Article Text

Abstract
Background Left ventricular (LV) size is an important clinical variable, commonly assessed at echocardiography by measurement of the internal diameter in diastole (IDD). However, this has recognised limitations and volumetric measurement from apical views is considered superior, particularly with the use of echocardiographic contrast. We sought to determine the agreement in classification of LV size by different measures in a large population of patients undergoing echocardiography.
Methods and results Data were analysed retrospectively from consecutive patients (n=2008, 61% male, median 62 years) who received echocardiographic contrast for LV opacification over 3 years in a single institution. Repeat studies were not included. LVIDD was measured, and LV end-diastolic volume (LVEDV) calculated using Simpson's biplane method. Both measures were indexed (i) to body surface area and categorised according to the American Society of Echocardiography (ASE) guidelines as normal, mild, moderate or severely dilated. Of 320 patients with a severely dilated LVEDVi, only 95 (30%) were similarly classified by LVIDD, with 86 patients (27%) measuring in the normal range. LVIDDi agreement was poorer, with only 43 patients (13%) classified as being severely dilated, and 173 (54%) measuring in the normal range.
Conclusions Currently recommended echocardiographic measures of LV size show limited agreement when classified according to currently recommended cut-offs. LV diameter should have a limited role in the assessment of LV size, particularly where a finding of LV dilation has important diagnostic or therapeutic implications.
- VALVULAR DISEASE
- HEART FAILURE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this subject?
-
Standard echocardiographic methods to assess left ventricular (LV) size involve measuring the LV diameter and volume; when contrast is used the latter correlates well with cardiac MRI.
What does this study add?
-
This retrospective study assessed more than 2000 patients to compare these two measures and their resulting classification of LV size. The main finding is that diameter frequently underestimates LV size compared with contrast-enhanced volumes, even when there is significant LV dilation.
How might this impact on clinical practice?
-
LV diameter should be used with caution as a measure of cardiac size. Volumetric assessment may be more appropriate particularly in heart failure and valvular heart disease for diagnosis, clinical decision-making and assessing response to therapy.
Introduction
Left ventricular (LV) size is standardly reported by measurement of the internal diameter in diastole (IDD) in patients undergoing echocardiography. It is quickly and easily obtained in the majority of patients and provides important diagnostic and prognostic information.1–3 In some conditions, such as valvular heart disease, the LV dimension is important for assessing severity and guiding the timing of surgical intervention.4–6 Nevertheless, there are limitations of the LV diameter which are well recognised.7 This may be underestimated if the image plane or the measured diameter is not properly aligned through the short axis of the ventricle. Variability between readers in terms of where the measure is made can result in inconsistent reporting, particularly if serial assessment is required. Finally, the LV diameter is a relatively crude and simplified assessment of a three-dimensional structure, which cannot take into account more complex variations in ventricular shape or size.8 ,9
For these reasons, alternative means of assessing LV size are recommended. Using orthogonal long-axis views, Simpson's biplane method allows a more accurate calculation of the LV volume, which may be corrected for patient size by indexing to body surface area (BSA).10 This technique relies on good apical image quality to visualise endocardial borders, but in cases where this is suboptimal, endocardial definition can be enhanced considerably with the use of an intravenous ultrasound contrast agent. The use of Simpson's biplane measure with echocardiographic contrast has been shown to provide a more accurate assessment of LV volume compared with cardiac MRI.11–15 Despite this, contrast volume measurements are not obtained in the majority of cases, and LV diameter continues to be recommended for reporting as a measure of LV size in European and American guidelines.16 ,17 However, the relationship between these different measures has not been previously investigated.
The primary aim of this study was to assess the consistency of different measures of LV size obtained during a single echocardiographic examination, in a large cohort of patients receiving echocardiographic contrast for clinical purposes.
