Article Text

Abstract
Objective To identify factors that independently predict the risk of rehospitalisation and death after acute heart failure (AHF) hospital discharge in a real-world setting, considering death without rehospitalisation as a competing event.
Methods Single-centre, retrospective, observational study enrolling 394 patients discharged from an index AHF hospitalisation. Overall survival was evaluated using Kaplan-Meier and Cox regression models. For the risk of rehospitalisation, survival analysis considering competing risks was performed: rehospitalisation was the event of interest, and death without rehospitalisation was the competing event.
Results During the first year after discharge, 131 (33.3%) patients were rehospitalised for AHF and 67 (17.0%) died without being readmitted; the remaining 196 patients (49.7%) lived without further hospitalisations. The 1-year overall survival estimate was 0.71 (SE=0.02). After adjusting for gender, age and left ventricle ejection fraction, the results showed that the risk of death was higher in patients with dementia, higher levels of plasma creatinine (PCr), lower levels of platelet distribution width (PDW) and at Q4 of red cell distribution width (RDW). Multivariable models showed that the risk of rehospitalisation was increased in patients with atrial fibrillation, higher PCr or taking beta-blockers at discharge. Furthermore, the risk of death without AHF rehospitalisation was higher in males, those aged ≥80 years, patients with dementia or RDW at Q4 on admission (compared with Q1). Taking beta-blockers at discharge and having a higher PDW on admission reduced the risk of death without rehospitalisation.
Conclusion When assessing rehospitalisation as a study endpoint, death without rehospitalisation should be considered a competing event in the analyses. Data from this study reveal that patients with atrial fibrillation, renal dysfunction or taking beta-blockers are more likely to be rehospitalised for AHF, while older men with dementia or high RDW are more prone to die without hospital readmission.
- Heart Failure
- Health Services
- Risk Factors
Data availability statement
Data are available on reasonable request. Raw and analysed data underlying this article will be shared on reasonable request to the corresponding author. Any data and materials that can be shared will be released via a Material Transfer Agreement.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Hospitalisation due to acute heart failure (AHF) is the most common reason for hospitalisation in people older than 65 years, with 1-year rehospitalisation occurring in almost half of those patients.
Several risk factors for HF readmissions have been identified, namely being an older patient, having lower systolic blood pressure and estimated glomerular filtration rate, increased heart rate, sedentary lifestyle, depressive symptoms, high number of comorbidities, among others.
WHAT THIS STUDY ADDS
Atrial fibrillation, renal dysfunction and beta-blocker prescription at discharge were identified to be independent risk factors for 1-year rehospitalisation due to AHF.
After an index AHF hospital discharge, the risk of death without rehospitalisation was higher in men, patients ≥80 years of age, with dementia, or with red cell distribution width at Q4 on admission.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The analysis performed in this study allows for the stratification of patients by the identified risk factors for each event separately, granting us the possibility to personalise interventions and make clinical decisions effectively. This knowledge can guide clinicians in establishing the short- and medium-term prognosis of AHF patients discharged from the hospital.
Introduction
Hospitalisation due to acute heart failure (AHF) is a global public health problem of pandemic proportions,1 representing the most common reason for hospitalisation in people older than 65 years in economically developed countries.2 The first year after hospital discharge is a golden period of adverse events, with unacceptably high postdischarge readmission and mortality rates.3 According to the European Society of Cardiology, the 1-year all-cause mortality among AHF patients is 23.6%, while the incidence of the combined outcome of death or HF hospitalisation within 1 year of discharge is 40.1%.4 Several studies have reported that the risk of being readmitted due to HF is higher in older patients, those who fail to comply with treatment, with longer index hospital stay (>7 days), lower systolic blood pressure (SBP) and estimated glomerular filtration rate (eGFR), heart rate over 70 bpm, high presence of comorbidities (such as renal or pulmonary dysfunctions), sedentary lifestyle, depressive symptoms, among others.5–10 Older age, higher levels of blood urea nitrogen and N-terminal pro-B-type natriuretic peptide (NT-proBNP), lower haemoglobin (Hgb) values and not taking a beta-blocker were among the described risk factors for mortality.7 11 However, most of these reports fail to consider competing risks in the data analysis, which may lead to an overestimation of the cumulative incidence and an inaccurate interpretation of data.12
Despite being independent, death and hospitalisation are closely related: death leads to the loss of sicker individuals, those more likely to be hospitalised and hospitalisation is associated with a higher risk of death.13 14 Moreover, after an AHF index hospitalisation, rehospitalisation may be impossible to observe due to a previous occurrence of death, which defines rehospitalisation and death as competing risks, that is, when a certain event prevents the event of interest from happening.12
The use of more specific techniques, such as cumulative incident function or subdistribution function to estimate the probability of each event, and the model introduced by Fine and Gray to test covariates when competing risks are present, ensures that the results can be correctly interpreted. As a result, competing risk analysis has received increasing attention and is becoming more frequently used in clinical studies. This strategy allows to split of the contribution of a covariate from each event type separately and, hence, to gain a better understanding of the disease.15
Using competing risk analyses, this study aimed to identify independent predictive factors for rehospitalisation and death without rehospitalisation among patients with an index admission for AHF, considering rehospitalisation as the event of interest and death without rehospitalisation as the competing event. Additionally, we sought to determine the 1-year overall mortality risk, after an AHF hospitalisation.
