Article Text

Abstract
Objectives To evaluate bare-metal Optimus and polytetrafluoroethylene (PTFE)-covered Optimus-CVS balloon-expandable, cobalt–chromium, hybrid cell–designed stents in congenital heart disease (CHD) interventions.
Methods Retrospective multicentre review of patients with CHD receiving Optimus stents. Stent mechanical behaviour, clinical indications and outcomes were assessed.
Results 183 stents (49.2% XXL/15-ZIG, 33.3% XL/12-ZIG, 17.5% L/9-ZIG) were implanted (98.9% success rate, 2.3% serious procedural complication rate) in 170 patients (57.6% men, 64.1% adults), median age 23.6 years (IQR, 15.2–39.2) and weight 63.5 kg (IQR, 47–75.7). Indications were right ventricular outflow tract stand-alone stenting or before revalvulation (62.4%), aortic coarctation treatment (15.3%), Fontan-circuit fenestration closure (12.4%) and miscellaneous (10%). 86/170 (50.6%) patients had PTFE-covered stenting (50% prophylactic). In 86/170 (50.6%) patients with stenotic lesions, median percentage of achieved stent expansion was 93.4% (IQR, 85.5%–97.7%), median gradient decreased from 28 mm Hg (IQR, 19–41) to 5 mm Hg (IQR, 1–9) (p<0.001), median vessel diameters increased from 13 mm (IQR, 7.9–17) to 18.9 mm (IQR, 15.2–22) (p<0.001) and percentage of vessel expansion was 45.2% (IQR, 19.8%–91.3%). In 30/36 (83.3%) patients with graft, median dilation of 2 mm (IQR, 2–5) above nominal diameter was achieved. Median stent shortening was 10.9% (IQR, 6.1–15.1) and was associated only with expansion diameter (OR: 0.66, 95% CI: 0.38 to 0.93). No clinically relevant fracture, stent embolisation or dysfunction occurred on a median follow-up of 9 (IQR, 4–14) months.
Conclusions Optimus stents are effective tools for transcatheter treatment of simple and complex CHD. Optimus stents’ reliable mechanical behaviour and particular covering design can promote widespread use.
- congenital heart disease
- cardiac catheterisation
- endovascular procedures
- heart defects, congenital
- outcome assessment, health care
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- congenital heart disease
- cardiac catheterisation
- endovascular procedures
- heart defects, congenital
- outcome assessment, health care
WHAT IS ALREADY KNOWN ON THIS TOPIC
Optimus stents are new promising additions to the armamentarium of congenital heart disease (CHD) interventionists. Data on their clinical application and performance remain limited.
WHAT THIS STUDY ADDS
Optimus stents are safe and effective tools for transcatheter treatment of simple and complex CHD. Reliable mechanical performance was demonstrated with sufficiently high radial strength for stenosis relief and good anchoring properties in extralarge compliant vessels.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Good short-to-midterm outcomes can promote widespread use of Optimus stents in CHD interventions. A formal protocol-driven monitored study is required to evaluate outcomes of Optimus stents in the long run.
Introduction
Stent implantation in congenital heart disease (CHD) has emerged as an alternative to surgery and complementary to balloon angioplasty.1 Encouraging clinical results and improvements in the designs of stents, balloon carriers and delivery sheathes widened the indications.2–4 Given the diversity of lesions and patient size range, several stents were commercially available throughout the past two decades. Each stent offered a combination of specifications and technical advantages.3 4 However, pitfalls are numerous, pushing interventionists to continuously search for the ideal stent.4 5 Optimus and Optimus-CVS (AndraTec, Koblenz, Germany) in bare-metal and polytetrafluoroethylene (PTFE)-covered versions are one of the latest additions to the armamentarium, promising high performance for better patient outcomes. Data on their clinical application and performance remain limited to small series.6–10 Here, we report the largest experience with Optimus stents for the treatment of various congenital cardiovascular defects with a comprehensive focus on indications, stent performance and procedure outcomes.
Patients and methods
Study design
We performed a retrospective multicentre data review of all consecutive patients with CHD who received Optimus stents from June 2020 until June 2022. Approval from the institutional review board was obtained (MR004: 2022-0503161831). Written informed consent was signed by the patients or their legal guardians to perform the procedure and to use their clinical records. Patients were divided into four groups: dysfunctional right ventricular outflow tract (RVOT) stand-alone stenting or prestenting before transcatheter pulmonary valve replacement (TPVR), coarctation of the aorta (CoA) treatment, closure of Fontan-circuit fenestration and miscellaneous. Safety and standard outcomes were evaluated. The prestenting and poststenting vessel diameters were measured in two orthogonal fluoroscopic projections. Target expansion diameters (TED) (ie, delivery balloon diameters) were recorded. Percentage of achieved stent expansion (PASE) and percentage of vessel expansion (PVE) were calculated. Stent lengths after implantation were also measured, and stent length shortening was calculated.
