequently in the setting of coronary heart disease.2 Increasing evidence, however, demonstrates that OHCA also increases by non-cardiac diseases.3
Stress-related disorders and anxiety are associated with multiple types of cardiovascular diseases4 5 and previous studies show an over-representation of these disorders among victims of cardiac arrest.4 6–11 Dysregulation of cardiac ion channels by the autonomic nervous system, in particular through sympathovagal imbalance, in combination with unhealthy lifestyle (ie, smoking, poor diet, lower physical activity) and metabolic abnormalities (ie, hypercholesterolaemia, immune dysregulations) are proposed as underlying mechanisms.4 9 12 Previous studies on OHCA, however, are limited by the inclusion of low number of cardiac arrests,6–8 11 12 retrieve data from selected populations8–12 or use in-hospital diagnosis to identify cardiac arrest patients.4 The latter may result in important inclusion bias by omitting OHCA patients who died prior to hospital admission. Thus, data on the risk of OHCA in large, unselected cohort of patients with OHCA are sparse. Filling this knowledge gap is needed considering the low survival chances after cardiac arrest in these patients.13 Accordingly, using a large unselected cohort of patients with OHCA from the Danish health registries, we investigated whether long-term stress conditions (ie, post-traumatic stress disorder, adjustment disorder) or anxiety were associated with OHCA in the general population. We stratified according to sex, age and cardiovascular disease (ischaemic heart disease, heart failure) to identify which risk factor confers the highest risk of OHCA in patients with long-term stress conditions or anxiety.
Methods
Patient and public involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
Study design and population
We conducted a nested case–control study in a nationwide cohort of individuals in the period between 1 June 2001 and 31 December 2015. Cases were patients who suffered OHCA with presumed cardiac causes from the Danish Cardiac Arrest Registry (DANCAR). We excluded OHCAs with obvious non-cardiac causes (eg, drug intoxication/overdose, drowning, trauma). Each OHCA case was matched using risk set matching based on age, sex and the index date (date of OHCA) with 10 non-OHCA controls who were alive on the index date from the general population, a study design used previously by this research group.14 15
Data sources
Data for this study were obtained from the Danish nationwide registries that have been described previously.14 15 In short, records at an individual patient level across the registries were cross-linked by the unique identification number that is allocated to each Danish citizen at birth or immigration. By doing so, it is possible to follow each Danish citizen longitudinally with respect to death, immigration, drug use and all inpatient and outpatient hospital contacts, allowing large-scale research with nationwide coverage. This study was based on data from the following registries: (1) the Danish Civil Registry containing information on date of birth, sex, immigration and emigration; (2) the Danish National Patient Registry containing data on all hospital diagnoses, procedures and operations coded according to the International Classification of Diseases 10th revision (ICD-10); (3) the National Prescription Register containing information on complete drug-dispensing records classified according to the Anatomical Therapeutic Chemical classification code (ATC code); (4) the Danish Registry of Causes of Death providing information about primary and contributing causes of death; (5) The Danish Psychiatric Central Research Register providing information on psychiatric hospitalisations and ambulatory contacts and (6) the DANCAR holding high-quality data on all OHCAs in Denmark since June 2001 according to the Utstein guidelines.14 The OHCA data have been systematically collected and reported by the emergency medical services (EMS) personnel to the DANCAR. An OHCA is included when a clinical condition of cardiac arrest results in cardiopulmonary resuscitation either by bystanders (with activation of EMS personnel) or by EMS personnel. The capture of OHCA cases is nearly complete because the EMS is activated for all clinical emergencies in Denmark and are obliged to fill out a case report for every attended OHCA providing information on important factors related to the OHCA. The presumed cause of OHCA was retrieved from the death certificates and discharge diagnosis codes. OHCAs with diagnosis codes for cardiac disease, unknown disease or unexpected collapse were classified as being of presumed cardiac cause. These registries have been used previously by this research group.14 15
Exposure of interest
We identified patients with long-term stress disorders (ICD: F43.1, F43.2) or anxiety (ICD: F40, F41) using the diagnosis codes from hospital admissions or ambulatory contacts registered the Danish National Patient Register or Danish Psychiatric Central Research Register up to 10 years prior to index date. Post-traumatic stress disorders (ICD: F43.1) and adjustment disorders (ICD: F43.2) comprised the long-term stress condition. The presence of long-term stress disorders or anxiety was defined as mutually exclusive and was analysed separately.