Methods
Study sample and clinical setting
This is a retrospective, single-centre and observational study conducted in the Internal Medicine Department of a tertiary university hospital in Portugal. The study design and detailed characterisation of the study population have been described elsewhere.16 Briefly, all patients hospitalised for AHF and discharged between January and December 2012 were considered for enrolment and were followed for up to 1 year after discharge. For the purposes of this study, the first hospitalisation for AHF during the study period was considered the index hospitalisation. Of note, only rehospitalisations due to AHF at the study centre were considered.
Data collection and study outcomes
Hospital discharge summaries, clinical records and telephone interviews were used for data collection, as previously described.16 The main outcomes of this subanalysis were the identification of risk factors for AHF rehospitalisation and death without rehospitalisation in the year following discharge from the index hospitalisation, considering death without rehospitalisation as a competing event.
Statistical methods
Categorical variables are described as absolute frequencies and percentages. Continuous variables are described in terms of mean, standard deviation (SD), median and interquartile range (IQR).
To analyse the overall mortality after discharge from AHF index hospitalisation, standard survival analysis methods were applied, considering death as the event of interest and the time between discharge and death as the follow-up time. Patients alive 1 year after discharge were censored, with a follow-up period of 365 days. Kaplan-Meier curves were obtained for the total sample and according to age groups (<80 years vs ≥80 years). Cox proportional hazards regression models were used to analyse the effect of covariates on the overall mortality after discharge.
To analyse the risk factors for rehospitalisation without bias, survival analysis methods taking competing risks into account were needed, considering rehospitalisation as the event of interest and death without rehospitalisation as the competing event. The follow-up period was considered the time between discharge and the occurrence of the first event (rehospitalisation or death without rehospitalisation). As previously, live patients were censored 1 year after discharge and after a follow-up period of 365 days. The cumulative incidence function (CIF) was estimated as the probability of failing from a given cause in the presence of competing events, given that a subject has survived or has already failed from different causes. Finally, the Fine and Gray model based on the subdistribution hazard function was used to analyse the effect of covariates in the rehospitalisation risk.
In both analyses, an exploratory evaluation was performed to decide which variables should be included in the multivariable models by fitting univariable models and considering all variables significant at the 0.05 significance level as candidates for the multivariable model. The final multivariable models were built, including all variables with p values lower than 0.05, after adjusting for age, gender, left ventricular ejection fraction (LVEF) and the remaining significant variables.
Statistical analysis was performed using SPSS V.26 and R softwares.
Results
Patients’ characteristics
This is a subanalysis of the previously reported population sample from the PRECIC study16, which enrolled 429 patients discharged during the year of 2012 after hospitalisation for AHF. A total of 394 patients were alive at discharge (34 patients suffered intrahospital deaths and one was lost to follow-up) and were considered for this subanalysis (figure 1). Table 1 summarises the baseline characteristics of this study cohort. Briefly, patients’ mean age was 79 years, and most of them were female (61.9%). Importantly, the majority of patients (70.5%) presented an LVEF >40%. At discharge, around half of the patients were prescribed a beta-blocker (52.9%) and an ACE inhibitor (ACEi) or an angiotensin receptor blocker (52.2%).
