Article Text

Abstract
Objective Postprocedural ischaemic and bleeding risks after transcatheter aortic valve replacement (TAVR) remain a major concern. Nevertheless, no reliable risk models incorporating both possibilities are currently available. We aimed to assess the accuracy of percutaneous coronary intervention (PCI)-derived models and the performance of a recalibrated model that included variables more applicable to TAVR.
Methods This study included 26 869 patients who had been enrolled in a national registry. Ischaemic events were defined as myocardial infarction, stroke, transient ischaemic attack or peripheral embolism at 1 year. Bleeding events were defined as any bleeding based on the Valve Academic Research Consortium-2 consensus document at 1 year. Patterns of Non-adherence to Anti-Platelet Regimen in Stented Patients (PARIS) and Coronary Revascularisation Demonstrating Outcome Study in Kyoto (CREDO-Kyoto) integer scoring systems were tested. The models were recalibrated by applying new variables using the Fine and Gray method.
Results The 1-year cumulative incidences for ischaemic and bleeding events were 2.7% and 3.1%. Patients with high PARIS and CREDO-Kyoto risk scores had higher incidences of both ischaemic (3.3% vs 2.4% vs 2.4%, p<0.001 and 2.8% vs 2.0% vs 0.8%, p<0.001) and bleeding events (3.3% vs 2.5% vs 0.8%, p<0.001 and 3.7% vs 3.0% vs 2.4%, p<0.001) when compared with intermediate and low-risk patients. The receiver operating characteristic area under the curves for these models were 0.53, 0.58, 0.56 and 0.55, respectively. After the models were recalibrated to incorporate variables more applicable to TAVR, the performance of ischaemic and bleeding models modestly improved (0.58 and 0.61, respectively).
Conclusions The PCI-derived models demonstrated modest accuracy but was inadequate for risk stratification of TAVR patients at 1-year follow-up.
Trial registration number 3395.
- aortic valve stenosis
- cardiac catheterization
- translational medical research
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study. Deidentified data from this study will not be shared.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Ischaemic and bleeding complications after transcatheter aortic valve replacement (TAVR) remain a major issue, known to impair patient survival. Although TAVR risk scoring systems have already been developed, they have focused predominantly on periprocedural bleeding events.
WHAT THIS STUDY ADDS
High Patterns of Non-adherence to Anti-Platelet Regimen in Stented Patients (PARIS) and Coronary Revascularisation Demonstrating Outcome Study in Kyoto (CREDO-Kyoto) risk score patients who received TAVR had experienced significantly more ischaemic and bleeding events. However, these models demonstrated low accuracy in stratifying ischaemic and bleeding events. The recalibrated model including PARIS and CREDO-Kyoto scoring model variables improved performance but remained at a modest accuracy.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Special attention should be paid to patients with the variables of ischaemic and bleeding risks. Further efforts are needed to enhance risk stratification of patients with TAVR in order to strengthen prognosis and avoid major detrimental events.
Introduction
Transcatheter aortic valve replacement (TAVR) is an established treatment for severe aortic stenosis (AS), and current guidelines recommended for a primary option particularly for elderly and comorbid population.1 2 Since its introduction, the number of patients undergoing TAVR has been increasing, and it is estimated that 240 000 and 26 000 TAVR procedures were performed in the USA and Japan, respectively, by the end of 2019.3 However, despite the improvement of technical procedures and patient management, ischaemic and bleeding complications after TAVR remain a major issue, known to impair patient survival.4 5
Precise risk assessment that incorporates the possibility of both events has become an essential part of the preprocedural assessment process. To date, various ischaemic and bleeding risk algorithms have been proposed for patients undergoing percutaneous coronary intervention (PCI), some of which are well validated.6–8 Validated risk models have enabled better clinical decision-making in the prevention of ischaemic and bleeding events.9
This study was designed to assess the accuracy of PCI-derived models and the performance of a recalibrated model that included variables more applicable to TAVR for 1-year ischaemic and bleeding outcomes. Although TAVR risk scoring systems have already been developed,10 they have focused predominantly on periprocedural bleeding events. Since 2013, the Japanese Transcatheter Valve Therapy (J-TVT) registry has collected data from patients undergoing TAVR. Unlike European patients undergoing TAVR, this study sample has unique characteristics such as small body mass index and body surface area (BSA). This data are used to compare variables with the Transcatheter Valvular Therapy registry in the USA, providing a unique opportunity to test the above objective.
Methods
Study design and samples
The J-TVT Registry was established by four academic societies (Japanese Circulation Society, The Society of Japanese Cardiovascular Surgery, Japanese Association for Thoracic Surgery and Japanese Association of Cardiovascular Intervention and Therapeutics) in collaboration with the Pharmaceuticals and Medical Devices Agency to develop a TAVR procedure database in Japan. Data collection began in September 2013 after the TAVR procedure was approved. Consecutive case registration is required for certification of the institutions and operators, and complete case registration is confirmed every 3 years for certification renewal. Data quality is ensured via an automatic system validation, reporting of data completeness, training of site data managers and data auditing, which is overseen by members of the J-TVT Registry Committee. The conduct of the study was approved by the Institutional Review Board of the Osaka University Graduate School of Medicine (Osaka, Japan) as well as National Clinical Database. This study was conducted in accordance with the provisions of the Declaration of Helsinki and the ethical guidelines for epidemiological studies in Japan.
