Article Text

Abstract
Objective
Sarcoidosis is over-represented among victims of cardiac arrest. We aimed to establish whether sarcoidosis is associated with out-of-hospital cardiac arrest (OHCA) in the general population.
Methods
We conducted a nested case–control study in a nationwide cohort of individuals between 1 June 2001 and 31 December 2015 in Denmark. OHCA cases from presumed cardiac causes were matched 1:10 by sex and age on OHCA date with non-OHCA controls from the general population. The association between sarcoidosis and OHCA was assessed using Cox regression by calculating HR and 95% CIs. Models were adjusted for cardiovascular disease. Finally, stratified analyses were performed according to sex, heart failure and ischaemic heart disease.
Results We identified 35 195 OHCA cases and 351 950 matched controls without OHCA (median age 72 years and 66.8% male). Patients with sarcoidosis had higher rate of OHCA compared with the general population after adjustments for common OHCA risk factors (HR 1.51, 95% CI 1.19 to 1.92). This increased OHCA rate occurred in women (HR 2.11, 95% CI 1.42 to 3.12) but not in men (HR 1.27, 95% CI 0.93 to 1.72; p value interaction=0.033), and was larger in patients with than without heart failure (HRheart failure: 2.59, 95% CI 1.42 to 4.73; HRno heart failure: 1.33, 95% CI 1.01 to 1.74; p value interaction: 0.007). The HR associated with sarcoidosis did not vary by the presence of ischaemic heart disease.
Conclusion Patients with sarcoidosis have a higher OHCA rate than the general population. This increased OHCA rate occurred in women but not in men, and was larger in patients with than without heart failure.
- Epidemiology
- Inflammation
- Electrophysiology
- Ventricular Fibrillation
- Heart Arrest
Data availability statement
Data underlying the present article is not available to be shared publicly, as access to Danish registry raw data for research purposes must be granted individually by Danish authorities.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Previous studies demonstrated an increased risk of cardiovascular comorbidity associated with sarcoidosis and reported an over-representation of sarcoidosis among victims of cardiac arrest.
WHAT THIS STUDY ADDS
We estimated overall and stratified HRs of out-of-hospital cardiac arrest (OHCA) associated with sarcoidosis in a large cohort specifically designed to study OHCA in the general Danish population (total 35 195 patients with OHCA).
Patients with sarcoidosis are associated with a higher OHCA rate than the general population after adjustments for common OHCA risk factors. This increased OHCA rate occurred in women but not in men, and was larger in patients with than without heart failure.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This study raises awareness of the higher risks of OHCA in patients with sarcoidosis.
Early risk monitoring is needed to prevent OHCA in sarcoidosis patients.
The mechanism(s) of sudden death in chronic inflammatory diseases need to be clarified.
Introduction
Out-of-hospital cardiac arrest (OHCA) is an increasing global health burden estimated to account for 50% of all cardiovascular deaths and up to 20% of all natural deaths in Western societies.1 The majority of OHCA is usually caused by cardiac arrhythmias (ventricular fibrillation/ventricular tachycardia) that occur most frequently in the setting of known cardiac diseases such as coronary heart disease, cardiomyopathy and heart failure.2 In addition to known cardiac disease, growing evidence implicates that non-cardiac disease may also increase the risk of OHCA.3
Sarcoidosis is a systemic chronic inflammatory disease of unknown cause characterised by the formation of immune granulomas in affected tissues.4 Although it predominantly affects the lungs, intrathoracic lymph nodes, skin5 or a combination of these sites, sarcoidosis may affect virtually any organ, including the heart.6 The estimated prevalence of cardiac involvement (cardiac sarcoidosis) is 5% in systemic sarcoidosis.7 It is likely that this prevalence of cardiac sarcoidosis is underestimated since many patients with cardiac sarcoidosis have nonspecific symptoms. Autopsy studies and cardiac imaging studies of patients with systemic sarcoidosis suggest a higher prevalence of cardiac involvement.8 9
Patients with sarcoidosis are at increased risk of cardiovascular morbidity10 and previous studies suggested an increased risk of cardiac arrest in patients with sarcoidosis.8 11–13 However, most of these data were either derived from studies with small populations8 or limited by the use of in-hospital diagnoses to detect cardiac arrest,11–13 which may cause important inclusion bias by omitting cardiac arrest patients who died before hospital admission. Further, it remains unknown which subgroups of patients with sarcoidosis are at highest risk of cardiac arrest and may benefit most from preventive measures.