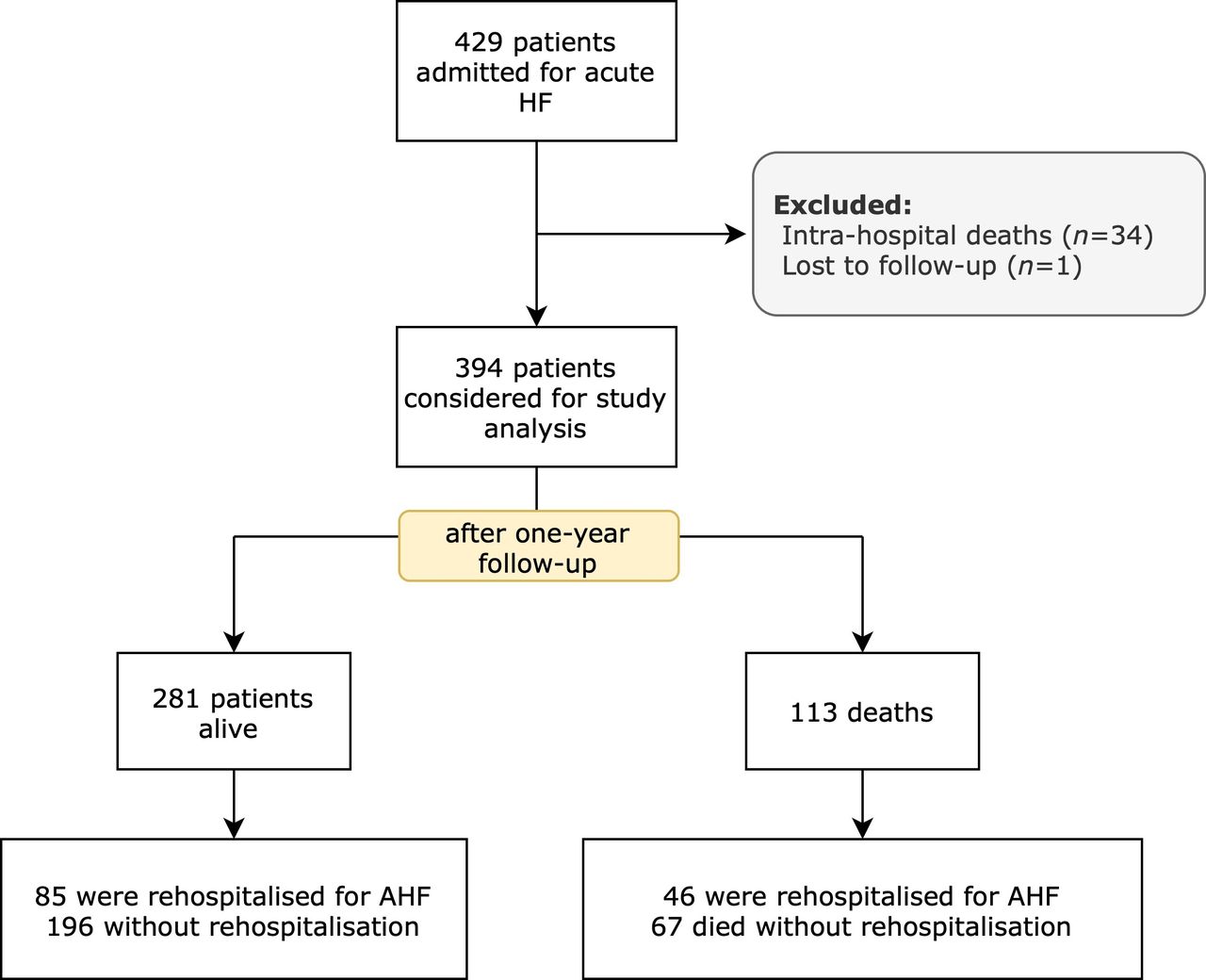
Flow chart of the study population. AHF, acute heart failure; HF, heart failure.
Baseline characteristics of the study cohort
Overall mortality after discharge
One year after discharge, a total of 113 patients (28.7%) were dead, and 281 (71.3%) patients remained alive (figure 1). Figure 2A presents the Kaplan-Meier curve for overall mortality after discharge, for the total sample. Considering that in a previous report, we found that being ≥80 years was a significant predictor for a higher all-cause 1-year mortality risk,17 Kaplan-Meier curves for overall mortality according to different age groups (<80 years vs ≥80 years) are also presented, independently of the occurrence of a rehospitalisation before death (figure 2B). The overall 1-year survival estimate was 0.71 (SE=0.02), being significantly lower (p=0.015, table 2) for patients aged ≥80 years [0.66 (SE=0.03) vs 0.77 (SE=0.03) if <80 years].