Optimus and Optimus-CVS stents’ characteristics
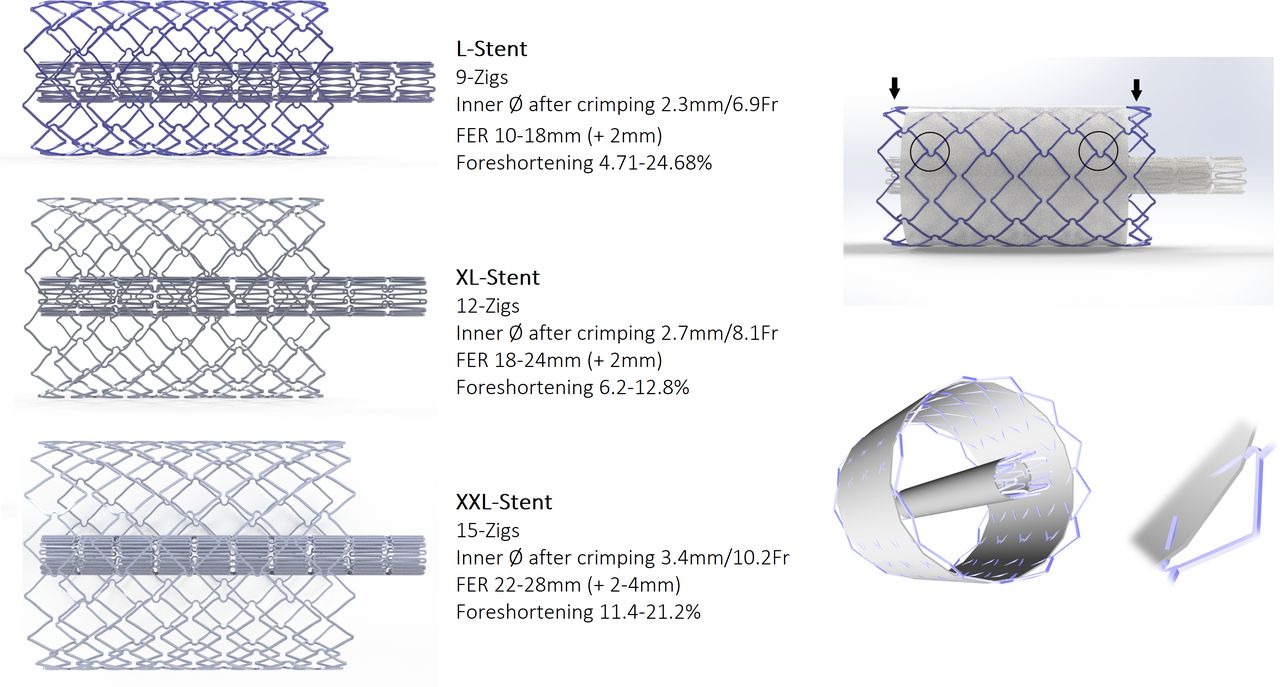
Optimus is a balloon-expandable, non-premounted, cobalt–chromium vascular stent. The Optimus stent has a unique hybrid-cell (semiopen) design with Omega-flex connections between ZIG segments and atraumatic rounded edges (figure 1). This modern stent design offers homogeneous expansion, good stent flexibility and low bench-side foreshortening. Along with this flexibility, the laser-cut cobalt–chromium alloy promises stable vascular anchoring, radial strength and resistance to fracture. The hybrid design facilitates interventions through the open cells. The thickness of struts is 0.22 mm, and the length of the segments is 4.8 mm. Optimus stents are available in three sizes: L/9-ZIG, XL/12-ZIG and XXL/15-ZIG to offer a functional expansion range of 10–18 mm, 18–24 mm and 22–28 mm, respectively (figure 1). The available nine lengths are 13, 18, 23, 28, 33, 38, 43, 48 and 57 mm. The stent length can also be customised for specific procedures.11 Optimus stents are available in bare-metal and PTFE-covered versions. This broad portfolio allows the physician to choose the optimal platform for the target lesion and the clinical needs of the patients. Optimus-CVS offers a secure sandwich covering with thermally bonded inner and outer Nano-PTFE layers and a unique end-free technology with half a row of cells bare-metal at both extremities (figure 1). This particular feature allows wider dilatation ranges without creating an overhang of the PTFE covering. An additional 2-Fr and 3-Fr sizes are required over the introducer size of the balloon carrier for comfortable delivery of bare-metal and covered stents, respectively. Details of the physical behaviour of the stents are provided by the manufacturer on every stent cover. Optimus stents are currently CE-approved in class II-2b for the nine standard lengths.