Our aim of the current study was therefore twofold: (1) to establish whether sarcoidosis is associated with increased hazard of OHCA using a large dataset from a cohort that was specifically designed to study OHCA in the general population and (2) to identify subgroups with the highest hazard of OHCA associated with sarcoidosis by performing stratified analyses according to sex and presence of cardiovascular risk factors such as ischaemic heart disease and heart failure.
Methods
Study design and population
We conducted a nested case–control study in a nationwide cohort of individuals between 1 June 2001 and 31 December 2015. Cases were OHCA victims from presumed cardiac causes from The Danish Cardiac Arrest Registry. Each case was matched with up to 10 non-OHCA controls using risk set matching based on age, sex and the index date (date of OHCA) that were drawn from the general population. We used the same study design and population previously.14
Data sources
This study was based on nationwide Danish health registers. For the present study, the following registries were linked at an individual patient level using a unique identification number that is assigned to all Danish residents on birth allowing large-scale research with nationwide coverage: (1) The Danish Civil Registry, (2) The Danish National Patient Registry, (3) The National Prescription Registry, (4) The Danish Registry of Causes of Death and (5) The Danish Cardiac Arrest Registry. These registries are well described and have been previously used.14–19
Briefly, The Danish Civil Registry contains information on patient’s date of birth, sex as well as emigration and immigration history.15 The Danish National Patient Registry provides data on all the hospital admissions, including diagnoses and procedural codes and is coded according to the International Classification of Diseases 10th edition (ICD-10).16 The National Prescription Registry contains information on complete drug-dispensing records coded according to the Anatomical Therapeutic Chemical (ATC) Classification system.17 The Danish Registry of Causes of Death provides data on the cause of death.18 The Danish Cardiac Arrest Registry is an ongoing nationwide registry that holds information on all OHCAs since June 2001 (5.8 million people, covering 100% of the Danish population).14 An OHCA is included when a clinical condition of cardiac arrest results in resuscitation efforts either by bystanders (with activation of the Emergence Medical Services (EMS) system) or by EMS personnel. The capture of OHCA cases is nearly complete because the EMS is activated for all clinical emergencies in Denmark and EMS personnel are required to complete a case report form for every OHCA. The presumed cause of OHCA was obtained from the death certificates and discharge diagnosis codes. OHCAs with diagnosis codes for cardiac disease, unknown disease or unexpected collapse were classified as being of presumed cardiac cause.14 Patients who suffered OHCA from non-cardiac causes (eg, trauma, attempted suicide, drug overdose, drowning, violent attack and other non-cardiac diseases) were excluded.
Exposure of interest and covariates
Patients with sarcoidosis were identified by using diagnoses codes from hospital admissions registered in the Danish National Patient Registry up to ten years prior to index date.
Comorbidities were defined binarily as present if the diagnoses were given up to 10 years before the index date. The following known risk factors of OHCA were identified: heart failure, ischaemic heart disease, cerebrovascular disease, atrial fibrillation, peripheral artery disease and diabetes mellitus. The latter was defined as the use of antidiabetic drugs within 6 months before the index date as we did previously,14 since the diagnosis code of diabetes has a low sensitivity in the Danish registries.