We included all patients who underwent TAVR from September 2013 to December 2019 in Japan. Cases from institutions that performed less than 20 cases annually were excluded to preclude the influence of outliers when modelling site variability. The study population included 25 819 patients. Those excluded comprised 629 patients (2.3%) treated for non-AS, 80 patients (0.3%) without information on age and 341 patients (1.3%) with only periprocedural follow-up data. The assessment of scoring models was performed excluding 199 patients (0.7%) who lacked one or more components of the Patterns of Non-adherence to Anti-Platelet Regimen in Stented Patients (PARIS) or Coronary Revascularisation Demonstrating Outcome Study in Kyoto (CREDO-Kyoto) risk scoring models (figure 1). The PARIS and CREDO-Kyoto scores were developed from Western and Japanese patients undergoing PCI to individually assess ischaemic and bleeding risks. The PARIS score was externally validated using 2 years of thrombotic and bleeding events data from the Assessment of Dual Antiplatelet Therapy with Drug-eluting Stents registry.11 The CREDO-Kyoto score was externally validated based on 3 years of thrombotic and bleeding events data from the Randomised Evaluation of Sirolimus-Eluting vs Everolimus-Eluting Stent Trial and the Nobori Biolimus-Eluting versus Xience/Promus Everolimus-Eluting Stent Trial.12 13 Both scoring models have moderate levels of discrimination and are generally used to predict the risks of ischaemic and bleeding events of patients undergoing PCI.
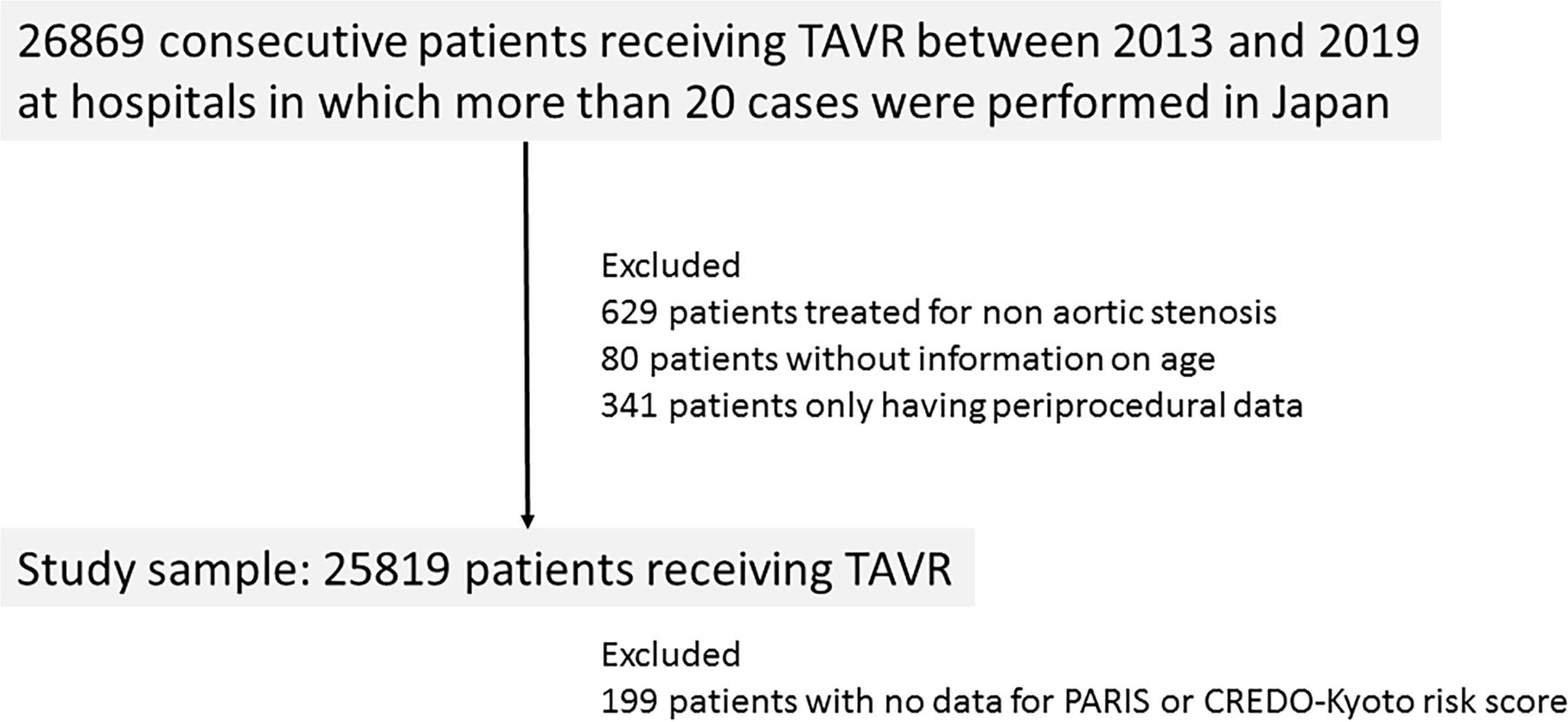
Study flowchart. CREDO-Kyoto, Coronary Revascularisation Demonstrating Outcome Study in Kyoto; PARIS, Patterns of Non-adherence to Anti-Platelet Regimen in Stented Patients; TAVR, transcatheter aortic valve implantation.