Methods
Data were analysed retrospectively from 2211 consecutive patients who received echocardiographic contrast for LV opacification, out of a total population of 28 227 undergoing echocardiography over 3 years from January 2010 to December 2012, in a single institution. Two hundred and three studies were excluded from analysis in patients who had repeat contrast echocardiography during this time, to avoid duplication in specific patient groups (eg, inpatients with severe heart failure). The resulting study population numbered 2008 patients.
Echocardiographic contrast (Definity, Lantheus Medical Imaging, N. Billerica, Massachusetts, USA) is routinely administered in this institution in the following circumstances: (1) to enhance endocardial border definition when accurate calculation of LV volumes and ejection fraction (LVEF) is required, (2) for improved visualisation of regional wall motion where two or more segments are not clearly seen, (3) for assessment of ventricular thrombus or (4) for clarification of apical pathology. Volume measurements are not routinely performed on non-contrast images due to potential difficulty in visualising endocardial borders and inaccurate quantification.
Patients were scanned on a Phillips iE33 platform using either an S5-phased or X5-phased array transducer. Images were obtained from standard parasternal and apical windows. The LV end-diastolic diameter was measured from two-dimensional (2D) images in the parasternal long-axis view, timed with mitral valve closure at the level of the mitral valve chordae.
All patients received echocardiographic contrast at the discretion of the reporting cardiologist for the indications previously described; 0.2–0.3 mL of contrast was diluted to 10 mL in normal saline with incremental 1 mL intravenous injection. Contrast images were obtained using a low mechanical index power modulation setting. Images were acquired with complete filling of the LV to minimise apical swirling artefacts and attenuation of basal segments. Standard apical four-chamber and two-chamber views were recorded with care taken to align the true long axis of the ventricle. LV volumes and LVEF were calculated by Simpson's biplane method, following manual delineation of the endocardial border in the largest (end-diastolic) and smallest (end-systolic) frames.
Patients’ height and weight were documented and BSA calculated using the Mosteller formula.18 Measures of LV size were indexed (i) to BSA and classified according to cut-offs from the American Society of Echocardiography (ASE) Chamber Quantification Guidelines as normal, mild, moderate or severely dilated.10 All echocardiograms were performed by American Registry for Diagnostic Medical Sonography (ARDMS) registered sonographers, with LV diameter and volume measures performed and reported according to ASE criteria by cardiologists with level 2 or level 3 certification. The study protocol was reviewed and approved by the Health Research Ethics Board at the University of Alberta, ID Pro00037315.
Statistics
Normally distributed data are presented as mean±SD, or where skewed as median and IQR. Normality was assessed using the Kolmogorov-Smirnov test. Sex-related differences in patient characteristics were determined using the Mann-Whitney U test. Correlations of LV diameter and volume indices were calculated using Spearman's r, and agreements in classifications of LV size were assessed using Cohen's κ. Comparisons of patient characteristics in different quartiles of LV end-diastolic volume index (LVEDVi) were compared using the Jonckheere-Terpstra test and the χ2 test for trend (for categorical variables). SPSS V.21 (IBM Corp, Armonk, New York, USA) was used for all analyses.
Results
The study population was predominantly male (61%) with a median age of 62 (53–72) years (table 1). Male patients tended to be older (64 vs 59 years) with a larger LV diameter (5.4 vs 4.6 cm) and LV indexed volume (72 vs 58.5 mL/m2) but lower ejection fraction (45% vs 60%). However, there was no difference in LV indexed diameter between men and women.
Study population characteristics
When assessed by quartiles of LV volume index, patients with larger ventricles had lower ejection fraction and lower body mass index (table 2). However, there was no significant relationship with age or BSA among quartiles of LV volume index.
Characteristics of the cohort by quartile of LVEDVi
Correlation of LV diameter with LV volume index
There was a strong correlation between LVIDD and LVEDV, (r=0.74, p<0.001). However, when correlated with LVEDVi, the relationships were more modest (r=0.63 and 0.61 for LV diameter and LV indexed diameter, respectively). For each measure the correlation was weaker in women (table 3).