Concomitant pharmacotherapy was defined as one or more checked prescriptions up to 6 months before the index date (see table 1 for the included drugs and online supplemental table 1 for the ATC codes) as we did previously.14 QT-prolonging drugs were defined as advised by the CredibleMeds list (www.CredibleMeds.org).20 For antimicrobial drugs with QT-interval prolonging potential, we shortened the exposure period to 14 days before the index date because these drugs are generally prescribed for short periods. Please see online supplemental table 1 for all the ICD-10 and ATC codes used throughout the study.
Supplemental material
Baseline characteristics of the study population
Statistical analyses
We used Cox proportional hazards regression model to estimate the association between sarcoidosis and OHCA by calculating the HR and (95% CI. Models were adjusted for the following common OHCA risk factors: heart failure, ischaemic heart disease, cerebrovascular disease, atrial fibrillation, peripheral artery disease, diabetes mellitus and the use of QT-prolonging drugs. First, we studied the association between sarcoidosis and OHCA in the general population. Next, we performed a sensitivity analyses by additionally adjusting for the presence of implantable cardioverter defibrillator (ICD), pacemaker or cardiac resynchronisation therapy (CRT). Second, we stratified according to sex, cardiovascular disease, heart failure and ischaemic heart disease. By performing stratified analyses according to cardiovascular disease, heart failure and ischaemic heart disease our original matching was lost, therefore, we additionally adjusted for age and sex in our model as we did previously.14 Interaction between sarcoidosis and either sex, cardiovascular disease, heart failure or ischaemic heart disease was estimated by including the cross product of the two factors as a variable in the model. Further, we examined whether patient characteristics were different between cases with and without sarcoidosis. Categorical data were presented as absolute numbers and percentages, and continuous data as medians together with their associated IQR.
Results
Subject characteristics
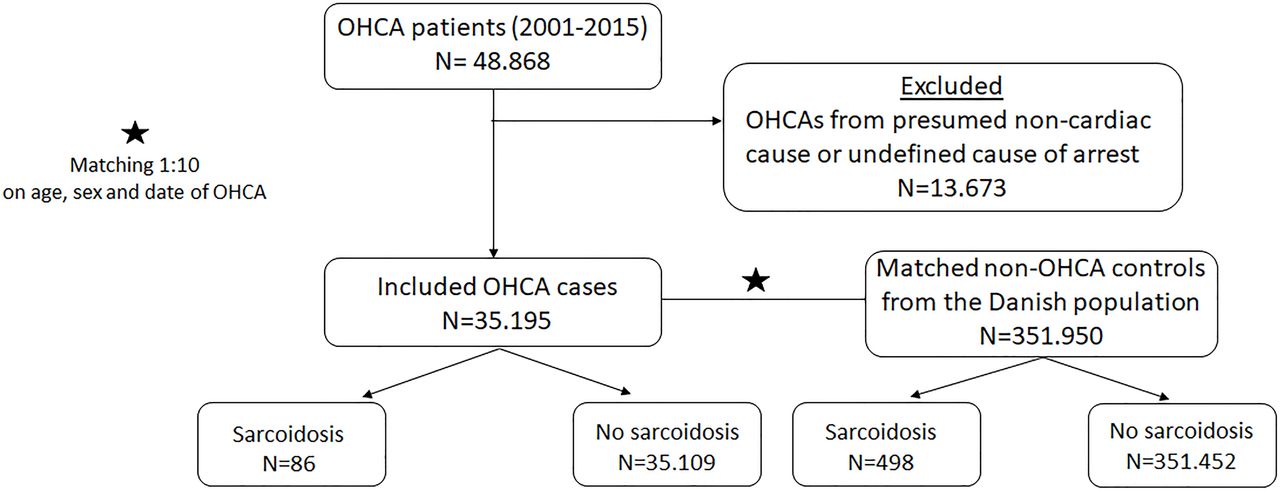
We identified 35 195 OHCA cases and 351 950 matched controls without OHCA (figure 1). The median age was 72 years and 66.8% were male (table 1). Compared with non-OHCA controls, OHCA cases had a larger burden of cardiovascular disease and concomitant pharmacotherapy (table 1). Table 2 shows the characteristics of OHCA cases with and without sarcoidosis. Although cases with sarcoidosis were younger than cases without sarcoidosis (67 vs 72 years), the proportion of cardiovascular comorbidities was higher among cases with sarcoidosis compared with cases without sarcoidosis regarding heart failure (30.23% vs 20.25%), ischaemic heart disease (30.23% vs 26.46%), cerebrovascular disease (15.12% vs 13.95%), atrial fibrillation (23.26% vs 17.32%), peripheral artery disease (13.95% vs 11.11%) and diabetes mellitus (23.26% vs 15.12%). Likewise, use of beta-blockers, diuretics, antithrombotics and QT-prolonging drugs was more prevalent among cases with sarcoidosis than cases without sarcoidosis (table 2).