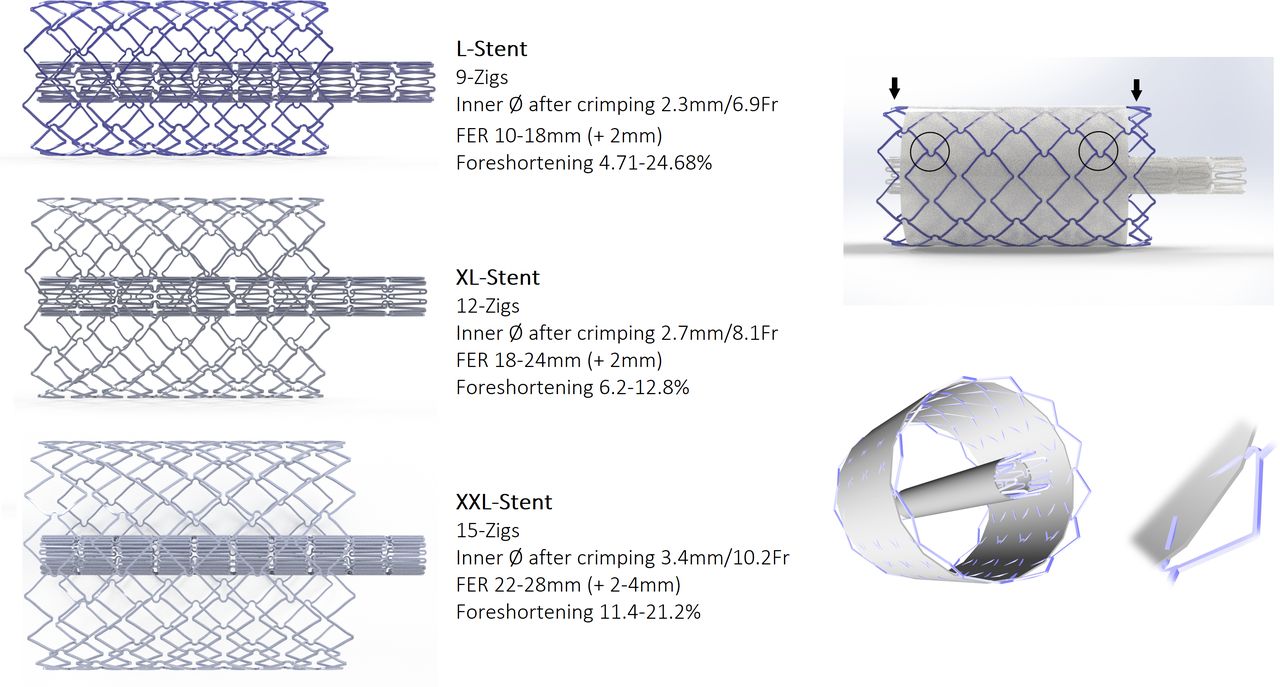
On the right side, three available sizes of Optimus stents in bare-metal versions: L/9-ZIG, XL/12-ZIG and XXL/15-ZIG. On the left side, Optimus-CVS with end-free sandwich e-PTFE covering design. Note one-half of a row of cells remaining bare segments at either end of the stent (black arrows), and the metal struts sandwiched with inner and outer layers of Nano-ePTFE layers. Note the special hybrid cell design with omega-flex connectors (black circles). PTFE, polytetrafluoroethylene.
Interventional procedure
After wire positioning, haemodynamic measurements and angiography, a long sheath of appropriate size was advanced across the lesion. Stent length was chosen according to the lesion to treat. The stents were hand-crimped onto dual or single delivery balloons. Stent implantation was performed as routinely for all types of stenting procedures. Pressure measurements and dimensions were re-evaluated after stent placement. When necessary, the stent was redilated using a larger-diameter or higher-pressure balloon. Indicated TPVRs were planned to be performed immediately after RVOT prestentings during the same procedure. Implantation was considered successful only when the stent was implanted into the correct position uneventfully and the patient was safely discharged.
Follow-up
Patients’ follow-up was performed according to each institutional protocol (clinical examination, ECG and transthoracic echocardiography). General and vascular access complications were recorded.
Statistical analyses
Statistical analyses were performed using SPSS, V.22.0 for Macintosh (IBM, Armonk, New York, USA). Nominal and continuous variables were expressed in count with percentage and median with IQR, respectively. The normality of measurements was assessed using Shapiro-Wilk test. Statistical analysis for continuous variables was conducted using Mann-Whitney U test or Kruskal-Wallis test as appropriate. Bivariate Pearson correlation was used to measure the strength and direction of linear relationships between continuous variables. Univariable and multivariable linear regression analyses were performed to investigate factors associated with stent shortening. A p-value <0.05 was considered statistically significant. All reported p-values are two-sided.
Results
During the study period, 170 patients (64.1% adults) underwent implantation of 183 Optimus stents in seven tertiary centres. Patients’ clinical and procedural characteristics are outlined in table 1. Overall implantation success rate was 98.9%. There were four (2.3%) serious procedural complications (of which two were stent related). Procedural outcomes are detailed in table 2.
Patients’ clinical and procedural characteristics
Procedure outcomes
RVOT stand-alone stenting or prestenting before TPVR group
114/183 (62.3%) stents were deployed in the RVOTs of 106 patients, median age of 28.6 years. Tetralogy of Fallot was the most common underlying diagnosis (64.1%). Patients had patched RVOTs (37.7%), native RVOTs (28.3%), surgical bioprosthetic conduits (15.1%) (including two patients with Melody valves), homograft conduits (12.3%), stented RVOTs (4.7%) (including one patient with a Melody valve) and surgical biological valves (1.9%).
In 7/106 (6.6%) patients, stand-alone RVOT stenting aimed to relieve obstruction. In 3/7 patients, stand-alone RVOT stenting was urgent for acute heart failure and obstructive pulmonary valve endocarditis. One of these three patients died from refractory septic shock 4 days after stenting. The remaining 99/106 (93.4%) patients had RVOT prestenting as preparation for TPVR. The RVOT prestenting and TPVRs were performed as planned in a single procedure in 91/99 (91.9%) of subjects. TPVR was done using the XT (54.9%) and S3 (45.1%) Edwards Sapien valves with diameter of 20 mm (1%), 23 mm (33%), 26 mm (26.4%) and 29 mm (39.6%). In 6/99 (6.1%) patients, TPVR was intentionally rescheduled after successful RVOT prestenting. One of those six patients experienced haemodynamic compromise after wire-related distal left pulmonary artery perforation that was safely embolised. In 2/106 (1.9%) patients, surgical revalvulation was needed after unsuccessful RVOT prestentings. In the first patient with 29 mm large native RVOT, stent slipped down from the balloon during sheath retrieval for uncovering leading to off-target stent implantation, scheduled surgical stent removal and revalvulation. In the second patient with 20 mm large surgical bioprosthetic conduit, stent slipped down from its carrier during delivery inside the sheath leading to excessive manipulations for system retrieval, severe wire-related haemoptysis, abortion of the prestenting procedure and elective surgical revalvulation.