Correlations of measures of LV size with LVEDVi
Classification of LV size
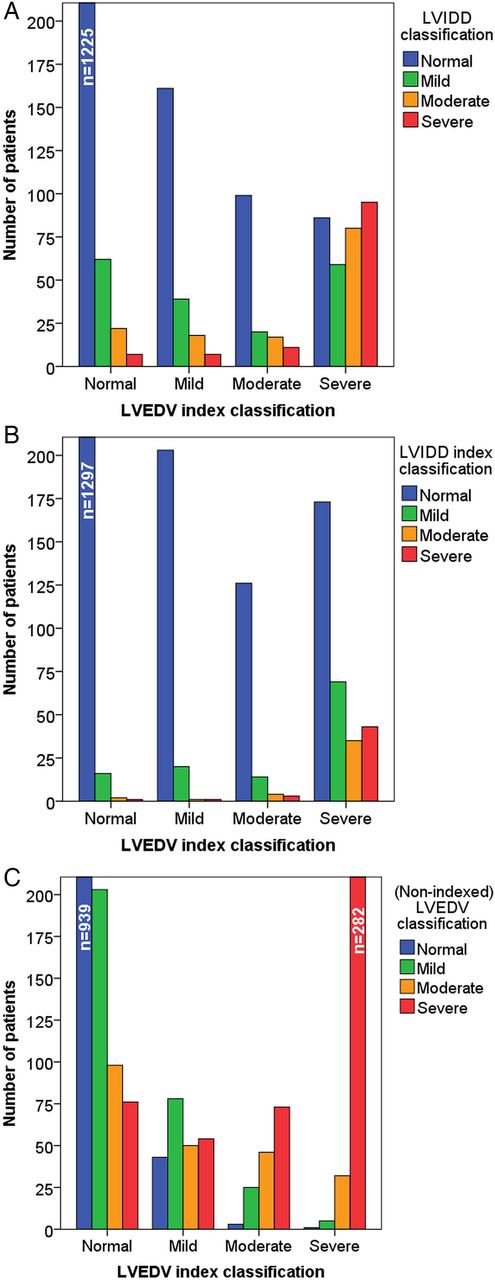
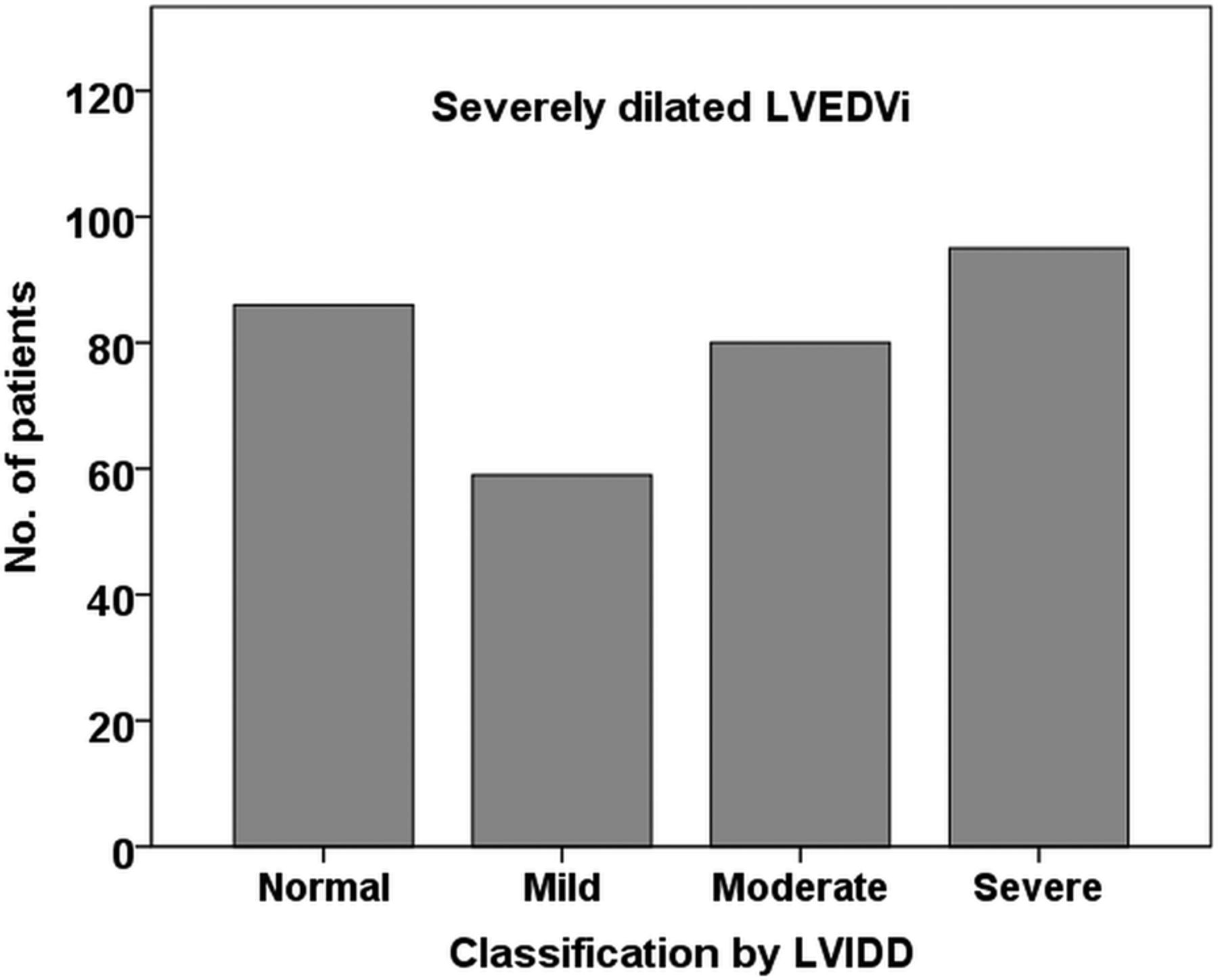
Measures of LV size were categorised as normal, mild, moderate or severely dilated according to ASE defined cut-off values for LV diameter, LV indexed diameter, LV volume and LV indexed volume. When each measure was compared with LVEDVi, there was only limited agreement in classification of LV size (table 4 and figures 1A–C). Of 320 patients with a severely dilated LVEDVi, only 95 (30%) were similarly classified by