Article Text

Abstract
Background and aims Randomised controlled trials comparing transcatheter aortic valve replacement (TAVR) and surgical aortic valve replacement (SAVR) were performed in highly selected populations and data regarding long-term secondary complications beyond mortality are scarce. This study used data from Ontario, Canada to compare mid-term and long-term clinical outcomes in a representative real-world cohort of patients who underwent TAVR and SAVR from 2007 to 2016.
Methods A novel overlap weighting propensity score method was used to match patients undergoing TAVR or SAVR. Primary outcomes were all-cause, cardiovascular and non-cardiovascular mortality either in-hospital or at 1, 3 and 5 years postdischarge. Secondary outcomes included adverse outcomes and readmission. Long-term primary and secondary outcomes were compared using a weighted competing risks subdistribution proportional hazards model.
Results The study included 9355 SAVR and 2641 TAVR patients. All-cause mortality at 1 year (HR 1.21; 95% CI 1.02 to 1.43), 3 years (HR 1.45; 95% CI 1.28 to 1.64) and 5 years (HR 1.48; 95% CI 1.33 to 1.65) was significantly higher among patients underwent TAVR compared with SAVR, with both cardiovascular mortality at 3 and 5 years and non-cardiovascular mortality at 1, 3 and 5 years significantly higher for TAVR. Hazards of myocardial infarction and readmission for angina at 1, 3 and 5 years were significantly greater for TAVR.
Conclusions In this overlap weighted cohort, both cardiac and non-cardiac mortality rates were increased in TAVR patients. Residual or unmeasured confounding may have contributed to these findings. More studies are needed to identify factors predictive of long-term outcomes in real-world cohorts.
- transcatheter aortic valve replacement
- aortic valve stenosis
- outcome assessment, health care
Data availability statement
Data are available on reasonable request. The dataset from this study is held securely in coded form at ICES. While legal data sharing agreements between ICES and data providers prohibit ICES from making the data set publicly available, access may be granted to those who meet prespecified criteria for confidential access, available at www.ices.on.ca/DAS. The full data set creation plan and underlying analytic code are available from the authors upon request, understanding that the computer programs may rely upon coding templates or macros that are unique to ICES.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Several randomised control trials have evaluated the safety and efficacy of transcatheter aortic valve replacement (TAVR) compared with surgical aortic valve replacement (SAVR) and have reported either similar outcomes or improved survival for TAVR. However, these trials were performed in highly selected populations, limiting the generalisability to real-world patients with limited follow-up duration, and there remains a paucity of data regarding long-term secondary complications beyond mortality.
WHAT THIS STUDY ADDS
In this overlap weighted cohort, patients who underwent TAVR had increased hazards of long-term adverse complications, including myocardial infarction and angina compared with SAVR after accounting for multiple clinical comorbidities and the hospital frailty risk score. Excess mortality among TAVR patients was also observed but was increased for both cardiac and non-cardiac causes.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
More studies in the recent era and with long-term follow-up are needed to confirm the long-term clinical benefits of TAVR and to improve patient selection for these procedures.