In the present study, ischaemic and bleeding risk scores were estimated based on the PARIS and CREDO-Kyoto risk score models. Exclusion criteria included clinical presentation of acute coronary syndrome and existence of a chronic total occlusion lesion, as these variables were not applicable to the study population (online supplemental figure 1). Patients with severe chronic kidney disease (CKD) were defined as those who required maintenance dialysis or with an estimated glomerular filtration rate of <30 mL/min per 1.73 m2, determined by serum creatinine levels using the Cockcroft-Gault equation. Patients with haemoglobin levels of <12 g/dL (men) and <11 g/dL (women) were defined as anaemic for PARIS risk scoring and <11 g/dL (men and women) for CREDO-Kyoto risk scoring. We categorised the patients into three risk groups (low, intermediate and high) based on the threshold value reported in the registry data.6 7 Moreover, HAS-BLED and CHA2DS2-VASc scoring systems were also assessed as post hoc analyses.14 15 HAS-BLED is a scoring system to assess 1-year risk of major bleeding using 7 components; hypertension, abnormal renal and liver function, prior stroke, prior bleeding, labile INR, elderly, and drug usage such as antiplatelet agents. CHADS2-VASc is also a scoring system to assess annual risk of stroke using 7 components; congestive heart failure, hypertension, elderly, diabetes mellitus, prior stroke, vascular disease, and female. In this study, the presence or absence of liver disease to assess HAS-BLED scoring could not be confirmed due to insufficient data.
Supplemental material
Clinical outcomes
Primary ischaemic events were defined as myocardial infarction, stroke, transient ischaemic attack and peripheral embolism within 1 year of the procedure. Myocardial infarction, stroke and transient ischaemic attack were defined based on the Valve Academic Research Consortium-2 (VARC-2) consensus document.16 A peripheral embolism was defined as a suspected thrombotic embolism. Contrast-enhanced CT confirmation was not required for the identification of valve-related thrombosis. A primary bleeding event was defined as any bleeding based on the VARC-2 consensus document within 1 year of the procedure, including life-threatening or disabling, major or minor bleeding. Major bleeding was defined as any overt bleeding that resulted in a drop in haemoglobin level of 3.0 g/dL or greater, required transfusion or caused hospitalisation or permanent injury, or required surgery. A periprocedural drop in haemoglobin level above 3.0 g/dL was excluded except for overt bleeding. Minor bleeding was defined as any bleeding clinically deserved mention, such as life threatening, disabling or major bleeding. Those adverse events that require hospitalisation for 1 year after the index procedure were surely recorded. The Society of Thoracic Surgeons (STS) V.2.73 was used for the calculation of STS-predicted risk of mortality.
Statistical analysis
For the unadjusted analyses, continuous variables are presented as mean±SD or as median with IQR. The Wilcoxon rank sum test was used to compare these values between groups. Categorical variables were compared using the χ2 test. The cumulative incidences of bleeding and ischaemic adverse events were estimated for 1 year based on risk score categories. Death was considered as a competing risk factor. Cumulative event incidences were compared across all the risk categories using the Gray’s test. Model discrimination was assessed using the C-statistic, estimated as the area under the time-dependent receiver-operating characteristics curve at 360 days. Multivariable Fine and Gray subdistribution hazard models were constructed to predict the outcomes of the variables included in the CREDO-Kyoto and PARIS score models in a randomly sampled 70% of the cohort. Discrimination of the model was assessed in the rest of the cohort using the C-statistic. All statistical analyses were performed using SAS V.9.4 (SAS Institute, Cary, North Carolina) and R V.4.1.2 (R Core Team 2021, Vienna, Austria). Two-tailed p values of less than 0.05 were considered statistically significant.
Results
Baseline characteristics
The study patients were predominantly elderly (mean age 84 years) and women (68%). The median STS score was 6.0 (4.3–8.8). The femoral artery was the dominant access site (89%) and most patients were treated with balloon-expandable aortic valves (75%). A relatively small aortic valve size was selected for the study due to Asian-specific small physiques.
Patients who experienced ischaemic events within 1 year after the procedure were older and had smaller BSA. There was also a higher prevalence of peripheral vessel disease, CKD, cerebrovascular disease and history of hypertension among these patients when compared with those who did not experience an ischaemic event. Consequently, STS scores were significantly higher in patients who experienced ischaemic events than in those who did not. Additionally, self-expandable valves were more often necessary in patients who experienced ischaemic events. The transfemoral approach was more often performed in patients who had no ischaemic events than in those who did (table 1).
