Article Text

Abstract
Background Cilostazol is an oral antiplatelet agent currently indicated for treatment of intermittent claudication. There is evidence that cilostazol may reduce femoropopliteal restenosis after percutaneous endovascular intervention.
Methods We searched PubMed, Scopus and Cochrane databases from 1966 through September 2013 for randomised controlled trials (RCTs) evaluating the addition of cilostazol to standard care in patients receiving femoropopliteal endovascular treatment. Restenosis, target lesion revascularisation and combined adverse outcomes (death, revascularisation and amputation) within 1–2 years postprocedure were evaluated.
Results Of 205 articles, three RCTs were included in the analysis. The pooled data provided a total of 396 patients, 195 of whom received cilostazol. When compared to standard medical therapy alone, cilostazol significantly reduced the risk of restenosis (risk difference −0.20; 95% CI −0.29 to −0.11; p<0.0001; number needed to treat 5), target lesion revascularisation (risk difference −0.17; 95% CI −0.25 to −0.09; p<0.0001; number needed to treat 6). Death and amputation were not different in between groups.
Conclusions and limitation Cilostazol significantly increases femoropopliteal patency and decreases adverse outcomes in percutaneous endovascular intervention. However, further RCTs are needed because of limited sample size; this meta-analysis represents the best current evidence.
- PERIPHERAL VASCULAR DISEASE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
-
Cilostazol could decrease restenosis rates after endovascular therapy for peripheral artery disease, but the current randomised controlled trials evaluating this have small sample size.
What does this study add?
-
We sought to improve the current level of evidence by conducting a systematic review and meta-analysis of cilostazol and outcomes after endovascular therapy for peripheral artery disease. We discovered that compared to standard medical therapy alone, cilostazol significantly reduced the risk of restenosis and target lesion revascularisation without any significant side effects.
How might this impact on clinical practice?
-
Our study provides the best current evidence for using cilostazol after endovascular therapy in peripheral artery disease as well as a rationale for a large, multicentre randomised controlled trial.
Introduction
Peripheral arterial disease (PAD) is highly prevalent and has been demonstrated to increase cardiovascular mortality by 15-fold in individuals with severe symptomatic large-vessel disease.1 Nevertheless, it still remains an underdiagnosed and undertreated condition.2 Femoropopliteal lesions account for nearly three quarters of lower extremity PAD.3 ,4 Revascularisation is required for patients with critical limb ischaemia. The most recent guidelines on the management of femoropopliteal PAD have expanded the indications for endovascular therapy (EVT) to the detriment of surgical revascularisation.5–7
Antiplatelet therapy is recommended after EVT for PAD.5 Cilostazol is a phosphodiesterase-3 inhibitor indicated for the treatment of intermittent claudication.5 ,8 The potential benefits of cilostazol after EVT for PAD are not addressed in current guidelines. Therefore, we decided to perform a systematic literature review and meta-analysis of the outcomes of randomised controlled trials (RCTs) that compare cilostazol to standard therapy alone after EVT for femoropopliteal PAD disease. Cilostazol could potentially improve procedural outcomes at a low cost, as it has been demonstrated to be cost-effective for the treatment of intermittent claudication due to PAD.9 ,10
Materials and methods
Search strategy
We systematically searched PubMed, Scopus and Cochrane Central Register of Controlled Trials for RCTs from 1966 to September 2013, which compared cilostazol to standard medical therapy in patients with femoropopliteal EVT. The review was performed in accordance with established methods for systematic reviews in cardiovascular medicine.11 The following medical subject heading terms were included for a MEDLINE search and adapted for other databases as needed: “cilostazol” AND (“peripheral arterial disease” OR “endovascular therapy” OR “femoropopliteal”). In addition to searching databases, reference lists of all included studies, meta-analyses and reviews were manually searched, including unpublished data. There was neither language nor patient population size restriction for the search.
Data extraction
Two authors independently completed data extraction after following defined search criteria and quality assessment. They obtained data from tables, text and graphs. When the data were presented in percentage the absolute values were calculated. Disagreements were resolved by consensus after review by the senior author of the study.
Selection criteria
Inclusion criteria were RCTs with (1) a direct comparison between patients treated with cilostazol and a control group who received standard medical therapy alone; (2) patients with femoropopliteal lesions due to PAD; (3) patients who received EVT; and (4) reports of the primary and secondary outcomes. Exclusion criteria were (1) studies that only reported outcomes of cilostazol, without a direct comparison to a control group; (2) observational studies; (3) non-randomised clinical trials; and (4) overlapping patient population, identified by studies developed over the same period of time with common authors or common study centres. In this case, only the study with a greater number of patients was included.
Outcomes
The primary outcome studied was 1–2-year incidence of restenosis after endovascular treatment defined by Doppler. Secondary outcomes of interest were 1–2-year target lesion revascularisation and combined major adverse outcomes, which included death, target lesion revascularisation, surgical revascularisation and amputations. When major combined outcomes were not presented as defined it was calculated adding the individual outcomes.