Introduction
Aortic valve stenosis (AS) is the most common cardiac valve disease, affecting 3% of adults aged 65 and older and nearly 10% of those older than 80 years.1–3 Severe symptomatic AS is fatal and, if untreated, mortality can exceed 50% at 2 years.2 4 Surgical aortic valve replacement (SAVR) is the traditional method of aortic valve replacement and has been demonstrated to improve survival.5 More recently, transcatheter aortic valve replacement (TAVR) has emerged as a less invasive treatment option for patients with severe AS and is currently widely worldwide as an alternative to SAVR following the demonstration of its non-inferiority or superiority in clinical trials comparing TAVR to SAVR in patients at high, intermediate and more recently at low surgical risk at one or 2 years.6–9 Thus, TAVR has become the dominant form of AVR in most Western countries.10 11
However, concerns have been raised about the generalisability of these trial results to real-world patients because randomised controlled trials (RCTs) systematically exclude patients with certain clinical and anatomical characteristics, such as bicuspid valve, concomitant mitral/tricuspid or ascending aorta disease or recent neurological events.6 12 Thus, in a single-centre study, it has been shown that approximately 50% of patients deemed at low-surgical risk would have been ineligible in trials comparing TAVR and his counterpart SAVR.13 In addition, there is limited information on longer-term follow-up14–16 and a word of caution has been raised by several meta-analysis.17 18 Furthermore, data on several important secondary endpoints, such as incident atrial fibrillation, angina and reintervention are scarce.16 19 To address these issues, using population-based observational data from Ontario, Canada, we derived a longitudinal representative real-world cohort of patients who underwent SAVR or TAVR from 2007 to 2016 and compared in-hospital and long-term clinical outcomes for each procedure.
Methods
Study design and data sources
This retrospective population-based cohort study was conducted using population-based administrative databases housed at Institute for Clinical Evaluative Sciences (ICES), including the Canadian Institute for Health Information Discharge Abstract Database (CIHI-DAD) to ascertain clinical and demographic information, Ontario Health Insurance Plan (OHIP) Claims Database which captures universally available coverage for all hospital services, physician services and diagnostic tests, National Ambulatory Care Reporting System, which contains data for all hospital-based and community-based ambulatory care, the Ontario Drug Benefits Claims database to capture prescription history for individuals aged 65 and older, the Continuing Care Reporting System to identify admissions to long-term and continuing care, Registered Persons Database (RPDB) to obtain out-of-hospital mortality data, Ontario Census Area Profiles and Local Health Integration Networks. ICES is a prescribed entity under Ontario’s Personal Health Information Protection Act (PHIPA). Section 45 of PHIPA authorises ICES to collect personal health information, without consent, for the purpose of analysis or compiling statistical information with respect to the management of, evaluation or monitoring of the allocation of resources to or planning for all or part of the health system.
Study cohort
The cohort included all patients aged 18 or older who underwent a transfemoral TAVR (regardless of the type of TAVR devices) or isolated SAVR procedure for AS in Ontario, Canada from 1 April 2007 to 31 December 2016.
Outcomes
Primary outcomes were all-cause, cardiovascular and non-cardiovascular mortality at 1, 3 and 5 years and were evaluated from the procedure date until date of death or administrative censoring. In-hospital outcomes were identified from the DAD and deaths after discharge were identified from the RPDB.
Secondary outcomes included ischaemic stroke, haemorrhagic stroke, myocardial infarction, acute kidney injury, vascular complications (including mechanical valve complications, infection, embolism, fibrosis and haemorrhage), atrial fibrillation, endocarditis, permanent pacemaker implantation, defibrillator, reintervention and cause-specific readmission at 1, 3 and 5 years and were evaluated from discharge date. Secondary outcomes were identified using previously validated algorithms based on diagnostic codes from the DAD or ICES validated algorithms (details are shown in online supplemental table 1).
Supplemental material
Statistical analysis
Given that patients undergoing TAVR are more likely to have comorbidities and advanced age, a novel propensity score method, termed overlap weighting,20 was used to address the potential for confounding by indication. While inverse probability weighting is commonly used to address systematic differences in baseline characteristics in observational settings, subjects with extreme propensity scores may have inaccurate or unstable weights and often dominate results or are excluded due to imprecision.21 22 Overlap weighting addresses these limitations by assigning each subject a weight equal to the probability of being assigned to the opposite intervention group.20 22 Previous literature has demonstrated the validity of this propensity score method that mimics attributes of an RCT.20
Patients were weighted using a propensity score for undergoing TAVR estimated from a multivariable logistic regression model containing age, sex, Charlson Comorbidity Score, frailty, myocardial infarction, stroke, dementia, chronic dialysis, cancer, chronic obstructive pulmonary disease, previous surgery and chronic lung disease. Age and sex were collected from the RPDB. Charlson Comorbidity Score was defined as the predicted mortality by weighting comorbid conditions23 and frailty was defined using the Hospital Frailty Risk Score.24 Myocardial infarction, stroke, chronic dialysis and cancer were identified based on diagnostic codes from the DAD and OHIP Claims Database fee codes. Dementia was identified based on ICES validated algorithms (online supplemental table 1).17 25 Baseline characteristics were then compared for the two groups using standardised differences (table 1).