Baseline characteristics in patients with and without 1-year ischaemic or bleeding events
Patients who experienced bleeding events were more often women and had a small BSA. There was also a higher prevalence of CKD, anaemia, previous PCI, atrial fibrillation and history of peripheral vessel disease when compared with those who had no bleeding events. Notably, there was a significantly higher rate of preprocedural aspirin or warfarin use observed in patients with bleeding events. The use of self-expandable valves was similar in patients with and without bleeding events. The transfemoral approach was more often performed in patients without bleeding events than in those with (table 1).
Clinical outcomes according to PARIS and CREDO-Kyoto risk scoring models
The cumulative 1-year incidence rates of bleeding and ischaemic events were 3.1% and 2.5%, respectively (figure 2). The mortality rate was 8.2%. According to PARIS scoring, patients were classified into high, intermediate and low bleeding risk scores as follows: high was ≥8 points (N=20 357, 79.5%), intermediate was from 4 to 7 points (N=4999, 19.5%) and low was ≤3 points (N=264, 1.0%). They were also classified into high, intermediate and low ischaemic risk scores scoring as follows: high was ≥5 points (N=3582, 14.0%), intermediate was from 3 to 4 points (N=8092, 31.6%) and low was ≤2 points (N=13 946, 54.4%). The cumulative incidences of bleeding and ischaemic events over 1 year were significantly different between the three groups (3.3% vs 2.5% vs 0.8%, p<0.001 and 3.3% vs 2.4% vs 2.4%, p<0.001) (figure 3). The receiver operating characteristic area under the curve (ROC-AUC) for bleeding and ischaemic risk scores was 0.56 and 0.54, respectively.
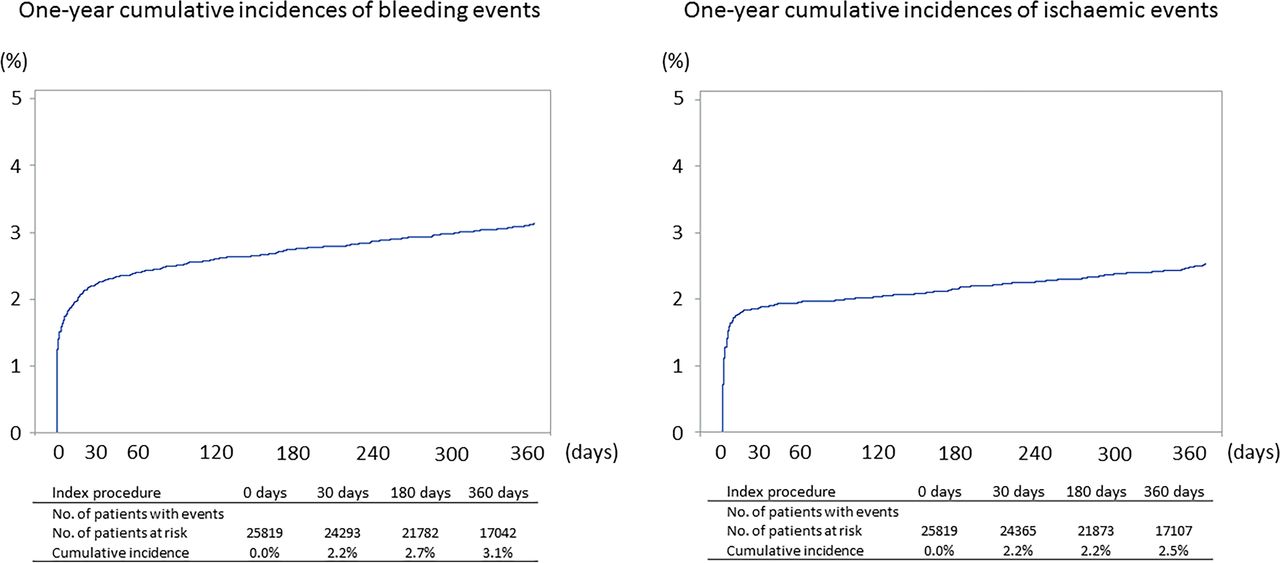
One-year cumulative incidences of bleeding and ischaemic events.