Flow chart of patient inclusion OHCA, out-of-hospital cardiac arrest.
Characteristics of out-of-hospital cardiac arrest cases with and out without sarcoidosis
Association between sarcoidosis and OHCA
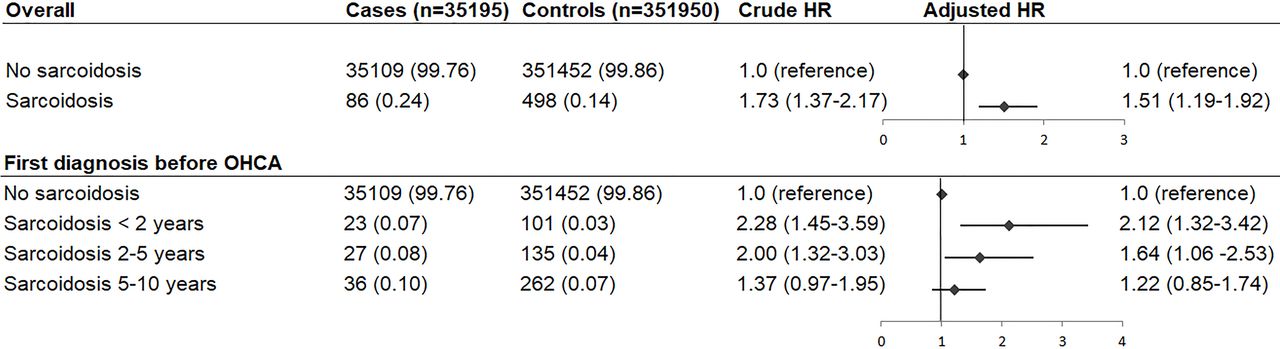
Sarcoidosis was diagnosed in 86 (0.24%) OHCA cases and 498 (0.14%) non-OHCA controls, and was associated with increased hazard of OHCA after adjusting for common OHCA risk factors (HR 1.51, 95% CI 1.19 to 1.92, figure 2). This increased HR remained persisted after adjustments for the presence of ICD, pacemaker or CRT (HR 1.51, 95% CI 1.19 to 1.91). We found that OHCA rate was higher when the first diagnosis of sarcoidosis was within 2 years prior to index date compared with the rest of the follow-up (HR 2.12, 95% CI 1.32 to 3.42, figure 2).

{kind=link}
{kind=link}
HRs of the association between sarcoidosis and out-of-hospital cardiac arrest: overall and divided by first diagnosis date of sarcoidosis. Numbers in table are number (%) unless indicated otherwise. Error bars denote 95% CI. HR adjusted for presence of cardiovascular disease and the use of QT-prolonging drugs. OHCA, out-of-hospital cardiac arrest.