Baseline characteristics before and after propensity matching using overlap weighting
In-hospital outcomes in the overlap weighted cohort were compared using logistic regression. ORs and corresponding 95% CI are presented in table 2. Primary and secondary outcomes for patients undergoing TAVR versus SAVR were compared using overlap propensity score-weighted competing risks sub-distribution proportional hazards models.26 HRs and corresponding 95% CIs are presented in table 3.
In-hospital outcomes
Primary end points at 1, 3 and 5 years
Sensitivity analysis
This study included all types of TAVR devices, which may be related to the postsurgical outcomes. Thus, in a sensitivity analysis, the fiscal year was adjusted in the calculation of weights to account for the increasing usage of TAVR devices over the study period. To account for potential confounding due to initiation of cardiovascular medications during follow-up, including statins, anticoagulants and antihypertensives, sensitivity analyses were conducted by adding new onset of cardiovascular medications separately to the calculation of weights.
Results
Study population
Before propensity matching, a total of 3036 patients undergoing TAVR (mean age 82.54 years; female 45.93%) and 18 396 patients undergoing SAVR (mean age 68.59 years; female 41.21%) were identified. After propensity matching using overlap weighting, the matched cohort included 9355 SAVR (mean age 79.43 years; female 45.50%) and 2641 TAVR patients (mean age 79.43 years; female 45.50%) (table 1). As shown in table 1, patients in the TAVR and SAVR cohorts were similar and comparable in baseline characteristics after propensity matching.
In-hospital outcomes
In-hospital outcomes are presented in table 2. Rates and likelihood of in-hospital all-cause mortality were similar for matched TAVR and SAVR patients (3.41% vs 1.83%; OR 0.83; 95% CI 0.60 to 1.15). Rates and likelihood of in-hospital endocarditis (≤0.23% vs 0.64%; OR 0.15; 95% CI 0.05 to 0.47) and atrial fibrillation (2.39% vs 7.79%; OR 0.24; 95% CI 0.17 to 0.32) were significantly lower in the TAVR group. Rate of pacemaker implantation (11.32% vs 4.32%; OR 2.06; 95% CI 1.67 to 2.53) were significantly higher in the TAVR group than in the SAVR group.