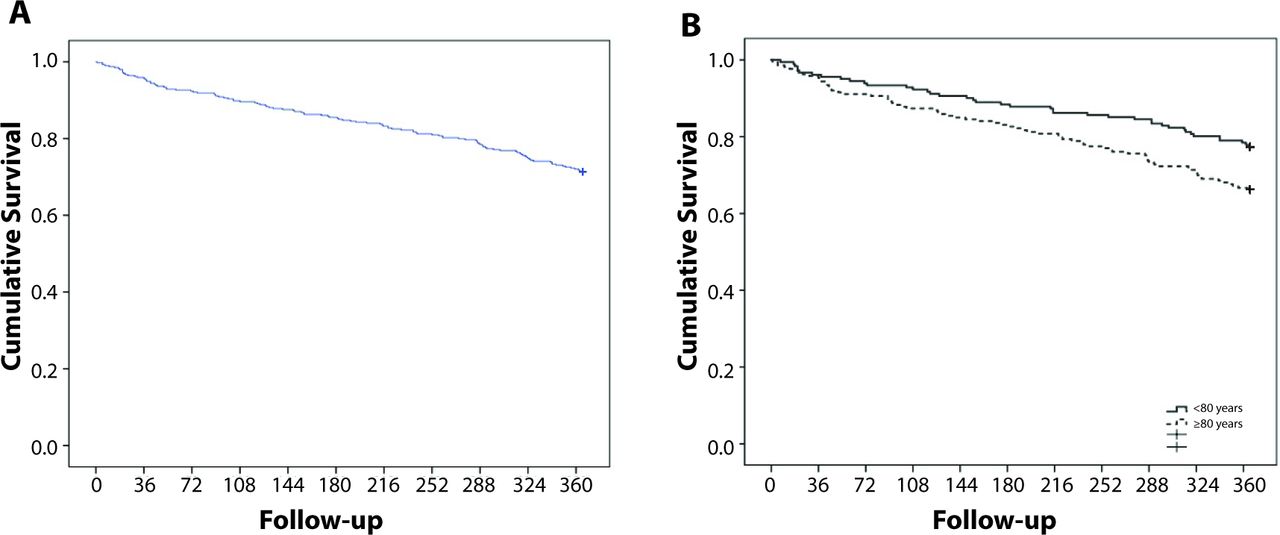
Kaplan-Meier curves for overall mortality after discharge (A) and overall mortality after discharge by age group (B).
Univariable and multivariable Cox model for overall mortality after discharge
Table 2 includes information about the unadjusted and adjusted hazard ratio (HR) and 95% CI for overall mortality after discharge. The factors age, active cancer, dementia, need for caregiving, atrial fibrillation (AF), ACEi, plasma creatinine (PCr), plasma urea (PUr), platelet distribution width (PDW), red cell distribution width (RDW), haematocrit (Htc) and Hgb were identified as potential predictive factors of overall mortality after discharge. After adjusting for gender, age and LVEF, only dementia, PCr, PDW and RDW remained statistically significant. The risk of death was increased in patients with dementia (HR 2.43, 95% CI 1.56 to 3.79), with higher levels of PCr (HR 3.28, 95% CI 2.05 to 5.25), with lower levels of PDW (HR 0.90, 95% CI 0.83 to 0.97), and at the Q4 of the RDW (HR 3.90, 95% CI 2.13 to 7.12).