Covariates
The following well-known risk factors of OHCA were identified up to 10 years prior to index date: heart failure, ischaemic heart disease, cerebrovascular disease, atrial fibrillation, peripheral artery disease, diabetes mellitus and depression. Since the diagnosis code of diabetes mellitus has a low sensitivity in the Danish registries, the presence of diabetes was defined using redeemed prescription of glucose-lowering drugs within 6 months prior to index date as done previously.14 15 Concomitant drug treatment was defined as one or more redeemed prescription at any pharmacy in Denmark up to 6 months prior to index date. We assessed the following drug use: beta-blockers, calcium-channel blockers, diuretics, renin–angiotensin system inhibitors, diuretics, antithrombotics, nitrates, Vaughan-Williams class I or III antiarrhythmic drugs, anxiolytics, antidepressants and QT-interval prolonging drugs. Drugs with QT-prolonging potential were defined using the CredibleMeds list.16 For antimicrobial drugs with QT-interval prolonging potential drugs, we shortened the exposure time to 14 days before the index date as these drugs are generally prescribed for shorter periods. An overview of all the used ICD-10 and ATC-codes are provided in online supplemental table 1.
Supplemental material
Statistical analyses
We used Cox proportional regression model to estimate the association between long-term stress disorders and the rate of OHCA, and between anxiety and the rate of OHCA, by calculating the HR and the associated 95% CI. We calculated both crude estimates (unadjusted analysis) and adjusted estimates by performing multivariable analysis adjusted for the following prespecified confounders: heart failure, ischaemic heart disease, cerebrovascular disease, atrial fibrillation, peripheral artery disease, diabetes mellitus, depression and the use of QT-prolonging drugs. We further investigated the relation of long-term stress or anxiety with OHCA by stratifying according to sex and age. Next, to investigate a possible confounding effect by the presence of cardiovascular disease, we studied the relation of long-term stress conditions or anxiety with OHCA stratified according to the presence of cardiovascular disease. By performing stratified analyses according to cardiovascular disease our original matching was lost, hence we additionally adjusted for age and sex in our model as we did previously.14 15 The presence of interaction on a multiplicative scale between our exposure of interest and sex, age and cardiovascular disease was estimated by consecutively including the cross-product of the two factors as a variable in the model. A two-tailed p<0.05 was considered indicative of significant difference among groups. Next, the relationship between the exposure of interest (ie, long-term stress disorders, anxiety) and OHCA was studied in individuals without the comorbidities from table 1 (ie, cardiovascular comorbidities, depression) and without the use of cardiovascular drugs, QT-prolonging drugs and antidepressants. Finally, we compared whether patient characteristics or concomitant medication use was different between the exposure categories among cases. The study population was described as cases and controls using the χ2 test for categorical variables and the Mann-Whitney test for continuous variables. For this study, we used the same dataset as we for our previous studies.14 15 Therefore, table 1 with baseline characteristics in this study is largely overlapping with table 1 of our previous studies.14 15
Baseline characteristics of the study population
Results
Patient characteristics
The study population consisted of 35 195 OHCAs with presumed cardiac causes and 351 950 matched controls without OHCA from the general population (figure 1). The median age was 72 years and 66.8% were male (table 1). The prevalence of comorbidities was higher among OHCA cases compared with non-OHCA controls. Likewise, use of cardiovascular drugs and QT-prolonging drugs was more prevalent among OHCA cases than in non-OHCA controls.