Primary outcomes
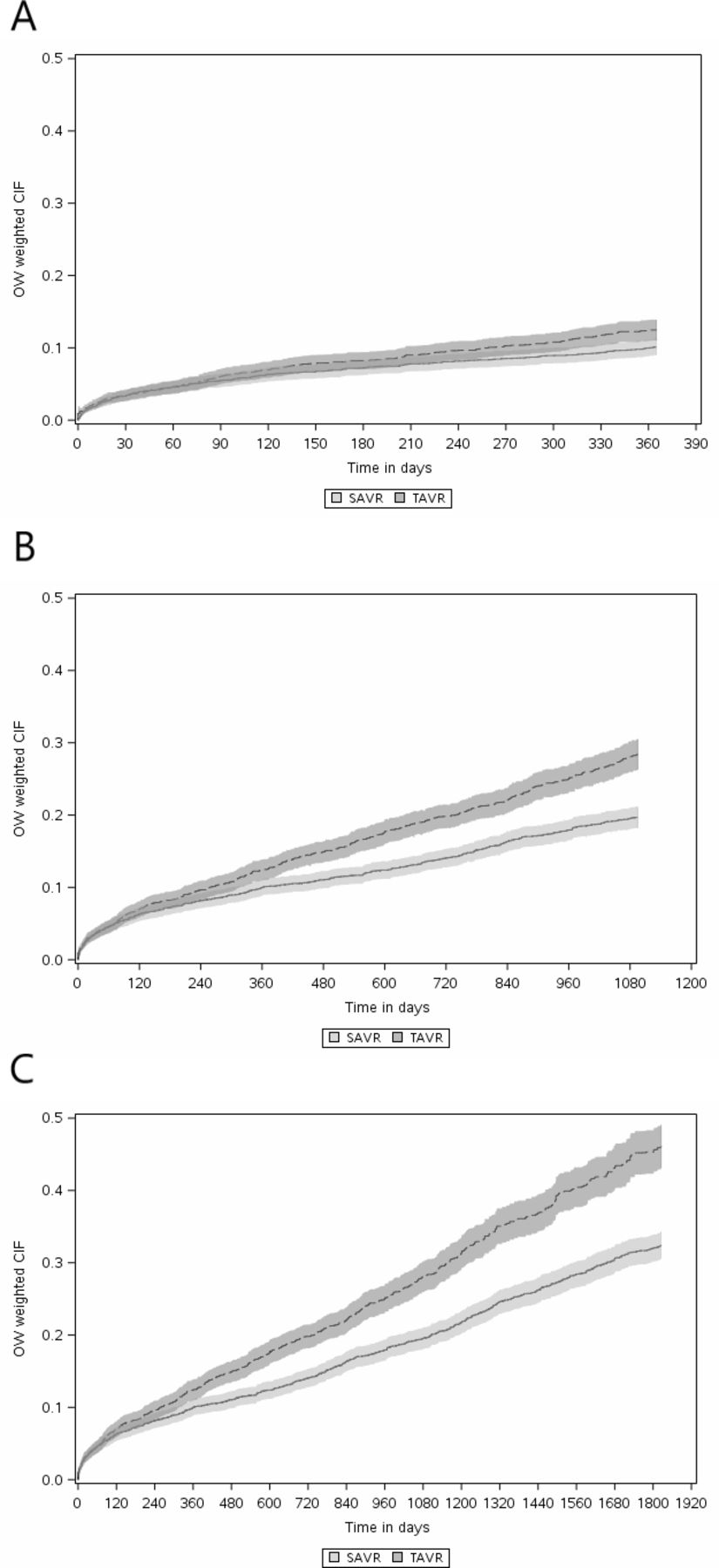
Results for primary outcomes (including in-hospital mortality) are presented in table 3 and figure 1. Rates and hazards of all-cause mortality at 1 year (14.69% vs 5.40%; HR 1.21; 95% CI 1.02 to 1.43), 3 years (27.68% vs 9.96%; HR 1.45; 95% CI1.28 to 1.64) and 5 years (34.27% vs 14.70%; HR 1.48; 95% CI 1.33 to 1.65) were significantly higher in the TAVR compared with SAVR group. Rates and hazards of non-cardiovascular death at 1 year (6.85% vs 2.26%; HR 1.39; 95% CI 1.09 to 1.79), 3 years (14.16% vs 5.22%; HR 1.48; 95% CI 1.24 to 1.75) and 5 years (18.44% vs 8.32%; HR 1.48; 95% CI 1.28 to 1.72) were also significantly higher in the TAVR group. Although in the base model, no significant differences in the rate or hazard of cardiovascular death were observed for TAVR versus SAVR at 1 year, the rates and hazards of cardiovascular death were significantly higher in the TAVR group at both 3 (13.52% vs 4.75%; HR 1.42; 95% CI 1.18 to 1.70) and 5 years (15.83% vs 6.38%; HR 1.49; 95% CI 1.26 to 1.75). Long-term hazards of primary outcomes occurring from date of discharge to 1, 3 and 5 years showed similar results and are presented in online supplemental table 2.