AHF rehospitalisation after discharge
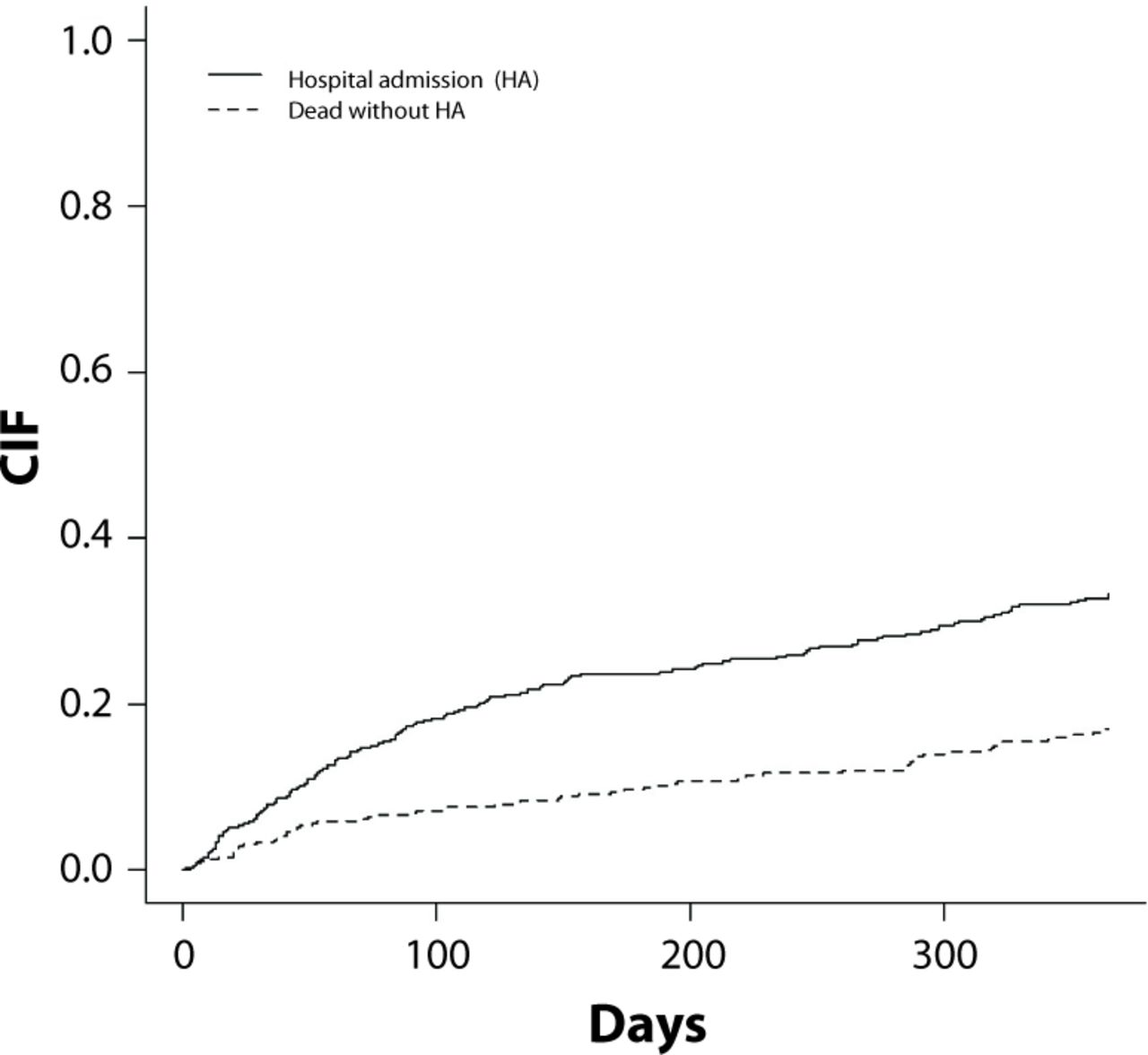
A total of 131 patients (33.3%) experienced rehospitalisation after discharge, and 67 (17.0%) died without being rehospitalised (figure 1). The remaining patients (n=196, 49.7%) were alive 1 year after discharge without any hospital readmission. Figure 3 presents the CIF for all possible events. The probability of rehospitalisation and death without rehospitalisation 1 year after discharge were 0.33 and 0.17, respectively.

{kind=link}
{kind=link}
{kind=link}
Cumulative incident function (CIF) for possible events: rehospitalisation and death without rehospitalisation due to AHF. AHF, acute heart failure.
Table 3 includes information about the unadjusted subdistribution HR (SHR) and 95% CI for all possible events. Hypertension, diabetes, AF, beta-blocker, PCr, PUr, PK+, RDW and Hgb were identified as potential predictive factors of AHF rehospitalisation. Age, LVEF, active cancer, dementia, need for caregiving, ACEi, beta-blocker, PDW, RDW, Htc and Hgb were identified as potential predictive factors of death without rehospitalisation.