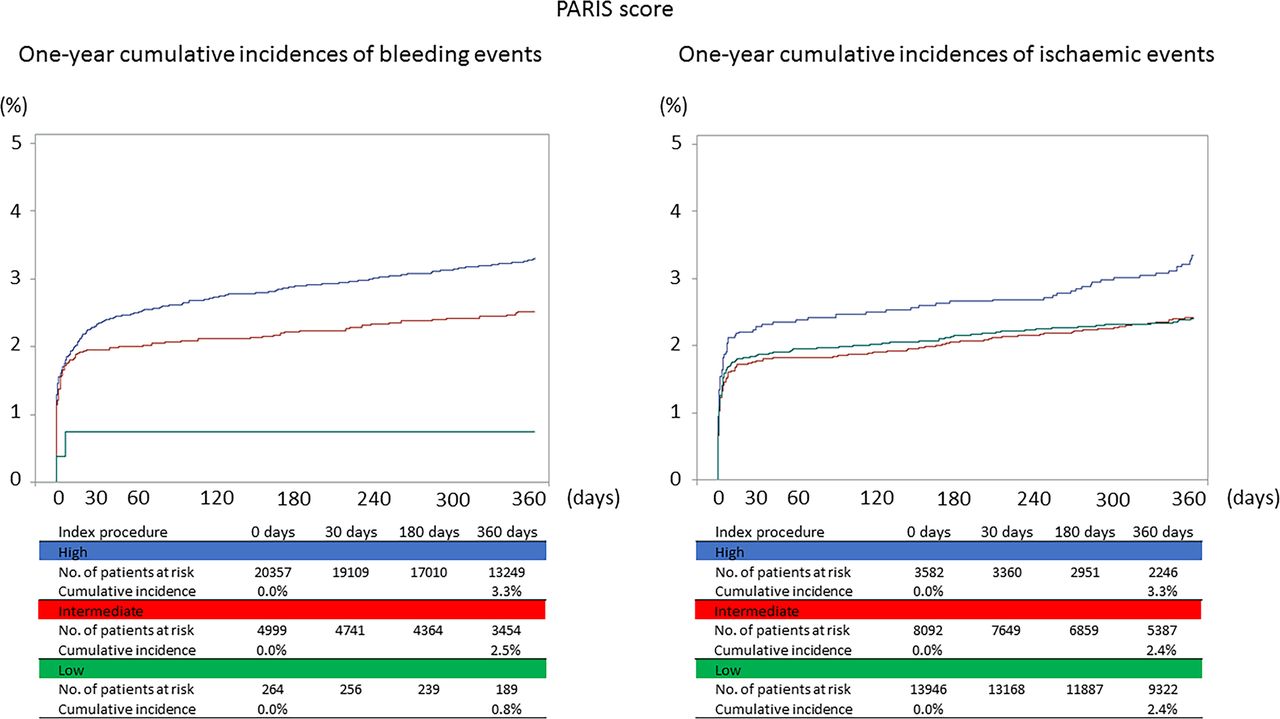
One-year cumulative incidences of bleeding and ischaemic events according to PARIS scoring strata. PARIS, Patterns of Non-adherence to Anti-Platelet Regimen in Stented Patients.
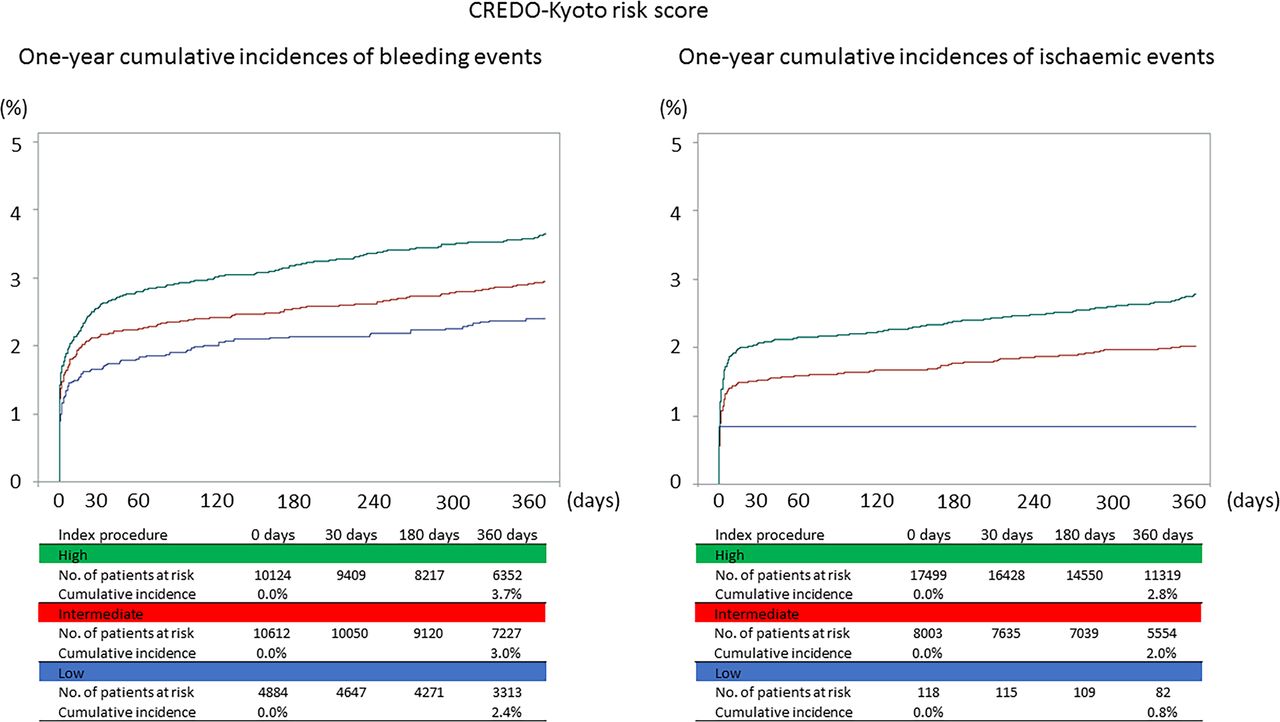
According to CREDO-Kyoto risk scoring, patients were classified into high, intermediate and low bleeding risk scores as follows: high was ≥3 points (N=10 124, 39.5%), intermediate was from 1 to 2 points (N=10 612, 41.4%), and low was 0 points (N=4884, 19.1%). They were also classified into high, intermediate and low ischaemic risk scores as follows: high was ≥3 points (N=17 499, 68.3%), intermediate was from 3 to 4 points (N=8003, 31.2%) and low was ≤2 points (N=118, 0.5%). The 1-year cumulative incidences of bleeding and ischaemic events were significantly different between the three groups (3.7% vs 3.0% vs 2.4%, p<0.001 and 2.8% vs 2.0% vs 0.8%, p<0.001) (figure 4). The ROC-AUC for bleeding and ischaemic risk scores was 0.55 and 0.58, respectively.