{kind=link}
(A) Cumulative incidence functions (CIF) for all-cause mortality at 1 year. (B) CIF for all-cause mortality at 3 years. (C) CIFs for all-cause mortality at 5 years. SAVR, surgical aortic valve replacement; TAVR, transcatheter aortic valve replacement.
Secondary outcomes
Results of secondary outcomes (evaluated postdischarge) are presented in table 4. Hazards of myocardial infarction were significantly greater in the TAVR compared with SAVR group at 1 year (HR 1.77; 95% CI 1.26 to 2.50), 3 years (HR 1.92; 95% CI 1.51 to 2.43) and 5 years (HR 1.96; 95% CI 1.58 to 2.42) and hazards of readmission due to angina were also significantly higher in the TAVR group at 1 year (HR 1.93; 95% CI 1.21 to 3.10), 3 years (HR 1.86; 95% CI 1.37 to 2.54) and 5 years (HR 1.86; 95% CI 1.39 to 2.48). Notably, hazards for all cause readmission were significantly lower in the TAVR compared with SAVR group (HR 0.89; 95% CI 0.82 to 0.95) at 1 year, but similar at 3 and 5 years. No differences in ischaemic stroke, haemorrhagic stroke, atrial fibrillation, endocarditis, reintervention, valve complications, acute kidney injury, permanent pacemaker implantation and defibrillator were observed with TAVR versus SAVR.
Secondary end points at 1, 3 and 5 years
Sensitivity analyses
Results of sensitivity analyses assessing the impact of potential confounding due to an increase in use of TAVR over the study period and medication usage are presented in online supplemental table 3. While primary analyses showed that cardiovascular mortality and reintervention were not significantly different for TAVR versus SAVR at 1 year, these estimates became significant showing greater mortality and reintervention rates associated with TAVR at 1 year when adding index fiscal year to the calculation of weights. However, treatment effects remained unchanged when adding a binary variable of new onset of cardiovascular medications during follow-up to the calculation of weights.
Discussion
In this retrospective population-based observational cohort of all patients who underwent a SAVR or TAVR between 2007 and 2016, we showed that, in overlap weighted propensity matched patients with similar baseline characteristics, early (in-hospital) all-cause mortality did not differ significantly between those undergoing TAVR versus SAVR, but in-hospital complications markedly differed. TAVR was associated with higher rates and likelihood of in-hospital pacemaker implantation, but a lower likelihood of in-hospital endocarditis and atrial fibrillation than SAVR. TAVR was also associated with greater hazards of long-term all-cause, cardiac and non-cardiac mortality than SAVR and was associated with a higher long-term hazard of myocardial infarction and admission due to angina than SAVR. Hazard of all-cause readmission was significantly lower in the TAVR group at 1 year but not thereafter.