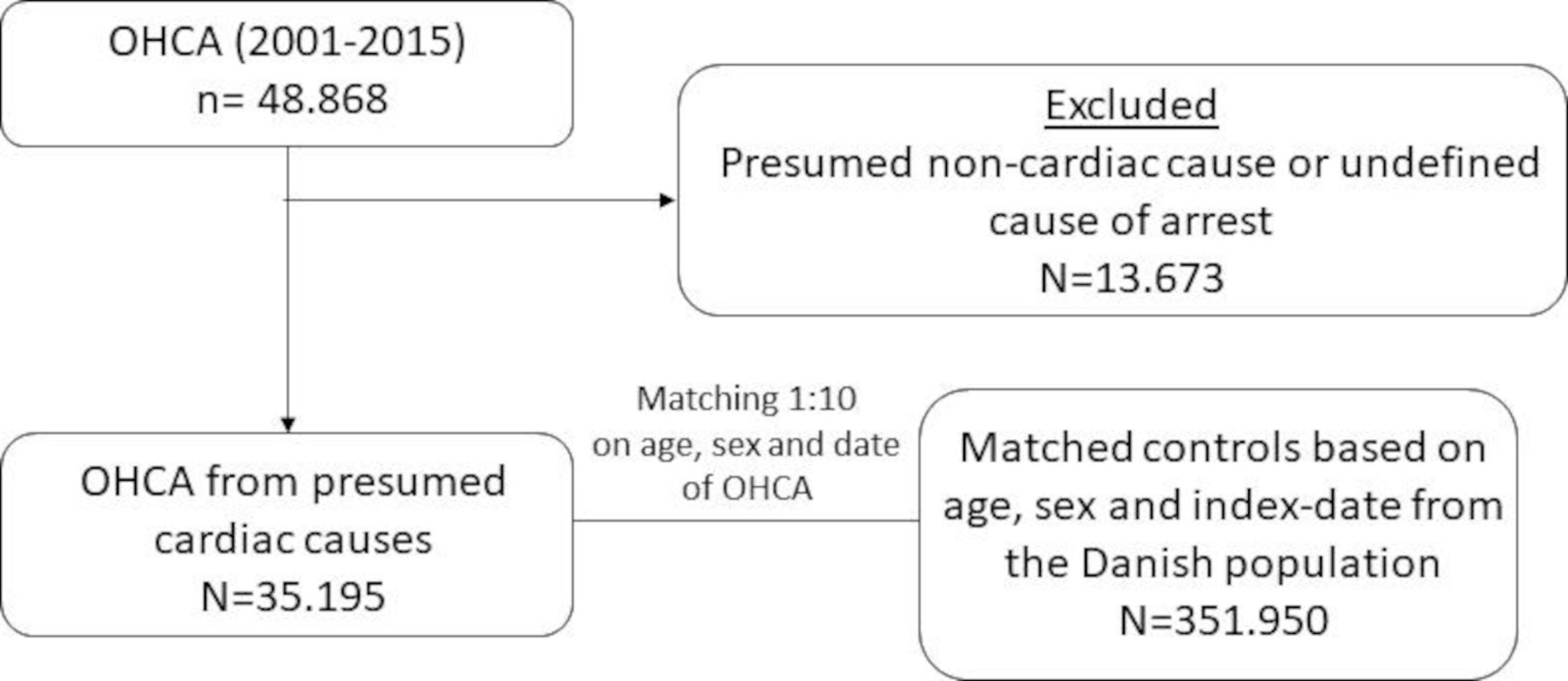{kind=link}
Flow chart of patient inclusion OHCA, out-of-hospital cardiac arrest.