One-Year cumulative incidences of bleeding and ischaemic events according to CREDO-Kyoto scoring strata. CREDO-Kyoto, Coronary Revascularisation Demonstrating Outcome Study in Kyoto.
The populations according to HAS-BLED and CHA2DS2-VASc scoring systems are shown in online supplemental file 1. The ROC-AUC of HAS-BLED scoring for bleeding was 0.56 and that of CHA2DS2-VASc scoring for ischaemic events was 0.56.
Recalibrated risk stratification using PARIS and CREDO-Kyoto scoring
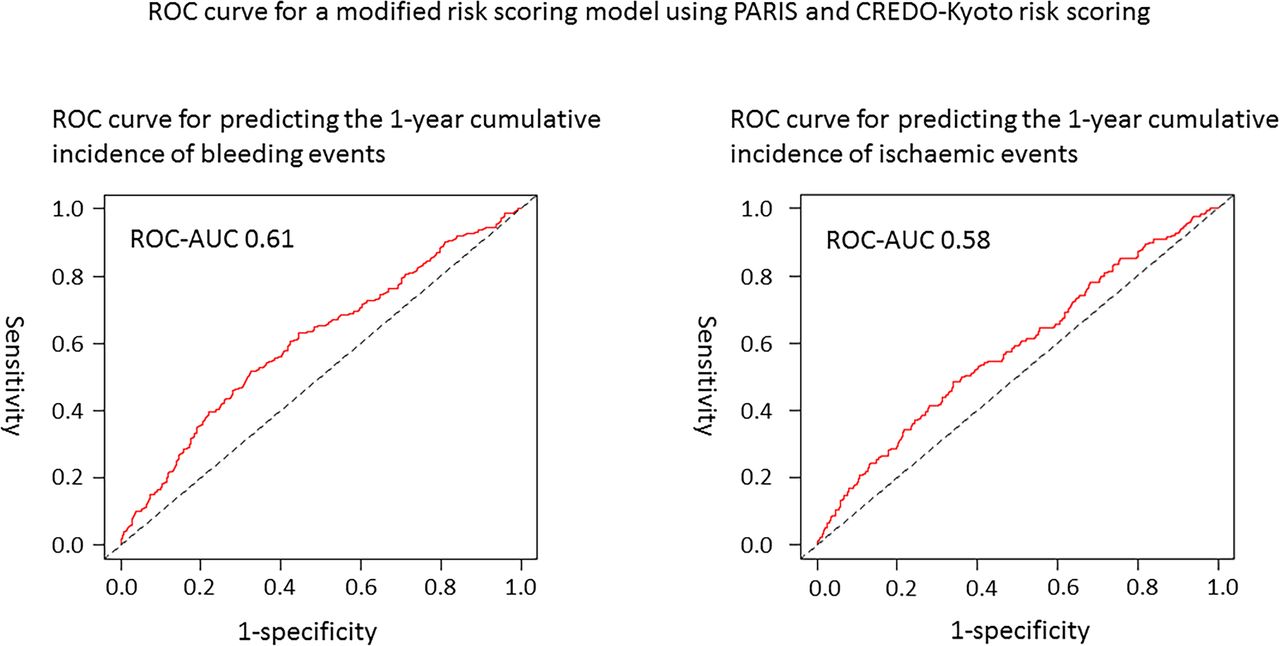
The point estimates and 95% CIs for each variables including PARIS and CREDO-Kyoto scoring models in a recalibrated model are shown in table 2. Peripheral vessel disease was the only independent predictor for bleeding events (adjusted HR 1.42, 95% CI 1.13 to 1.79, p=0.003). Peripheral vessel disease (adjusted HR 2.18, 95% CI 1.73 to 2.73, p<0.001), CKD (adjusted HR 1.56, 95% CI 1.07 to 2.27, p=0.02) and severe CKD (adjusted HR 1.29, 95% CI 1.05 to 1.58, p=0.01) were independent predictors for ischaemic events. The ROC-AUC for the recalibrated model was 0.61 for bleeding events and 0.58 for ischaemic events (figure 5).