Univariable Fine and Gray model for rehospitalisation (event of interest) and death without rehospitalisation (competing event) due to AHF
Table 4 displays the adjusted SHR and 95% CI for all possible events after AHF hospital discharge. Multivariable models, adjusting for age, gender and LVEF, showed that risk of rehospitalisation was increased in patients with AF (SHR=1.58, p=0.020), higher creatinine levels (SHR=2.00, p<0.001) or taking a beta-blocker at discharge (SHR=1.61, p=0.010). The risk of death without rehospitalisation was increased in males (SHR=1.72, p=0.040), those ≥80 years (SHR=1.87, p=0.030), patients with dementia (SHR=2.68, p<0.001) or RDW at Q4 on index admission (compared with the first, SHR=2.54, p=0.030). Taking a beta-blocker at discharge and high PDW levels at admission reduced the risk of death without rehospitalisation due to AHF (SHR=0.55, p=0.040 and SHR=0.89, p=0.009, respectively).
Multivariable Fine and Gray model for the two events: rehospitalisation (event of interest) and death without rehospitalisation (competing event) due to AHF
Discussion
This is a 1-year follow-up study of a cohort of real-world AHF patients who were discharged after an index hospitalisation from an internal medicine department of a tertiary care hospital, in Portugal. Considering that there may be different risk factors for death and rehospitalisation in AHF patients after hospital discharge, the main goal of this study was to identify the independent predictors of rehospitalisation for AHF, considering death as a competing event. In addition, it was sought to determine the risk factors for 1-year overall mortality, independently of the occurrence of a rehospitalisation before death. Of note, our study reports data from a real-world geriatric HF population, predominantly having a LVEF >40%, which is largely underrepresented in clinical trials and cardiology-based registries.
After performing the competing risks analyses, we were able to identify which factors independently contribute to the risk of rehospitalisation 1 year after hospital discharge from AHF in our study population: AF, renal dysfunction or beta-blocker prescription at discharge. In addition, we have identified predictors of death without rehospitalisation: being a male patient, aged ≥80 years, with dementia, and RDW at Q4 on index admission were considered as high-risk factors, while taking beta-blockers at discharge and having higher PDW levels on the index admission were found to be low-risk factors. Interestingly, we have previously reported the predictors of 1-year overall mortality after AHF hospitalisation,17 and identified those having ≥80 years of age, with active cancer, dementia, higher urea, RDW at Q4 and lower PDW levels as being at higher risk of mortality. Consistent with this, we are now reporting that, after adjusting for gender, age and LVEF values, having dementia, RDW at Q4 and lower PDW levels remain as independent risk factors for overall mortality after hospital discharge. Altogether, this knowledge will allow us to stratify patients by risk factors for each event (rehospitalisation or death) separately, at discharge of the index hospitalisation.
Hospital readmission is a key marker of healthcare quality, particularly when assessing AHF patient outcomes. However, despite its widespread use, there is some controversy regarding the statistical methods employed to analyse the risk of rehospitalisation, as these analyses mostly do not consider patients who die before experiencing a readmission event within the period of interest.18 Significantly, it has been estimated that 46% of studies in high-impact medical journals are susceptible to competing for risk bias,19 highlighting the importance of considering death and rehospitalisation separately in the risk analysis of HF patients.
Many pivotal clinical trials included in the pharmaceutical and device development programmes for HF management have tested the benefit of the intervention on the composite primary endpoint of cardiovascular death and HF hospitalisation. However, several researchers have noted that the emphasis on the reduction of 30-day hospitalisation rates may have adverse consequences, such as an increased risk in the 30-day mortality,20 and that risk-adjustment models do not account for the competing risk of mortality.21 In fact, there is one report of increased 30-day and 1-year mortality after the successful implementation of a Hospital Readmissions Reduction Programme when competing risks analyses were used.22
These findings are particularly important considering the characteristics of our study population, a real-world cohort of geriatric patients with multiple comorbidities (having an average of three comorbidities per patient) and with the majority of patients having LVEF >40%.16 We should not neglect that HF is regarded as the cardiovascular syndrome of ageing, resulting from the combination of cardiovascular conditions of older adults with age-related changes in cardiovascular structure and function23, and that the mortality, hospitalisation and rehospitalisation rates are still high in this population.2 24 Therefore, it is of utmost importance to find risk factors for these events in such patients.