Covered stenting was used in 35/106 (33%) patients, and the indication was prophylactic in 27/35 (77.1%) patients. In the remaining patients, covered stents were applied as a bridge to surgery for obstructive conduit vegetation (n=3), exclusion of RVOT aneurysms (n=2) or Melody valve intimal proliferation (n=1), and as a rescue treatment to seal RVOT conduit rupture (n=2). The XXL/15-ZIG stent was implanted in 68.4% of cases. In four patients with native RVOTs, a single 57 mm XXL/15-ZIG stent was used to simultaneously treat pulmonary branch stenosis. Indications for implanting a second stent (n=8/106, 7.5%) were important stent recoil (n=3), optimal redilation of crushed proximal stent segment (n=2), residual gradient (n=1), conduit rupture (n=1) and securing the first stent with pulmonary branch jailing (n=1).
Overall, median RVOT diameters increased from 20.7 mm (IQR, 15.6–24.4) to 24.4 mm (IQR, 21.3–28) (p<0.001). More specifically, in 50/106 (47.2%) patients with stenotic RVOT lesions, the median TED was 24 mm (IQR, 22–26) and the median PASE was 89.2% (IQR, 81.2%–94.2%). The median RVOT diameters increased from 15.1 mm (IQR, 13–19) to 21.3 mm (IQR, 18.9–23) (p<0.001), and the median PVE was 33.9% (IQR, 18%–48.7%). In this subgroup of 50 patients, 31 (62%) patients had implanted grafts. Dilation beyond the nominal graft diameter was performed in 25/31 (80.6%) patients including 10 (40%) with homograft conduits, 13 (52%) with surgical bioprosthetic conduits and 2 (8%) with surgical biological valves. The percutaneous valve size was 2 mm (IQR, 1–4) larger than the nominal graft size. In the remaining 56/106 (52.8%) patients with non-stenotic RVOTs, the median TED was 28 mm (IQR, 26–30), and the median PASE was 96.7% (IQR, 91.3%–100%). RVOT diameters increased from a median of 23.9 mm (IQR, 21.5–26) to 27.4 mm (IQR, 25–29) (p<0.001), and the median PVE was 12.3% (IQR, 6.7%–21.1%) before TPVR. On a median follow-up of 12 (IQR, 5–16) months, no pulmonary incompetence was noted in patients with TPVR. There was no clinically relevant fracture. The latest median maximal Doppler velocity on the stent was 2 m/s (IQR, 1.5–2.5).
CoA group
Twenty-seven stents were deployed in 26 patients with CoA. 57.7% of patients had native CoA, 30.8% had surgical CoA repair (including three patients with tube interposition) and 19.2% of patients had previous stents. Covered stenting was used in 20/26 (76.9%) patients and was prophylactic in 14/20 (70%) patients. Covered stenting was also applied to exclude four aortic aneurysms and to treat two intrastent intimal proliferations. In 7/26 (26.9%) patients, the coarctation consisted of a pinpoint lesion that was passed retrogradely (figure 2). Two patients had a subatretic CoA requiring brachial–femoral artery rail before retrograde stenting. A second stent was needed in 1/26 (3.8%) patients to cover the lesion entirely. Stenting increased the median coarctation diameter from 6 mm (IQR, 3–12) to 15.3 mm (IQR, 13.7–17.6) (p<0.001), and the median PVE was 161.8% (IQR, 25.8%–326.8%). The median peak-to-peak gradient decreased from 24 mm Hg (IQR, 15–31) to 1 mm Hg (IQR, 0–4) (p<0.001). Angiographic controls showed that the aneurysms had been completely excluded. There were no aortic wall lesion or vascular access complications. Baseline maximal Doppler velocity decreased from 3.2 m/s (IQR, 2.7–4) to 2.2 m/s (IQR, 1.9–2.4) at discharge (p<0.001) and remained stable without any reappearance of diastolic tail on a median follow-up of 9 (IQR, 3–13) months.