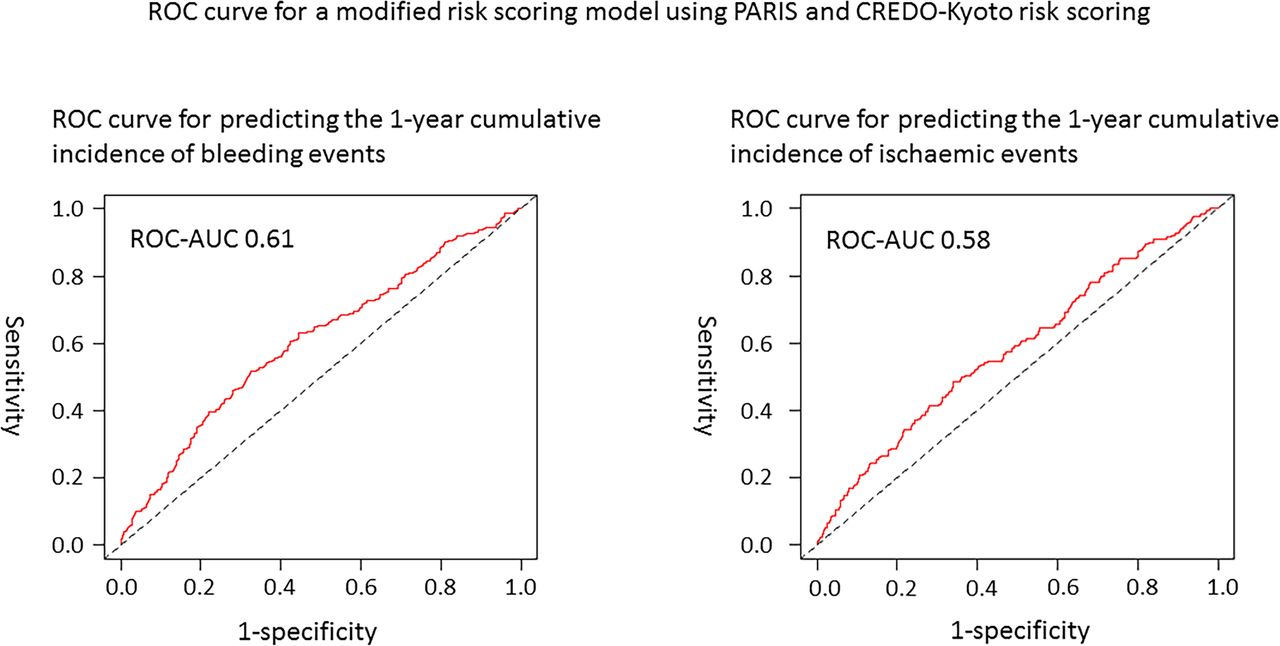
ROC curve for a modified risk scoring model using PARIS and CREDO-Kyoto. AUC, area under curve; CREDO-Kyoto, Coronary Revascularisation Demonstrating Outcome Study in Kyoto; PARIS, Patterns of Non-adherence to Anti-Platelet Regimen in Stented Patients; ROC, receiver operating characteristic.
Independent predictors of ischaemic and bleeding events based on the recalibrated model
Discussion
Primary findings from the nationwide prospective registry were as follows; (1) the cumulative 1-year incidences of bleeding and ischaemic events were 3.1% and 2.5%, respectively; (2) high PCI risk score patients who received TAVR had experienced significantly more ischaemic and bleeding events. However, these models demonstrated low accuracy in stratifying ischaemic and bleeding events. Moreover, PCI risk scoring models allow the identification of patients who are at low risk of bleeding and ischaemic events but cannot be applied to small numbers of patients with TAVR and (3) the recalibrated model including PARIS and CREDO-Kyoto scoring model variables improved performance but remained modestly accurate and inadequate for risk stratification of TAVR patients at 1-year follow-up (figure 6).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Validation of traditional ischaemic and bleeding risk scores in patients with transcatheter aortic valve replacement. AUC, area under curve; AF, atrial fibrillation; BMI, body mass index; CABG, coronary artery bypass grafting; CKD, chronic kidney disease; CHF, congestive heart failure; J-TVT, Japanese Transcatheter Valve Therapy; MI, myocardial infarction; OMI, old myocardial infarction; PCI, percutaneous coronary intervention; PVD, peripheral vessel disease; ROC, receiver operating characteristic; VARC-2, Valve Academic Research Consortium-2.
In the pivotal trials for patients with low or intermediate surgical risks, the incidences of serious bleeding events for 1 year ranged between 3.2% and 15.2%.17–19 Moreover, that was 18.2% in a prospective registry20 and the incidence of bleeding events was low in this study. Bleeding events often include the drop of haemoglobin in the endpoint definition of TAVR trials, but it was not included in this study, because whether it is obvious that bleeding was unknown in this registry data. In fact, the incidence of the in-hospital change in haemoglobin ≥3 g/dL was nearly 15% in this study, although including the obvious bleeding events. Additionally, it was revealed that the transfemoral approach reduced the risk of periprocedural bleeding events by nearly 90% in this study. Those may have contributed to the reduced number of bleeding events.