Statistical analysis
Meta-analysis was performed according to recommendations of the Cochrane Collaboration and the Quality of Reporting of Meta-analyses (QUORUM) guidelines and PRISMA statement using Review Manager (RevMan) V.5.2 version (Copenhagen, Nordic Cochrane Centre, The Cochrane Collaboration, 2012).12 ,13 Pooled treatment effects were estimated using risk difference (RD) with the Mantel-Haenszel method. We calculated the number needed to treat (NNT) according to the recommendations of the Cochrane Collaboration.13 Heterogeneity was assessed using χ2 tests and I2 statistic; we defined I2 <25% as low heterogeneity according to the Cochrane Handbook of Systematic Reviews. We performed fixed effect analysis when I2 was less than 25% or p value at least 0.10; otherwise we used random effect. We assessed quality for each included trial according to the methods of the Cochrane Collaboration.13 All included studies were controlled trials and were considered high quality.
Results
The process of study selection is shown in figure 1. Initial MEDLINE search using a systematic approach yielded 205 studies. The search in EMBASE and Cochrane registries did not yield additional studies. Through a review of titles and abstracts, 173 studies were rejected due to lack of relevance to our meta-analysis. The remaining 32 articles were reviewed and assessed for satisfaction of the inclusion or exclusion criteria. Three studies met all criteria and were included in this analysis.

Studies selection.
The first study14 had a follow-up period of 24 months and compared cilostazol/aspirin with ticlopidine/aspirin in 200 patients with femoropopliteal lesions. At 12 and 24 months, the cilostazol/aspirin group reduced restenosis rates (18% vs 43% and 27% vs 52%, respectively). A smaller study in 200915 also found similar results with restenosis rates (43% vs 70.3%). These findings were validated in a larger multicentre study in 2013 with 200 patients16 that demonstrated an angiographic restenosis rate at 12 months of 20% in cilostazol group versus 49% in the non-cilostazol group.
In order to obtain pooled estimates, a total of 396 patients were included in this analysis. Following EVT for femoropopliteal PAD lesions, 195 individuals were treated with cilostazol and standard medical therapy, whereas 201 received standard medical therapy alone, which included aspirin and a thienopyridine. The main characteristics of individual studies can be found in table 1. Of note, stent restenosis by Doppler was defined as a peak systolic velocity ratio >2.4 in Iida et al14 and Soga et al15 and >2 in Iida et al.16
Characteristics of studies included in the meta-analysis
Table 2 illustrates baseline characteristics of populations in the individual studies. All baseline variables including stenting ratio were similar in all studies with the exception of preprocedural Ankle Brachial Index (ABI) in Iida et al16; despite both groups having the ABI on the moderate disease range it was higher on the cilostazol group (0.71 vs 0.66).
Baseline characteristics in individual studies
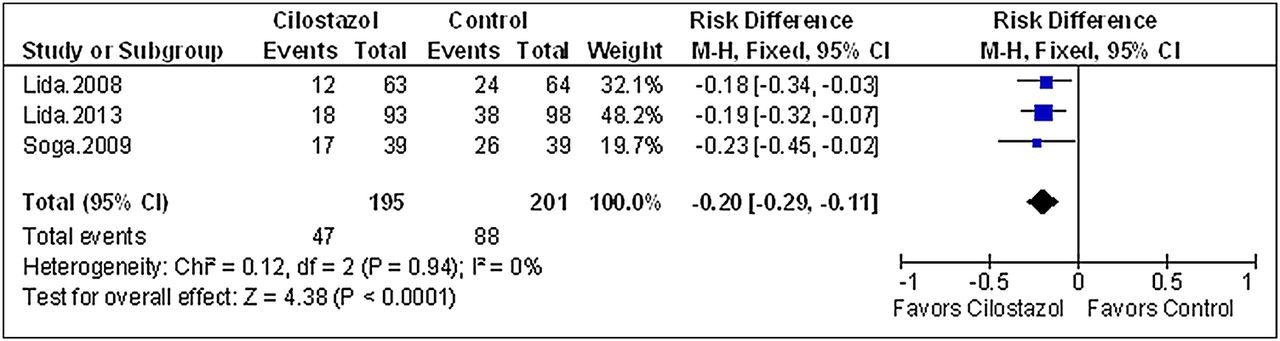
For the primary outcome, as seen in figure 2, the follow-up revealed a significantly reduced incidence of restenosis in patients who received cilostazol in addition to standard medical (RD −0.20; 95% CI −0.29 to −0.11; p<0.0001; NNT 5). This was reflected on a reduced need for target lesion revascularisation (RD −0.17; 95% CI −0.25 to −0.09; p<0.0001; NNT 6) with a NNT of 5 for both outcomes (figure 3). We also conducted a sensitivity analysis utilising OR as the primary pooled estimate and the effect size did not change. Death and amputations did not statistically differ between the two groups.

Twelve-month to 24-month incidence of restenosis.