LVIDD, with 86 patients (27%) measuring in the normal range (figure 2). LVIDD index agreement was poorer, with only 43 patients (13%) classified as being severely dilated, and 173 (54%) measuring in the normal range.
Classification of LV dilation by different measures of LV size
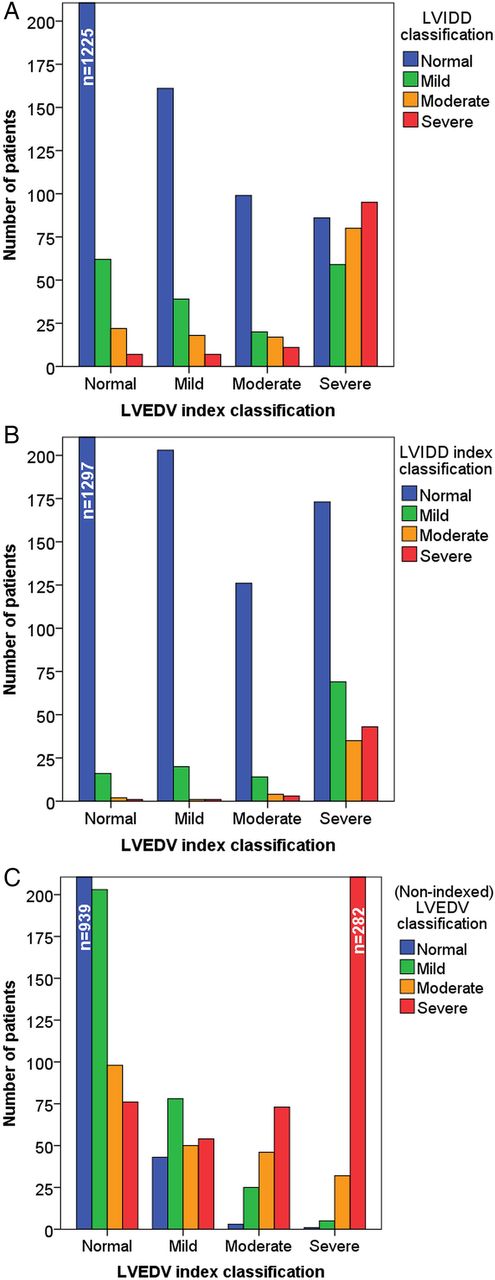
Classification of left ventricular (LV) size by (A) LV internal diameter in diastole (LVIDD) according to LV end-diastolic volume index (LVEDVi), (B) LVIDD index (LVIDDi) according to LVEDVi and (C) LV end-diastolic volume (LVEDV) according to LVEDVi.