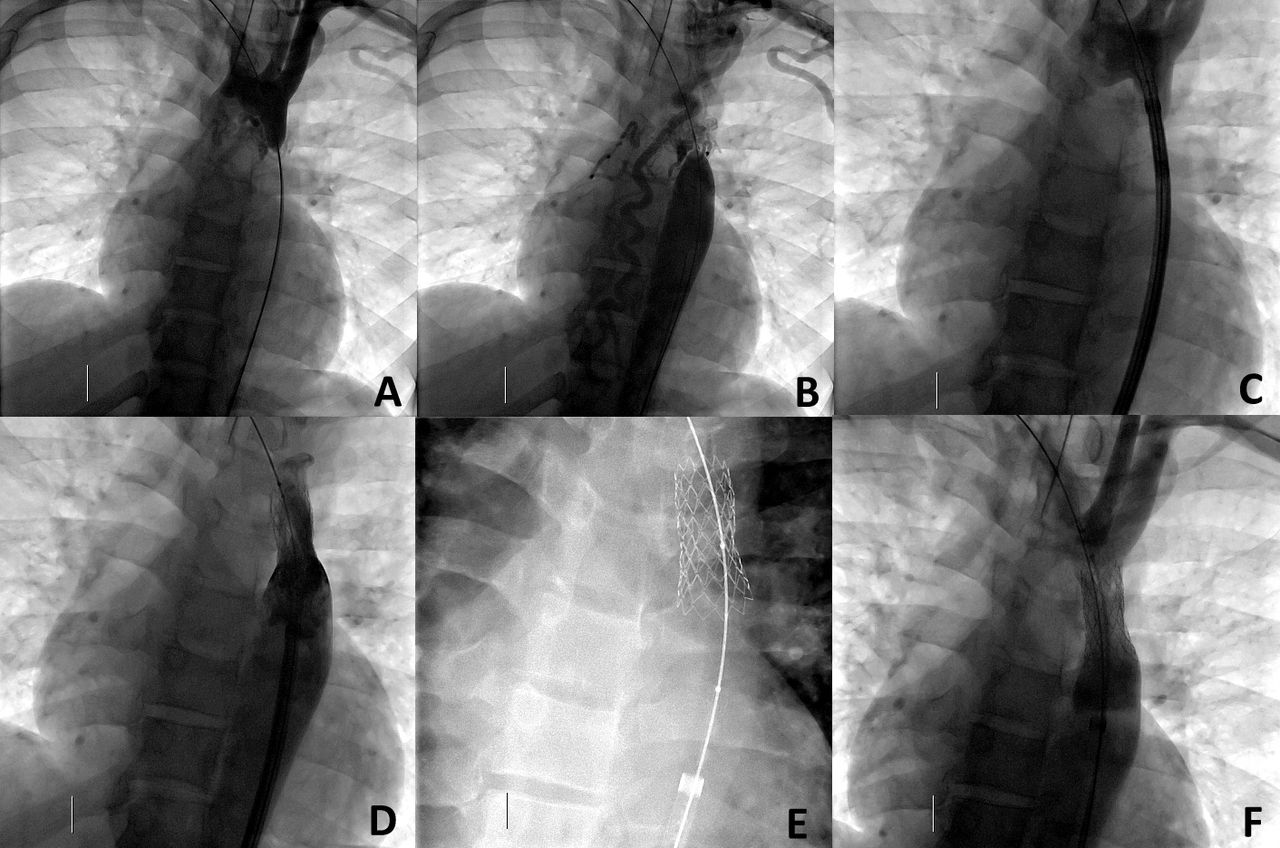
Pinpoint aortic coarctation in a patient aged 17 years (A, B). Positioning of a 43 mm/L Optimus-CVS inside a 12-Fr sheath (C). Successful implantation with a 16 mm/3.5 cm dual balloon (D). Note the stent moulding the vessel anatomy after distal part flaring with a 24 mm/4 cm Altosa-XL balloon (E). Excellent exit angiogram (F).
Closure of Fontan-circuit fenestration group
Twenty-two covered stents were deployed in 21 patients, median age 6.1 years, to close Fontan-circuit fenestration. The AltoSa-XL single balloon catheters (AndraTec) were used to deliver the stents in 71.4% of patients. Two XL stents slipped down the Altosa-XL balloons during uncovering (sheath retrieval) but were easily repositioned over the carriers and implanted into position. In one patient, the positioning of the first stent was not optimal and a second stent was required to abolish right-to-left shunting. The median PASE was 98.2% (IQR, 92.3%–100%). The invasive central venous pressure increased from a median of 12 mmHg (IQR, 11–14) to 14 mmHg (IQR, 12–15) (p=0.112), whereas the oxygen saturation increased from a median of 88% (IQR, 86%–90%) to 97% (IQR, 96%–98%) (p<0.001). Control angiography confirmed complete shunt closure in all patients (figure 3). Results remained stable on a median follow-up of 5 months (IQR, 3–10). Coumadin therapy was stopped in 6/21 (28.6%) patients.
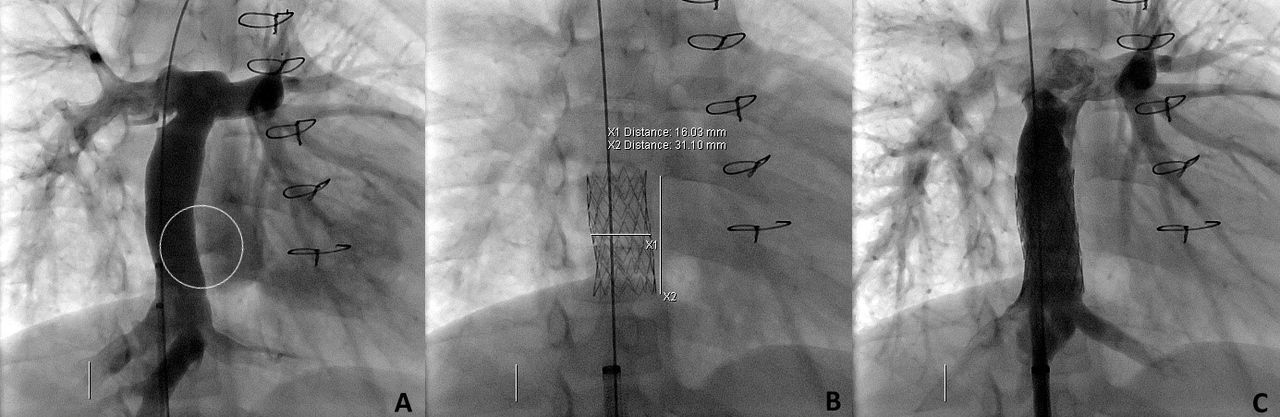
Successful closure of extracardiac (16 mm large Gore-Tex graft) Fontan fenestration (black circle) using 33 mm/XL Optimus-CVS implanted with 16 mm large Altosa-XL balloon (A–C). Note the special design of the stent moulding the anatomy with complete shunt closure (C).