Estimated HRs of OHCA for stress-related disorders and anxiety in the general population
Long-term stress conditions were diagnosed in 324 (0.92%) OHCA cases and 1577 (0.45%) non-OHCA controls, and were associated with higher rate of OHCA after adjustments for common OHCA risk factors (HR 1.44, 95% CI 1.27 to 1.64, table 2). Both post-traumatic stress disorder (HR 1.80, 95% CI 1.13 to 2.86) and adjustment disorders (HR 1.42, 95% CI 1.24 to 1.63, online supplemental table 2) were independently associated with increased OHCA rate. Anxiety was diagnosed in 299 (0.85%) OHCA cases and 1298 (0.37%) non-OHCA controls and was associated with increased rate of OHCA (HR 1.56, 95% CI 1.37 to 1.79, table 2). Our results did not change significantly when also adjusting for the use of anxiolytics and antidepressants. When we studied the prevalences of concomitant medication use or comorbidities in the different exposure categories among cases, we found that depression was more frequent among patients with long-term stress and anxiety than individuals with neither of the two diagnoses. Also, patients with long-term stress and anxiety more often used anxiolytics, antidepressants and QT-prolonging drugs (online supplemental table 3).
HR of out-of-hospital cardiac arrest (OHCA) in patients with long-term stress conditions or anxiety as compared with patients with neither of the two diagnoses
Stratified analyses
Stratified analyses according to sex showed that OHCA rate was increased both in women (HRlong-term stress 1.44, 95% CI 1.18 to 1.76; HRanxiety 1.73, 95% CI 1.44 to 2.07) and in men (HRlong-term stress 1.45, 95% CI 1.22 to 1.72; HRanxiety 1.39, 95% CI 1.13 to 1.69), and that this OHCA rate was not significantly different between the groups (p value interaction: stress-related disorders: 0.6594, anxiety: 0.1895, table 3). Stratification according to age showed that the estimates for the association between long-term stress disorders and OHCA rate, and between anxiety and OHCA rate, did not differ significantly between the age groups (p value interaction: stress-related disorders: 0.0639, anxiety: 0.5647, table 4). Finally, when we performed stratified analyses according to the presence of cardiovascular disease, we observed no statistically significant difference in OHCA rate between patients with and without cardiovascular disease (p value interaction: stress-related disorders=0.8973, anxiety=0.5988, table 5). Similarly, the HRs did not vary significantly by the presence of ischaemic heart disease or heart failure (online supplemental tables 4 and 5). Finally, the HRs remained elevated when we studied the association with OHCA of long-term stress conditions and anxiety in individuals without the comorbidities from table 1 (ie, cardiovascular comorbidities, depression) and without the use of cardiovascular drugs, QT-prolonging drugs and antidepressants (online supplemental table 6).
HR of out-of-hospital cardiac arrest (OHCA) in patients with long-term stress conditions or anxiety: stratification according to sex
HR of out-of-hospital cardiac arrest (OHCA) in patients with long-term stress conditions or anxiety: stratification according to age
HR of out-of-hospital cardiac arrest (OHCA) in patients with long-term stress conditions or anxiety: stratification according to cardiovascular disease
Discussion
In this study, we showed that long-term stress disorders (post-traumatic stress and adjustment disorders) or anxiety were associated with increased OHCA rate in the general population. The association persisted when the outcome was corrected for common OHCA risk factors. This association applied to men and women and was independent from the presence of cardiovascular disease.
Comparison with previous studies
Stress-related disorders and OHCA
Our finding that stress-related disorders or anxiety were associated with increased rate of OHCA are supported by previous studies.4–12 A case–control study showed that cardiac arrest patients had experienced a higher number of major life events in the year prior to the cardiac arrest than had matched controls, and that experiencing major life events were associated with a higher risk of cardiac arrest.6 These findings were supported by a case-crossover study, where higher occurrence of major life events in the month compared with the previous 5 months prior to cardiac arrest was reported.7 In contrast, a case–control study in 81 American women described no difference in experiencing stressful life events within 6 months prior to cardiac death compared with matched controls, although cases experienced more often the death of a significant other than matched controls.8 Previous studies, however, had limited sample size.6–8 Also, the presence of stressful life event was based on interview with spouses or family, thereby increasing the risk of information bias. Finally, Song et al investigated the risk of cardiovascular disease, including cardiac arrest, in a large cohort of 136 637 patients with stress-related disorders compared with matched controls, and found a significant higher risk of cardiac arrest in those with stress-related disorders.4 The study, however, relied solely on inpatient and outpatient diagnosis to define cardiac arrest, and omitted patients who died before reaching the hospital. Such inclusion criteria may result in important inclusion bias, particularly since psychiatric disorders have been associated with lower survival rates after OHCA.13 In our study, the capture of OHCA is nearly complete due to our collaboration with all EMS departments. This allowed us to enrol both patients who survived to hospital admission and those who died before reaching the hospital, thereby minimising inclusion bias by the use of an unselected cohort of OHCA patients. Further, misclassification of the outcome may have occurred in the study by Song et al4 since the cohort was not specifically designed to study OHCA and properly adjudicating OHCA victims is challenging.