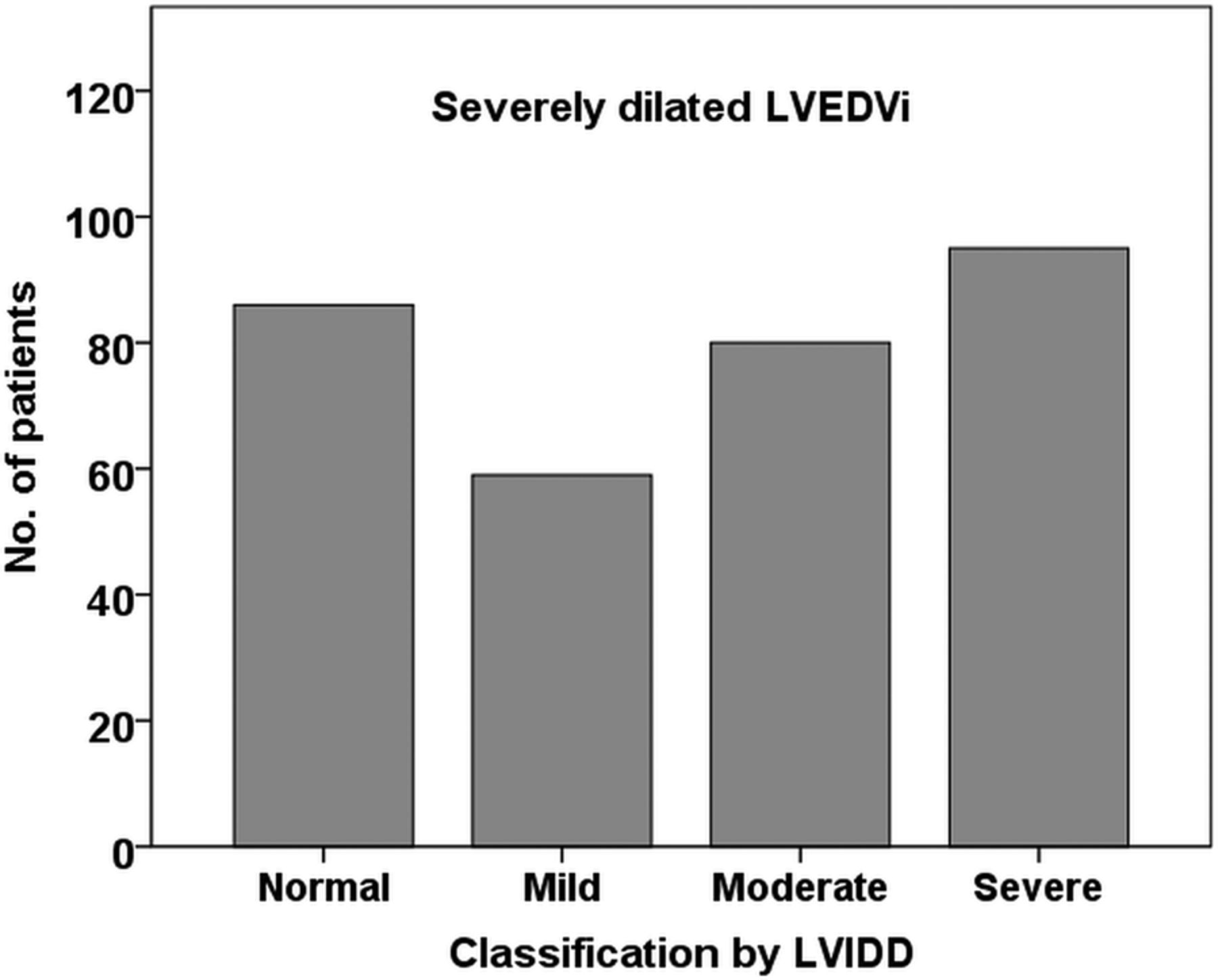
Classification of patients with severely dilated left ventricular end-diastolic volume index (LVEDVi) by LV internal diameter in diastole (LVIDD).
Assessing LVEDV, the classification agreement remained modest (κ=0.462). However, non-indexed volumes demonstrated an increased tendency to diagnose LV dilation with respect to indexed volumes: of 485 patients classified with a severely dilated LV volume, 76 (16%) had an indexed volume in the normal range.
When LV size was defined more simply as normal or dilated by the same criteria, there was similarly poor agreement in classification (table 5). Of 692 patients with a dilated indexed LV volume, 346 (50%) had an LV diameter in the normal range, and 502 (73%) had a normal indexed LV diameter. Agreement remained limited between indexed and non-indexed LV volumes (κ=0.580), again due to an increased likelihood of being classified as dilated by non-indexed volumes. Of 1022 patients with a dilated (non-indexed) LV volume, 377 (37%) had an indexed volume in the normal range.
Classification of LV (normal or dilated) by different measures of LV size
Discussion
This study demonstrates a marked discrepancy in recommended measures of LV size obtained by echocardiography in a large cohort of patients receiving contrast for clinical purposes. There is only modest correlation between LV diameter and LV indexed volume, and poor agreement in classifications of LV size; LV diameter, even when indexed, is frequently within the normal range even when the indexed volume is severely dilated (figure 3). Conversely, non-indexed LV volumes are more likely to be above the reference range than when indexed to BSA.