Miscellaneous group
Twenty Optimus stents were deployed for transcatheter repair of superior sinus venosus atrial septal defect with partial anomalous pulmonary venous drainage (SVASD/PAPVD) (using custom-made 80 mm and 100 mm long stents) (n=6), restoration of caval vein baffle (n=3), left pulmonary artery (n=4) (figure 4), innominate vein (n=1), superior caval vein (n=1), or inferior caval vein (n=1) patency, and sealing of an inherited dissecting thoracic aortic aneurysm (n=1). Covered stenting was used in 10/17 (58.8%) patients and was prophylactic in 2/10 (20%) patients. In stenotic lesions, stenting increased the median vessel diameter from 7.7 mm (IQR, 4.7–8.5) to 13.5 mm (IQR, 9.9–22.3) (p<0.001), and the median PVE was 117.4% (IQR, 48%–201%). In two cases of transcatheter repair of SVASD/PAPVD, two overlapping stents were implanted. The use of a second stent was planned before the procedure in the first case and was necessary in the second case to secure the first stent in the superior caval vein after its downward migration. In another patient, second stenting was necessary to completely relieve the superior caval vein baffle obstruction after upward migration of the first stent during implantation.

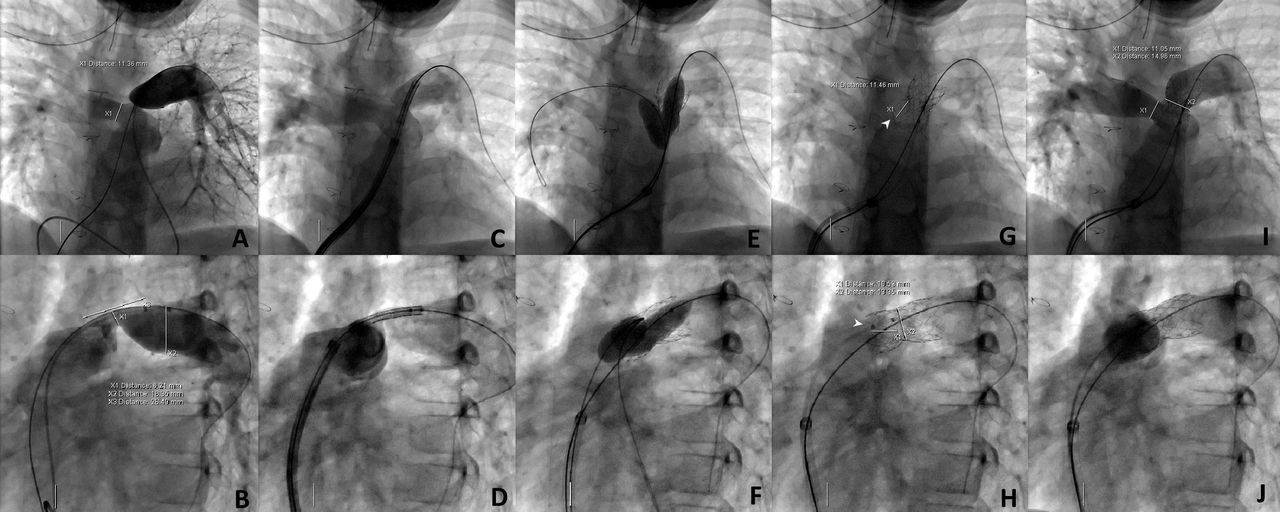
Left pulmonary artery focal and severe stenosis in a patient aged 13.5 years with surgically repaired tetralogy of Fallot (A, B). Positioning of a 33 mm/L bare-metal Optimus stent mounted on a 16 mm/3.5 cm dual balloon inside a 12-Fr sheath (C, D). Successful stent implantation followed by side-cell flaring to the right pulmonary artery with a 12 mm balloon (E, F). Note the stent’s particular design allowing a perfectly circular opening to the right pulmonary artery (white arrows) (G, H). Excellent exit angiogram (I, J).
Stent performance analysis
Overall median stent length was 43 mm (IQR, 38–48 mm), and stent shortening was 10.9% (IQR, 6.1%–15.1%). Analysis showed that shortening significantly increased with stent length (r=0.36, p<0.001) and TED (r=0.5, p<0.001). Distribution of stent shortening values was not the same for the three sizes of Optimus stents: median 6.8% (IQR, 3%–10.4%) for the L/9-ZIG versus median 12.3% (IQR, 4.9%–18.2%) for the XL/12-ZIG versus median 12% (IQR, 7.3%–15.8%) for the XXL/15-ZIG (p=0.003). In addition, median stent shortening of bare-metal stents was 12.3% (IQR, 8.1%–17.4%) and was significantly higher than median stent shortening of PTFE-covered stents, 8.6% (IQR, 3.7%–13.8%) (p=0.001). Vessel anatomy (curved vs straight), vessel type (arterial vs venous) and presence or absence of stenotic lesion did not significantly affect the distribution of stent shortening values. Multivariable analysis showed that TED (OR: 0.66, 95% CI: 0.38 to 0.93) was alone associated with increased odds of stent length shortening after implantation (table 3). The PASE was not significantly correlated with stent length (r=−0.02, p=0.83), TED (r=−0.09, p=0.25) or delivery balloon-to-stent length ratio (r=0.03, p=0.72). Optimus size and design, vessel anatomy and type did not as well significantly affect the distribution of PASE values.