Stratified analyses
The results of the stratified analyses are summarised in table 3 and presented in detail in online supplemental figure 1. We found that increased OHCA rate occurred in women (HR 2.11, 95% CI 1.42 to 3.12) but not in men (HR 1.27, 95% CI 0.93 to 1.72; p value interaction=0.033, table 3). Stratification according to cardiovascular disease showed no statistically significant difference in OHCA rate between patients with and without cardiovascular disease (HRcardiovascular disease 1.59, 95% CI 1.18 to 2.15; HRno cardiovascular disease 1.21, 95% CI 0.82 to 1.80; p value interaction=0.128, table 3). Stratification according to heart failure disease revealed that the association between sarcoidosis and OHCA was higher in patients with heart failure (HR 2.59, 95% CI 1.42 to 4.73) than in those without heart failure (HR 1.33, 95% CI 1.01 to 1.74; p value interaction=0.007, table 3). Finally, stratified analyses according to ischaemic heart disease showed no statistically significant difference in OHCA rate between patient with and without ischaemic heart disease (p value interaction=0.437).
HRs of the association between sarcoidosis and out-of-hospital cardiac arrest: stratification according to sex, cardiovascular disease, heart failure and ischaemic heart disease
Discussion
This nationwide nested case–control study yielded two important results: (1) sarcoidosis was associated with a 1.5-fold increased hazard of OHCA compared with the general population, and persisted after adjustments for common OHCA risk factors and (2) this association occurred in women but not in men, and was larger in patients with heart failure than in patients without heart failure.
Comparison with previous studies
Our finding that sarcoidosis was associated with increased rate of OHCA is supported by previous studies.11–13 21. Yafasova et al investigated the long-term risk of the composite outcome of ICD implantation, ventricular arrhythmias or cardiac arrest in patients with sarcoidosis compared with matched control subjects in a cohort study, and described significant higher HR of the composite cardiac outcome associated with sarcoidosis.21 Another cohort study by Te et al reported that patients with sarcoidosis had significant higher risk of ventricular tachycardia compared with matched controls.11 A large study of 369 285 sarcoidosis-related hospitalisations by Desai et al reported that nearly one-fifth of sarcoidosis patients experience arrhythmias during hospitalisation, and that the arrhythmia group had significantly higher in-hospital mortality than the non-arrhythmia group.12 Finally, Salama et al investigated in a longitudinal observational database whether sarcoidosis was associated with ventricular arrhythmias and cardiac arrest, and reported higher ORs of ventricular arrhythmias and cardiac arrest associated with sarcoidosis compared with controls without sarcoidosis.13 Previous studies, however, used in-hospital diagnosis to define cardiac arrhythmias and/or cardiac arrest, which may cause important inclusion bias by omitting patients who died before hospital admission. Our study was specifically designed to study OHCA in the general population. We could enrol both patients who survived to hospital admission and those who died prehospital due to our collaboration with all EMS departments. This allowed us to include patients who collapsed suddenly and unexpectedly, and to minimise selection bias by the use of an unselected cohort of OHCA patients.
Is sarcoidosis an independent risk factor for OHCA?