AF has been associated with a worse prognosis for patients with chronic HF and is a classical trigger for HF decompensation. Herein, the more advanced age and HF severity of this group of patients justify the finding that AF is associated with a higher risk of rehospitalisation, in line with previous reports.25 In the ESC-HF-LT Registry, the proportion of patients with AF varied widely among clinical profiles, with the highest prevalence of AF (34.7%) documented in patients with right HF. Curiously, this was also the group with the highest 1-year rehospitalisation rate (31.2%),26 in accordance with what was observed in this study.
Other authors have also reported that risk predictors for rehospitalisation are different from those for mortality. For instance, SBP <120 mm Hg at the index hospitalisation predicts mortality, whereas an increase in body weight predicts rehospitalisation.21 Although we included SBP in our risk analysis, it was not identified as an independent predictor of rehospitalisation or death without rehospitalisation.
Renal dysfunction has been recognised as a risk factor for HF rehospitalisation and mortality,25 and our data support this notion. Indeed, a previous report by Álvarez-García et al performed a competing risk analysis for risk prediction in hospitalised HF patients. They used competing risks analysis to develop the Redin-SCORE to predict the 1-month and 1-year risk of rehospitalisation due to HF acute episodes among ambulatory patients.6 Similar to our findings, they found that renal dysfunction, defined as an eGFR below 60 mL/min/1.73m2, among other clinical and laboratory parameters, were predictors of 1-year rehospitalisation.6
Interestingly, we found that higher levels of PCr at the index HF admission are: (1) a risk factor for overall mortality after discharge in the multivariable Cox model and (2) a risk factor for rehospitalisation, but not for death without rehospitalisation, in the competing risk analysis. Of note, this last finding does not weaken the impact of renal dysfunction on mortality, since patients are known to die during and after AHF rehospitalisations, and rehospitalisation for HF is a known risk factor for death.27 In a systematic review of models for predicting mortality and/or hospitalisation in patients with HF, Ouwerkerk et al found that the strongest predictors were blood urea nitrogen and sodium levels.28 Perkins et al have developed a prediction model for rehospitalisation derived from a cohort of 607 chronic kidney disease patients hospitalised for HF; 19.1% were rehospitalised within 30 days.29
In our study, 52.8% of patients had a prescription for a beta-blocker at hospital discharge,16 and this was associated with a higher risk of rehospitalisation and a lower risk of death without rehospitalisation. These are in line with recent evidence from multiple studies reporting that the uptitration of beta-blockers is associated with more HF hospitalisations in patients with a preserved ejection fraction.30 31 Nevertheless, these results need to be addressed, given that the known mortality benefit of this class of drugs in HF patients seems limited to those with LVEF <40% and in sinus rhythm,25 30 whereas our patients had mostly LVEF >40% (70.5%) and AF (51.7%).16 Notably, 75.2% of patients with LVEF <40% were discharged with a beta-blocker,16 following the guidelines in place at the time the study was conducted, and we adjusted the analysis for LVEF. Therefore, we can presume that the higher risk of rehospitalisation is related to the frequent side effects of beta-blockers—negative inotropism, bradycardia and hypotension—and the contribution of these factors to the decompensation of HF patients.25 Recently, Stolfo et al performed a propensity score-matched analysis from the Swedish HF registry focusing on older patients (>80 years) with LVEF <40%, typically underrepresented in randomised control trials.32 The authors concluded that the use of beta-blockers was high for those patients and was strongly associated with improved all-cause and cardiovascular survival.
HF is not only associated with an increased risk of all-cause dementia, as it may represent a risk factor itself for dementia. In a meta-analysis by Cannon et al, the prevalence of cognitive impairment among HF patients was estimated as 43%.33 Adelborg et al reported in a large, nationwide cohort study in Denmark that HF was associated with an approximately 20% risk increase of all-cause dementia among patients surviving at least 1 year after HF diagnosis.34 The possible mechanisms underlying this risk association are chronic cerebral hypoxia secondary to hypoperfusion or cerebral inflammation, and microvascular dysfunction due to neurohormonal HF activation mechanisms.34 Our findings add new information to this interplay between HF and dementia, showing that dementia is: (1) a risk factor for overall mortality after discharge and (2) a risk factor for death without rehospitalisation, but not for rehospitalisation. These findings reinforce the relationship between dementia and death after AHF hospitalisation and prompt further investigation into the death causes of these patients.