Univariable and multivariable linear regression analyses of factors associated with stent length shortening
Discussion
The progressive change in the design and material of stents was necessary to cover the attributes of the ideal stent: safe delivery to the target lesion (low profile, flexibility and easy trackability), high performance at the site of implantation (radial force, vascular conformability, retrievability, expansion without shortening and fracture resistance) and a reliable PTFE covering when needed. Previously tested medium and large stents presented a certain compromise between technical advantages and design disadvantages.5 7 12 The gap of extralarge stents in the armamentarium was also problematic.9 13 For all those reasons, Optimus and Optimus-CVS were developed to tackle the interventionist’s daily challenges promising performance and outcomes.
Advantages of Optimus stents
Optimus stents are designed with cobalt–chromium hybrid-cell technology to keep together sufficiently high radial strength for stenosis relief, resistance to fracture, along with flexibility and anchoring properties. The radial strength of Optimus stents was satisfactory, and TEDs were achieved in most cases with sufficiently high PASE and PVE values. The need for secondary stenting in case of important recoil or residual gradient was limited to four cases (2.3%) in this study, avoiding excess implants. The anchoring properties of Optimus stents were particular. There was no case of embolisation or migration after stent implantation. The hybrid design with thin and sharp laser-cut struts offered the necessary retention forces to effectively prestent compliant and extralarge conduit-free RVOTs up to 30 mm in diameter. Newly implanted stents were firmly fixed to the RVOTs even when repetitive or laborious manipulations of extralarge sheaths had to be taken across the stent to facilitate safe delivery of the valves. Ninety-two percentage of the TPVRs were done immediately after RVOT prestentings obviating the need for the two-part procedure that was reported as a strategy to avoid dislodgment of newly implanted stents.13 14 The rounded edges ensured atraumatic wall coverage. We observed only three cases of balloon rupture of which two were secondary to exposed fragments of previously implanted fractured stents within the target zone. We did not observe non-harmonic strut expansion with overexposed sharp edges, a complication previously reported with stents of similar design.14 15 The segment-to-segment Omega connectors contributed to homogeneous expansion that was achieved with matching balloon-to-stent length and slow expansion of dual delivery balloons.16 Optimus stents also offered the flexibility needed for the treatment of angulated regions without straightening the anatomy or compressing nearby structures. On top of all this, the hybrid design allowed intervention through open cells, especially when the branch jailing technique is needed in extralarge native RVOTs or complex bifurcation stenosis (figure 4). The shortening was low and as expected, with TED being the only associated risk factor. This gives a more predictable treatment with only one implanted stent, independently of the landing zone characteristics.
The portfolio of Optimus stents is one the largest in the armamentarium combining nine lengths, and three sizes with overlapping functional expansion ranges, along with bare-metal and covered versions making Optimus stents suitable for tailored treatment of various congenital malformations. One of the most interesting features of Optimus stents is the XXL/15-ZIG version that offers a scaffold to anchor the valve within the distensible native extralarge RVOTs, reducing the risks of valve dislodgement, perforation, paravalvular leak and stent fracture.17 This XXL version was necessary to cover the gap in existing products, especially since the newest extralarge TPVR systems and implantable RVOT size reducers were unavailable during study period in most European countries.18 19
Optimus stents are designed with competitive low profile deliverability and can be deployed through sheathes 1-Fr to 3-Fr size smaller than the ones required for similar stents.8 9 This is a major advantage in children and particularly in arterial interventions. The overall rate of vascular access complications was low in this survey, and all arterial interventions were event-free. AndraTec recommends AltoSa-XL and AltoSa-XL-Gemini balloons for implanting Optimus stents with the lowest profile. However, crimping the stent on these balloons is not easy and the opening of the AltoSa-XL-Gemini balloons is not optimal. Practically, Altosa-XL balloons can deliver Optimus-L through 10-Fr sheaths and Optimus-XL through 12-Fr sheaths. This is a major advantage to consider when treating paediatric CoA knowing that Optimus stents in both L and XL versions can be re-expanded during follow-up to catch up adult vessel diameter. Mounting Optimus-XXL over Altosa-XL-Gemini dual balloons can also reach diameters up to 30 mm through 14-Fr sheaths which is also an advantage for prestenting the RVOTs.