In contrast to our findings of excess mortality associated with TAVR, all prior RCTs have shown that TAVR was non-inferior or superior to SAVR irrespective of the surgical risk-score category (high, intermediate and low).6–9 27 As illustrative examples, the CoreValve trial of 797 high-risk patients27 reported a 20.1% relative reduction in the rate of all-cause mortality or stroke at 3 years in TAVR patients compared with SAVR patients, and the NOTION trial demonstrated no statistical difference for all-cause death, stroke or myocardial infarction at 5 years14 and 8 years15 in 280 lower-risk patients undergoing TAVR or SAVR. Several factors may contribute to the differences between our study and these RCTs. First, strict eligibility criteria in RCTs may limit the generalisability of their findings to more real-world cohorts, such as the one used in the present study. For example, the NOTION trial14 excluded almost 80% of patients who needed acute treatment and those with severe coronary artery disease, severe non-aortic valvular disease, prior heart surgery, recent stroke or myocardial infarction, and severe lung or renal disease. A recent report13 showing that that approximately 50% of low-risk patients who underwent a SAVR at a single-centre exhibited at least one exclusion criteria of the PARTNER 3 study.28
It is also important to note that our results are consistent with several other studies and reports. In a meta-analysis17 of six RCTs, TAVR was associated with poorer survival after 40 months (HR 1.31; 95% CI 1.01 to 1.68), suggesting that survival advantages shown for TAVR in prior RCTs may be limited to the first few years postprocedure and that long-term outcomes may favour SAVR over TAVR. These trends may be due to the fact that the most vulnerable patients died earlier after the intervention with SAVR, or that more complete coronary artery revascularisation occurred more often during SAVR than TAVR. A landmark analysis of the PARTNER Trial16 from 2 to 5 years also demonstrated an increased hazards of all-cause mortality in TAVR compared with SAVR (HR 1.23; 95% CI 1.00 to 1.52). In PARTNER 3,7 although the primary endpoint remained significantly lower with TAVR versus SAVR, the initial differences in death and stroke was no longer different at 2 years. In another meta-analysis18 of 14 comparative observational studies with propensity-score analytical approaches, TAVR mortality was also significantly greater at ≥3 years (HR 1.54; 95% CI 1.31 to 1.81). Similar findings with worse outcomes at 5 years with SAVR compared with TAVR were reported in the OBSERVENT study29 and in the German Gary registry.30 Therefore, our results add to the growing evidence that TAVR may not be as beneficial in real-world settings compared with RCTs. However, as both cardiovascular and non-cardiovascular mortality were significantly increased for TAVR versus SAVR in the present analysis, we also cannot rule out the fact that residual or unmeasured confounding contributed to these findings. Although we balanced our cohort on multiple indicating factors in the overlap weights (see table 1), accounted for competing risks in our analytical strategy, and performed several sensitivity analyses, our findings indicate that TAVR patients in this real-world cohort died more overall, and not just due to cardiovascular causes, suggesting that some source of unmeasured confounding might still be present in this observational context.
Although prior RCTs have shown comparable rates of adverse cardiac outcomes after TAVR versus SAVR within 1 or 2 years,31 our study showed that in a real-world population with severe AS, transfemoral TAVR was associated with higher long-term hazards of myocardial infarction and angina readmission at 5 years. More complete coronary artery revascularisation is often achieved with SAVR and may at least partially explain these findings. The findings suggest that the long-term benefits of TAVR may be influenced by a greater incidence of adverse cardiac events, highlighting the need for careful selection of patients who are most likely to benefit from a TAVR procedure.32 In a recent systematic review and meta-analysis,33 different frailty indices were predictive of mortality at 1 year after TAVR, suggesting that frailty might be an important factor for patient selection. Notably, in the recent FRAILTY-AVR study,34 although frailty was found to be a risk factor for death and disability following both TAVR and SAVR, depending on the specific frailty index used, the prevalence of frailty ranged from 26% to 68%, with the Essential Frailty Toolset showing the strongest predictive utility for death and disability. In the present study, frailty was measured using the Hospital Frailty Risk Score,24 which although previously validated, may not represent the best index for patient selection for TAVR and SAVR and may thus also be a source of potential residual confounding. Future studies evaluating the optimal frailty assessment tool for these patients are required.