The higher RDW level (at Q4; ie, higher than 16.3%) has been previously reported by us in the PRECIC study as an independent predictor of higher 1-year overall mortality risk in HF patients.28 Here, a higher RDW level is again associated with a higher mortality risk, yet in patients discharged from an index hospitalisation. In addition, this association is reinforced by the finding that patients with higher RDW had an increased risk of death without rehospitalisation. Recently, Melchio et al reported that HF patients discharged for AHF with higher RDW (>14.8%) had more comorbidities and were at higher risk of death (HR for death from any cause=1.73).35 The authors have also demonstrated that RDW adds prognostic information beyond that provided by well-established risk factors or biomarkers (eg, age, renal function, NT-proBNP levels, therapy) and is a powerful marker of worse long-term outcomes in AHF patients. Thus, there is a growing body of evidence that RDW can alert clinicians to the risk of death for individual patients in the first few hours of an AHF hospitalisation.
On the opposite, the prognostic impact of PDW, a specific marker of platelet activation, is still not yet well known. In a prospective observational study, which aimed to evaluate the prognostic impact of PDW among AHF hospitalised patients, Sato et al found an association between PDW levels and the prognosis of HF patients36: patients with higher PDW (>16.9) were at higher risk of all-cause death, cardiac death and a cardiac event (HR 1.72, 1.92 and 1.40, respectively).36 In contrast, our results show that patients with lower PDW levels were at higher risk of overall mortality after discharge and death without rehospitalisation, and had no influence on the rehospitalisation incidence levels.
Study limitations
This study has a few limitations that might introduce bias in our conclusions: (1) the rehospitalisation episodes analysed were only those occurring at the study centre, given the difficulty in accessing patient health data in other public or private health organisations, and, because of this, rehospitalisation rates might have been underestimated; (2) due to the retrospective nature of the study, with secondary use of data, signs of congestion and other clinical and laboratory parameters, like NT-proBNP, could not be evaluated as risk factors for readmission or death; it was also not possible to provide a thorough description of the group, including the aetiology of AHF, as well as the NYHA class on admission (3) the implantation of cardiac devices was not examined, although it was unlikely that a significant number of patients had implanted such devices, considering their age and that only a minority had LVEF ≤40%; (4) other factors that could have contributed to rehospitalisation, such as poor compliance to medication, were also not considered in the risk analysis; (5) the causes of death after discharge were not studied in detail, although we have previously reported that 42.9% of patients from the PRECIC study died of cardiovascular causes.16
Conclusions
Predicting the risk of an event of interest is a matter of great relevance in clinical practice. In this study, we aimed to accurately estimate the predictors of AHF rehospitalisation and death in a real cohort of patients after hospital discharge for AHF, considering death without rehospitalisation as a competing event.
Our findings support that AF, renal dysfunction and beta-blocker prescription at discharge are strong predictors of rehospitalisation. When considering the overall risk factors for death without rehospitalisation, we found that being male, ≥80 years of age, having dementia or high RDW levels are considered as high-risk factors, while taking beta-blockers at discharge and having high PDW levels at index admission represent a low risk. If confirmed in more extensive studies, these risk predictors may be used to guide clinicians about the short- and medium-term prognosis of AHF patients on hospital discharge and may help tailor clinical interventions to improve patients’ clinical outcomes.
Data availability statement
Data are available on reasonable request. Raw and analysed data underlying this article will be shared on reasonable request to the corresponding author. Any data and materials that can be shared will be released via a Material Transfer Agreement.
Ethics statements
Patient consent for publication
Acknowledgments
This manuscript was prepared with the medical writing support of Carla Gomes, Duarte Oliveira and Joana Melo from W4Research, financially supported by Novartis Portugal.
References
Footnotes
Contributors IM was the guarantor and responsible for the study design, data acquisition, clinical interpretation, discussion of the results and writing of the first draft; DM and LT were responsible for the statistical analysis and interpretation of data. All authors contributed to the critical review of the manuscript and approved its final version.
Funding Novartis Pharma supported statistics analysis through an unrestricted grant but had no access to the data or any other role in study design, analysis or decision to submit for publication.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.