Pitfalls of Optimus stents
Pitfalls of Optimus stents can be limited to difficulty in hand crimping the stents on balloons. We observed few stents sliding off their carriers during sheath insertion, delivery within low profile sheath or sheath retrieval for stent uncovering, resulting in three patients to system withdrawal and remounting and in two patients to implantation failure. This difficulty in stent crimping was not observed with large delivery dual balloons (diameter >24 mm) that offered a sufficient crimping platform for XXL stents. Over time, stent grip was enhanced by partial balloon inflation before stent mounting and or temporarily wrapping the stent with an umbilical tape. Short loaders were recently introduced in four sizes and facilitated stent insertion through traditional valved Cook sheaths. In tortuous pathways, mild inflation of the outer balloon was used to create ‘shoulders’ with anterior shoulder to assist stent progression and posterior shoulder to avoid stent sliding off the balloon. In this case, a one to two additional increase in the Fr profile of the balloon-stent unit had to be considered. In comparison, premounted large to extralarge stents are quick to prepare, pass easily through the sheath valve and can be advanced safely without a long sheath as they adhere firmly to the balloon catheter.20–22 This level of security and performance was reached when crimping the stents with a crimper device. Therefore, the introduction of premounted Optimus stents should be considered for highly complex and urgent procedures.
Extended possibilities with Optimus-CVS
Concerns about the performance of available covered stents kept the debates on indications and effectiveness of covered stenting ongoing.5 7 23 Covered stents have been routinely applied as ‘rescue’ treatment in case of an acute rupture or aneurysm formation.2 3 There is also a growing experience with prophylactic use of covered stenting to prevent complications.3 The particular technologies of Optimus-CVS and its low profile might put an end to these controversies. The covering of Optimus-CVS can be stretched up to 32 mm without tearing or creating flaps. We have progressively evolved from ‘curative’ to ‘prophylactic’ use of Optimus-CVS, especially when a significant increase in circumference is imposed on a poorly compliant or calcified wall. Indeed, Optimus-CVS sealed existing and expected graft tears at any TED with more complete dilation and better expected long-term outcomes. This approach was safely applied in narrow and subatretic coarctations while undoubtedly creating major tears in the vessel wall. Performance of Optimus-CVS was optimal even in cases with important discrepancies between the stenotic area and the largest vessel diameter (figure 2). Similarly, in patients with irregular RVOT conduits or calcified homografts, covered stenting permitted expansion of the conduit up to and beyond the nominal graft size to implant an adequately sized valve. Covered stenting will also create a more linear landing zone, avoiding RVOT irregularities at the implant site that might be a risk factor for infective endocarditis.24 Theoretically, a sharp calcified lesion might tear the membrane prematurely. We did not observe membrane failure on exit angiograms and follow-up ultrasound assessments suggested that membrane integrity was preserved.
The strongest competitor of Optimus-CVS is the covered CP stent that has been widely used with excellent results.3 23 However, the fragility and design of the covering imply precautious manipulations. Excessive stent shortening and PTFE-coating irregularities and overstretching have been seen with fully expanded covered CP stents negating many benefits of the covered nature.3 7 In comparison, the thermally bonded sandwich design of Optimus-CVS covering ensured optimal stability of the PTFE membrane to the metal frame8 (figure 5). This secured PTFE attachment was helpful in our experience when facing difficulties in inserting the stent through the valve or in negotiating tortuous anatomies to deliver the stent into position. The end-free design optimised stent positioning with less fear of compromising side-vessel patency. It was advantageous when targeting low-located fenestration without risking jailing the hepatic veins. In case of side branch occlusion, previous authors even highlighted the predictable behaviour of the Optimus-CVS covering in response to intentional repermabilisation.7 Finally, covered stenting for SVASD/PAPVD correction is a newly developed intervention and was mainly performed using 10-ZIG-covered CP stents.25 The promising characteristics of the Optimus-CVS made this new stent suitable for this procedure, especially since stent length and PTFE-covering design can be customised according to the patient’s needs11 (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Slightly expanded custom-made 85 mm/XXL Optimus bare-metal stent (A). Custom-made 80 mm/XXL Optimus-CVS with particular PTFE covering design for SVASD/PAPVD transcatheter repair (B). Note the 2.5 rows of bare-metal cells (≈25 mm) at the cranial end of the stent for maximal caval anchoring and patency of innominate and azygos veins (B). Stable covering with exactly 2.5 rows of bare-metal cells when the stent is inflated with a 30 mm dual balloon. PTFE, polytetrafluoroethylene; SVASD/PAPVD, sinus venosus atrial septal defect with partial anomalous pulmonary venous drainage.
Limitations
The main limitation of our report is the lack of long-term follow-up. We do not routinely perform CT scan to detect stent fracture, restenosis or aneurysm formation after stent placement. Therefore, under-reporting of these complications cannot be excluded. Long-term follow-up is also needed to confirm if Optimus-CVS can be redilated without membrane rupture after somatic growth, or when the stent was not fully dilated initially. A formal protocol-driven monitored study is required.
Conclusion
We report the largest experience with bare-metal and PTFE-covered Optimus stents in CHD interventions. Safety and efficacy were demonstrated across a wide spectrum of patient sizes, anatomical variations and clinical applications. Mechanical stent performance is reliable and short-to-midterm outcomes are very encouraging for widespread use.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the institutional review board (MR004: 2022-0503161831). All procedures contributing to this work comply with the ethical standards of the relevant national guidelines on human experimentation, and with the Helsinki Declaration of 1975, as revised in 2008.
Acknowledgments
We thank the entire catheterisation laboratory staff for their support and technical assistance during these procedures. We thank also Dr Mathieu Albertini for his participation in the data collection of centre 3.
References
Footnotes
Contributors RNH performed stratifications and all statistical calculations. RNH analysed the results, designed illustrative material, and took the lead in writing and revising the entire manuscript. SMM and DB supervised the project. All authors discussed the results, read and approved the final version of the manuscript. All authors are responsible for the overall content as guarantors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.