Strengths and limitations
Our study has several unique strengths. Drawing on data from linked administrative data, our study captured all eligible patients undergoing TAVR or SAVR in Ontario, Canada over a 12-year observation period (2007–2016). Without inclusion and exclusion criteria regarding patient risk and comorbidities, results of the present study are more generalisable to the general population of individuals indicated for these interventions. Our study also captured multiple outcomes for up to 5 years, providing essential information on the long-term safety and effectiveness of TAVR compared with SAVR and addressing, at least partially, several gaps related to long-term complications of these procedures. Notably, while most published observational studies with a propensity score matching used the inverse probability weighting method, our study used overlap weighting to address the potential for confounding by indication, which did not require us to exclude subjects with extreme propensity scores and was able to effectively balance baseline factors across the population with the most overlap in observed characteristics between TAVR and SAVR.21 22
Despite these strengths, our study is subject to several limitations. First, as indicated, due to the observational nature of this study, it may be subject to residual or unmeasured confounding, such as surgical risk (the Society of Thoracic Surgeons score or the European System for Cardiac Operative Risk Evaluation), which was not available for the present analysis. As TAVR is more likely to be performed in patients who had high surgical risk score or who were inoperable, the increased mortality may be related to surgical risk scores instead of the procedure. Further, overlap weights did also not include several physiological factors including, left ventricular ejection fraction, valve anatomy, pulmonary artery pressure, which were unavailable in these data. Second, improvement of expertise and technology occurred all along the study period, such as the first generation TAVR devices (Edwards Sapien XT, Medtronic CoreValve) used in early years and the second generation devices (Edwards Sapien 3, Medtronic Evolut R) used in the later study period, and have been shown to be associated with a marked decrease in mortality and morbidity.10 15 However, accounting for study period did not change the results in our sensitivity analysis. Nevertheless, based on our period of observation (2007–2016) it is likely that TAVR was mainly performed in high and intermediate risk patients. Third, with limited data on paravalvular aortic regurgitation and new onset left bundle branch block, our study did not examine or compare these important adverse events between the two groups. These adverse outcomes may provide mechanistic information on factors leading to worse clinical outcomes in the TAVR group. Finally, although our sensitivity analyses examined the effect of the initiation of cardiovascular medications over follow-up, we were limited to the binary classification of this variable and were unable to account for the potential time-varying nature of follow-up medication usage.
Conclusions
This study used the overlap propensity score method to compare in-hospital and long-term outcomes of TAVR versus SAVR in a large, real-world 2007–2016 cohort in Ontario, Canada. Our results suggest that compared with SAVR, TAVR patients experienced a higher risk of all-cause, mortality at 1, 3 and 5 years and higher hazards of myocardial infarction and angina readmission at 5 years. Both cardiovascular and non-cardiovascular mortality rates were increased, and we cannot exclude that residual or unmeasured confounding due to frailty, surgical risk or other physiological factors might have contributed to these findings. More studies in the recent era and with long-term follow-up are clearly needed to confirm the long-term clinical benefits of TAVR in real life and to improve patients’ selection.
Data availability statement
Data are available on reasonable request. The dataset from this study is held securely in coded form at ICES. While legal data sharing agreements between ICES and data providers prohibit ICES from making the data set publicly available, access may be granted to those who meet prespecified criteria for confidential access, available at www.ices.on.ca/DAS. The full data set creation plan and underlying analytic code are available from the authors upon request, understanding that the computer programs may rely upon coding templates or macros that are unique to ICES.
Ethics statements
Patient consent for publication
Ethics approval
Projects that use data collected by ICES under section 45 of PHIPA, and use no other data, are exempt from REB review. The use of the data in this project is authorised under section 45 and approved by ICES’ Privacy and Legal Office.
Acknowledgments
We thank IQVIA Solutions Canada for use of their Drug Information File. Parts of this material are based on data and/or information from the Canadian Drug Product Database and Data Extract, compiled and provided by Health Canada, and used by ICES with the permission of the Minister of Health Canada, 2017 (https://www.canada.ca/en/health-canada/services/drugs-health-products/drug-products/drug-product-database.html).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
DM-Z and JE are joint senior authors.
DM-Z and JE contributed equally.
Contributors All authors developed the study question. WP collected data. WP and ZL analysed data. ZL, DM-Z and JE interpreted the results. ZL drafted the manuscript, and all authors revised the manuscript. DM-Z and JE are responsible for the overall content as the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests DM-Z is consultant and received unrestricted research grant from Edward Lifesciences.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.