Previous studies demonstrated an increased risk of heart failure and atrial fibrillation associated with sarcoidosis.21 22 Both conditions have been related to OHCA,2 and therefore, the observed association between sarcoidosis and OHCA may be related to these underlying comorbidities. Nevertheless, sarcoidosis remained significantly associated with OHCA after adjustment for the presence of heart failure and atrial fibrillation. This finding together with an increased OHCA rate associated with sarcoidosis in individuals without cardiovascular comorbidities, suggests that it is unlikely that traditional risk factors alone explain the observed association in our study. Several mechanisms for our observed association of sarcoidosis with OHCA may be proposed. Granulomatous infiltration of the ventricle may result in inflammation and fibrosis which in turn may facilitate reentrant arrhythmias and life-threatening arrhythmias.23 In addition, elevated levels of interleukin-6 and tumour necrosis factor α have been identified in patients with sarcoidosis.5 Increased levels of these cytokines may modulate the function and/or expression of cardiac potassium channels which largely drives cardiac repolarisation.24 This may result in QT-prolongation and thereby increase the risk of ventricular arrhythmias and OHCA in sarcoidosis patients based on Torsade de Pointes arrhythmia. This may occur in women (that have smaller repolarisation reserve than men due to lower expression of repolarisation channels25) or in individuals more susceptible due to acquired factors (eg, heart failure secondary to downregulation potassium currents26). This may at least in part explain the higher OHCA rate observed in women and in patients with heart failure in our study. Finally, we found that OHCA rate associated with sarcoidosis was highest when the first diagnosis of sarcoidosis was within 2 years prior to index date. It is likely that this period (first diagnosis of sarcoidosis within 2 years prior to index date) may reflect a period of active inflammation while a first diagnosis of sarcoidosis before 2 years prior to index date may reflect a stabilised chronic condition. This suggests that acute inflammatory responses rather than chronic remodelling of the heart underlie OHCA in patients with sarcoidosis. However, given that previous studies reported associations of sarcoidosis with cardiovascular outcomes such as heart failure.21 22 it is possible that heart failure could contribute to increased OHCA rate observed in our study. Nevertheless, when patients with heart failure were excluded in a subanalysis, we observed that the OHCA rate was higher when the first diagnosis of sarcoidosis was within 2 years prior to index date (see online supplemental table 2). Thus, it is unlikely that heart failure alone explains this relationship.
Methodological considerations
We should acknowledge that our stratified analysis was based on small sample sizes, which may have resulted in possibly low statistical power. Thus, our study highlights the need for future larger-scale studies. Second, despite adjustment for potential confounders the possibility of residual confounding in our analyses cannot be excluded since data on risk factors for cardiovascular disease such as lifestyle factors (body mass index, smoking, alcohol use) and left ventricular ejection fraction were not available to include in our analyses. However, considering that OHCA occurs unexpectedly, and therefore, unpredictably, it is difficult, if not impossible, to obtain data on some clinical variables (such as left ventricular ejection fraction) shortly before the OHCA occurrence in a uniform manner across the study population. Furthermore, data on disease severity were not available to include in our analyses since information regarding comorbidities was defined as a binary variable which makes it hard to adjust properly for diseases such as heart failure and diabetes mellitus with a broad spectrum of diseases severities. Also, although the majority of the diagnosis codes from the Danish National Patient Registry have undergone scrutiny for data quality and generally shows high validity,27 the diagnosis codes used to identify sarcoidosis have not been validated previously, which may result in misclassification bias. Finally, we had no information regarding histological tissue analyses in our registries and we could not exclude the presence cardiac sarcoidosis among those diagnosed with sarcoidosis as the ICD-10 code D8685 to identify sarcoid myocarditis is not used in Denmark.
Conclusion
Patients with sarcoidosis have a higher OHCA rate compared with the general population. This increased OHCA rate occurred in women but not in men, and is larger in patients with heart failure than in patients without heart failure. Awareness of the higher risks of OHCA in patients with sarcoidosis as well as an early risk monitoring is needed to prevent OHCA.
Data availability statement
Data underlying the present article is not available to be shared publicly, as access to Danish registry raw data for research purposes must be granted individually by Danish authorities.
Ethics statements
Patient consent for publication
Ethics approval
The use of register-based data has been approved by the Danish Data Protection Agency (Ref.no. 2007-58-0015, local ref.no. GEH-2014-017, I-Suite 0.2735). No further ethical approval is required for register-based studies in Denmark.
Acknowledgments
For completion of the case reports which form the Danish Cardiac Arrest Registry, the authors thank the Danish Emergency Medical Services.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors TEE conceived the study idea. TEE, RC and GHG designed the research (methods). TEE performed the statistical analyses and wrote the manuscript. All authors critically revised and approved the manuscript. TEE and GHG are responsible for the overall content as guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.