{kind=link}
{kind=link}
{kind=link}
Twelve-month to 24-month incidence of target lesion revascularisation.
Discussion
The potential benefit of cilostazol following EVT for femoropopliteal PAD was investigated in this study. Our meta-analysis of RCTs revealed that 75 of 201 patients not treated with cilostazol have developed restenosis within 12–24 months and that the chance of restenosis may be mitigated in more than 50% with cilostazol. This result is particularly significant when taken into account that cilostazol is a generic and inexpensive drug that has been shown to be a cost-effective drug in other clinical scenarios, such as treatment of intermittent claudication and secondary prevention of cerebral infarction9 ,10 and that the benefit is obtained with a small NNT.
One-year incidence of restenosis after balloon angioplasty of femoropopliteal lesions has been reported as high as 64%.17 ,18 Sirolimus-eluting stents19–21 and endovascular brachytherapy22 ,23 have failed to demonstrate a long-term decrease in the restenosis incidence following lower extremity EVT for PAD, but paclitaxel-eluting stents have shown increased patency and a lower rate of events.23 Nevertheless, patency has greatly improved since the introduction of nitinol stents.18 ,24 When compared to percutaneous transluminal angioplasty, the use of nitinol stenting decreased the 12-month restenosis incidence from 81.3% to 36.7% in a RCT.18 Nevertheless, the results of this meta-analysis suggest that patency rates can be further increased with cilostazol in addition to nitinol stents, given that stent use did not differ among cilostazol and control groups, as illustrated in table 2.
Cilostazol has been shown to decrease restenosis and repeat revascularisation after percutaneous coronary intervention in patients with coronary artery disease, without an increased bleeding risk.25 Similarly, in this meta-analysis, target lesion revascularisation occurred in about every third patient on the control group over a 12–24 month follow-up. The chance of requiring a repeat target lesion revascularisation was reduced in more than 60% with the use of cilostazol. The combined incidence of death, revascularisation and amputation was also significantly reduced in the cilostazol group but it was mostly driven by the reduced need for revascularisation.
The main mechanism for cilostazol-mediated decrease in restenosis and target lesion revascularisation after EVT is likely inhibition of intimal hyperplasia. Cilostazol has been shown to suppress neointimal hyperplasia in animal models.26 ,27 Furthermore, RCTs have demonstrated that triple antiplatelet therapy with aspirin, clopidogrel and cilostazol was more effective than dual therapy alone in suppressing intimal hyperplasia.28 A second mechanism for improved outcomes in the cilostazol group is vasodilation. Studies have shown that cilostazol increases walking distance in patients with PAD and improves ankle-brachial index due to vasodilation.29–31 Moreover, cilostazol mediates an in-vitro inhibition of smooth muscle cell proliferation.32 Whether this effect contributes to improved EVT procedural outcomes is unknown. Cilostazol also inhibits platelet aggregation.
This meta-analysis has some limitations. Owing to the limited number of studies the sample size is small. However, despite the limited sample size, our meta-analysis represents the best available evidence for the use of cilostazol to increase femoropopliteal patency after endovascular intervention. As with any meta-analysis, our study is subject to publication bias that is potentially mitigated by the exclusive use of RCTs. Although the time frame of outcomes varied from 12 to 24 months, most cases of restenosis following EVT for femoropopliteal lesions occurred from 6 to 12 months,33 a time frame that was included in this study. The available data are exclusively from Asian populations and it is possible that our results apply exclusively to Asian populations, but that is unlikely due to prior positive cilostazol studies in other populations. Finally, regarding the antiplatelet properties of cilostazol, bleeding complications could not be assessed given that this outcome was not reported in all included studies and this could be considered to be an important limitation of our analysis. Only Soga's study attempted comparing major bleeding in dual versus triple therapy but no patients had events. Although not reported in these studies, there is robust evidence that when cilostazol is used in combination with dual antiplatelet therapy for other indications, there is no increased risk of bleeding compared to dual antiplatelet therapy alone. For example, in an RCT with patients with acute coronary syndrome undergoing stenting, triple therapy had similar bleeding events compared with dual antiplatelet therapy.34
In summary, in our meta-analysis of RCTs, cilostazol following endovascular treatment for femoropopliteal PAD was shown to significantly reduce restenosis, target lesion revascularisation and combined adverse outcomes when compared to a standard therapy control group. Large RCTs are urged to confirm our findings.
References
Footnotes
-
Contributors AMB, DCG, JSJ and TC were involved in the conception and study design. AMB, JSJ, RMNC and TPM were involved in the literature review. GEE-H, GNN, EFA and JJD were involved in the data collection. GNN, GEE-H, EFA and TPM were involved in the statistical analysis. AMB, DCG, GNN and TC were involved in the revising manuscript critically for important intellectual content. AMB, DCG, RMNC, TPM, GEE-H, GNN, EFA, JJD and TC were involved in the final approval of the manuscript submitted.
-
Competing interests No authors have any relationship with industry related to this manuscript.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.