Anxiety and OHCA
Our finding that anxiety was associated with higher rate of OHCA is in line with a previous study reporting a trend towards an increased risk of sudden cardiac death associated with high anxiety scores in a sample of women with no history of cardiovascular disease or cancer.9 Other studies of men with anxiety have described that high anxiety scores were associated with increased risk of sudden cardiac death.10 11 These previous studies, however, included small number of cardiac arrest patients,9–11 and no adjustments for important risk factors of OHCA, such as heart failure,10 11 diabetes mellitus11 and/or QT-prolonging drugs,9–11 were performed. Finally, studies in populations at risk for OHCA are equivocal. One study showed that anxiety was associated with an increased risk of ventricular arrhythmias 1 year after ICD implantation,12 while another study reported no association between anxiety and ventricular arrhythmias.17
Are long-term stress conditions and anxiety independent risk factors for OHCA?
Numerous studies demonstrated associations of stress-related disorders or anxiety with cardiovascular outcomes such as myocardial infarction, heart failure and cerebrovascular disease.4 5 These disease states might be biological mediators in the causal pathway of OHCA. Consequently, these disorders could contribute, to some extent, to increased OHCA rate associated with stress-related disorders and anxiety observed in our study. Nevertheless, both stress-related disorders and anxiety remained significantly associated with OHCA after controlling for these variables in the multivariable analyses, suggesting that it is unlikely that traditional risk factors of OHCA alone explain this relationship. Moreover, the elevated OHCA rate associated with stress-related disorders and anxiety in subjects without cardiovascular disease provides additional support for the notion that both stress-related disorders and anxiety may be directly related to OHCA.
The relation between stress and anxiety with sudden death has been long established10 11 18 and is likely mediated by the activity of the sympathetic autonomic nervous system.19 20 Indeed, a decrease in heart rate variability is a measure for an increase of the activity of the sympathetic nervous system and has been used as a biomarker for the increased risk of cardiac mortality.21 On the other hand, treatment with β-adrenoceptor blocking drugs is recommended to reduce cardiac mortality and prevent ventricular tachyarrhythmias.22 The exact mechanistic explanation of the proarrhythmic effects of increased sympathetic activity on the heart is still incompletely known. Increased sympathetic neural activity leads to an increase in heart rate, release of neurotransmitters into the circulation and local release of neurotransmitters in the heart.20 23 Each of these factors may potentially influence cardiac electrophysiology and facilitate ventricular arrhythmias and OHCA.20 23 Local release of catecholamines is related to changes in local action potential duration. The local effects have a sidedness, with stimulation of the left stellate ganglion leading to first a short increase and then a prolonged decrease of action potential duration in the left lateral and posterior wall, while right stellate stimulation shows these changes in the right ventricular wall and the left ventricular anterior wall of pigs.24 A shortening of action potential duration (and of the effective refractory period) is proarrhythmic in the setting of reentrant arrhythmias in two ways. First, it leads to shortening of the wavelength and thereby to facilitation of reentrant arrhythmias.25 Second, if the shortening of the action potential duration occurs adjacent to a region of myocardial ischaemia, it may cause an increase in the end-systolic ‘current of injury’ and thereby promote the genesis of closely coupled premature beats that may initiate reentry.26 Generalised release of noradrenalin from the adrenal glands has been studied by superfusing myocardial fibres or cells with fluids containing increased catecholamines. Superfusion human myocytes with norepinephrine leads to action potential prolongation and triggered activity based on early after depolarisations.27
In addition to a biological mechanism, behavioural and psychosocial factors may also contribute to OHCA risk. Stress-related disorders and anxiety often lead to unhealthy lifestyle, such as smoking and lower physical activity, which in turn may increase the risk of OHCA. In our study, we could not adjust for these factors since we had no data on these features to include in our statistical analyses. On the other hand, if such behaviours lie in the causal pathway between our exposure and OHCA, then treating them as confounders in the multivariable analyses, might underestimate the overall impact of stress-related disorders and anxiety on OHCA risk. Moreover, it is unlikely that knowledge of these factors would have altered our conclusions considering that we have adjusted for all the relevant cardiovascular comorbidities. Finally, other psychiatric disorders, such as the presence of depression, may contribute to OHCA risk. However, it is unlikely that depression accounts for our observed association in this study, since we adjusted for depression in the multivariable analyses.