The incidences of the ischaemic events for 1 year were also low in this study. Stroke after TAVR is the most important ischaemic adverse event, which has substantial impact on morbidity and mortality.4 It has been reported that the incidences of stroke for 1 year ranged between 0.2% and 5.0%.17 19 21 Systemic embolism including thrombotic stroke might be developed by the implanted valve as a consequence of delayed stent frame endothelialisation, tissue failure and changes in haemodynamics through the prosthetic valve. In addition to those embolic events, periprocedural myocardial infarction and delayed coronary obstruction after TAVR have also been recognised potential complication and caused poor prognosis.22 However, the incidences of those ischaemic events were very low particularly between 30 days and 1 year after the procedure, and it was similar to previous reports.17 19 21 It might mean the importance of identifying strong predictors particularly for periprocedural ischaemic events and the focus on avoiding bleeding events.
PARIS and CREDO-Kyoto high bleeding risk score patients accounted for approximately 10% of patients in the studies on PCI, in which nearly half were classified as having a concomitant high thrombotic risk. The registry study samples had high bleeding risk patients accounting for approximately 80% of patients, as defined by the PARIS risk model or 40% when defined by the CREDO-Kyoto risk model (online supplemental figure 3). Patients undergoing TAVR were older with various comorbidities and greater potential risks of bleeding events. However, stratification based on PCI risk scoring had low accuracy. The variables included in the risk scoring models are important factors for predicting bleeding events; however, risk factors for patients with TAVR may be associated with additional comorbid conditions. The incidence of bleeding events was lower in patients who underwent PCI. In fact, bleeding events occurred mainly within 30 days after the procedure, and the Kaplan-Meier curve estimates were equivalent to other TAVR registry data.10 Recent guidelines have recommended postprocedural antithrombotic therapy for patients undergoing TAVR in the form of antiplatelet or anticoagulant drug monotherapy.2 Differences in the participation of antithrombotic therapies among the patients may have influenced the incidence rate of bleeding events. Additionally, a greater number of elderly patients were included in the study when compared with the studies on PCI. Due to their age, they may have died before an ischaemic or bleeding event could have occurred, potentially resulting in lower event rates. Nevertheless, it has been reported that late bleeding events between 30 days and 1 year are associated with mortality.5 23
Only a few components applicable to TAVR, such as diabetes and renal impairment, were included in the PARIS and CREDO-Kyoto risk scores, most of which were discordant. Therefore, we developed a recalibrated model to assess whether performance could be improved. However, the recalibrated model had only modest accuracy. It is well known that peripheral vessel disease and CKD are independent predictors for ischaemic and bleeding events in patients with TAVR.24 25 However, the low event rates in this study made it difficult to create an accurate risk model. Machine learning that uses greater patient sample data may improve the performance of risk-scoring models, but our findings suggest that it is difficult to create a long-term prediction model using preprocedural baseline data alone because patients undergoing TAVR are very old with various comorbidities and their risk factors appear to change in a time-dependent manner after the procedure. Further studies are warranted to improve TAVR-specific tools used for detecting ischaemic and bleeding events and to clarify whether risk score-based decision-making can improve clinical outcomes in larger-scale patient cohorts.
Study limitations
The current study had several important limitations. First, this nationwide prospective registry was conducted on consecutive patients with TAVR but excluded those at institutions who performed less than 20 cases annually. Therefore, a selection bias was potentially present, and treatment strategies were based on each physician’s preference. Second, although the study was based on one of the largest nationwide TAVR registries, the number of bleeding and ischaemic events were small. Third, our study used risk scoring models designed for PCI, meaning some components of the scoring models were inapplicable for TAVR. Therefore, accurate risk scores were not always obtained. Finally, important data for assessing ischaemic and bleeding events, such as postprocedural antithrombotic therapy and history of bleeding events, were not available in this study, particularly, postprocedural antithrombotic therapy, which can affect clinical events. However, this study aimed to assess the association between baseline characteristics and ischaemic and bleeding events within 1 year after the procedure. The actual need for antithrombotic therapy after TAVR and its duration are not well established, and further studies are warranted.
Conclusion
Patients who underwent TAVR with high validated PCI risk scores experienced significantly more ischaemic and/or bleeding events. This model demonstrated only modest performance for stratifying patients in relation to ischaemic and bleeding events, even after model recalibration. Further efforts are needed to enhance risk stratification of patients with TAVR in order to strengthen prognosis and avoid major detrimental events.
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study. Deidentified data from this study will not be shared.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the Institutional Review Board of Kurashiki Central Hospital (Reference number 3395). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We thank the participants in the Japanese Transcatheter Valve Therapy registry.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors MO had full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish. SK revised the manuscript critically for important intellectual content. HK performed all statistical analyses. All authors contributed to conception of the work and made critical revision of the manuscript for key intellectual content.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.