Strengths and limitations
A main strength of this study is its population-based design in which large and unselected number of OHCA patients were obtained from nationwide databases, thereby minimising the risk of inclusion bias and selection bias and increasing the likelihood that our results are applicable to the community at large. Also, DANCAR was specifically designed to study OHCA, which allows accurate data collection for each OHCA patient. Nevertheless, the lack of information from primary care might have led to underestimation of the number of patients with milder forms of stress-related disorders or anxiety. Consequently, our results may not be directly applicable to subjects with less severe stress/anxiety or daily stress. Another limitation is that data on disease severity were not available in our analyses since information regarding diagnosis was defined as a binary variable. Third, we cannot exclude that residual confounders may have affected our results as we had no information on several risk factors such as smoking and alcohol consumption that may have contributed to the observed associations. Also, we had no data on left ventricular ejection fraction to include in our multivariable analyses. However, given the highly unpredictable way in which OHCA occurs, it is very difficult, if not impossible, to obtain such data shortly before the occurrence of OHCA in a uniform manner across the studied population. Fourth, higher prevalence of comorbidities among OHCA cases may result in higher diagnosis of stress-related conditions compared with non-OHCA controls in which having stress-related conditions is probably less diagnosed, as non-OHCA controls may seek less medical care. This, in turn, could result in overestimation of the OHCA risk associated with long-term stress conditions and anxiety. To deal with this, we performed an additional subgroup analyses by selecting only individuals without the comorbidities from table 1 (ie, cardiovascular comorbidities, depression) and without the use of cardiovascular drugs, QT-prolonging drugs and antidepressants. By doing this, we aimed to make cases and controls more comparable with respect to seeking medical care. Here, we confirmed our main findings that long-term stress conditions and anxiety (online supplemental table 6) were associated with higher risk of OHCA. Finally, the diagnosis codes used to identify stress-related disorders or anxiety have not been validated previously which may lead to misclassification bias. However, the majority of the information recorded in the Danish National Patient Registry has undergone scrutiny for data quality and shows high validity.28
Conclusion
Patients with stress-related disorders (post-traumatic stress and adjustment disorders) or anxiety have a higher rate of OHCA compared with those without these conditions. The association persisted when the outcome was corrected for common OHCA risk factors. This association applies to men and women and is independent from the presence of cardiovascular disease. Awareness of the higher risks of OHCA in patients with stress-related disorders and anxiety is important when treating these patients.
Data availability statement
No data are available. Data underlying the present article are not available to be shared publicly, as access to Danish registry raw data for research purposes must be granted individually by Danish authorities.
Ethics statements
Patient consent for publication
Ethics approval
The study is approved by the Danish Data Protection Agency (Ref.no. 2007-58-0015, local ref.no. GEH-2014-017, I-Suite 0.2735). No further approval from an ethics committee is required for register-based studies in Denmark.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors TEE conceived the study idea. TEE and GG designed the research (methods). TEE performed the statistical analyses and wrote the manuscript. All authors critically revised and approved the manuscript. TEE and GG are responsible for the overall content as guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests LVK has the last 3 years been a consultant for Lundbeck and Teva.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.