{kind=link}
{kind=link}
{kind=link}
Measures of left ventricular (LV) size obtained in a 36-year-old man, body surface area 2 m2. LV internal diameter in diastole measured in the normal range (5.6 cm); indexed volume was severely dilated (LV end-diastolic volume (LVEDV) 200 mL, LVEDV index (LVEDVi) 100 mL/m2).
LV size—diameter or volume?
Accurate assessment and classification of LV volumes is central to the practice of cardiology. Diastolic and systolic volumes determine ejection fraction, which remains the cornerstone measurement of LV systolic function.19 However, there are particular circumstances where LVEDV alone is an important diagnostic and prognostic measure. Ventricular dilation may be an early marker of disease in patients with dilated cardiomyopathy20 or undergoing follow-up for treatment with cardiotoxic therapy.21 Increasing LV cavity size portends worsening prognosis with adverse remodelling after myocardial infarction.22 Conversely a reduction in LV size is associated with improved outcome following cardiac resynchronisation therapy.23 The clinical importance of LV size (measured by end-diastolic diameter) is emphasised in guidelines for timing of surgery in patients with valvular heart disease.5 ,6
As such, the European Association of Echocardiography mandates reporting of LV dimensions in transthoracic echocardiography, with volumetric assessment advised by Simpson's biplane method when ejection fraction is calculated.16 The ASE recommendations list either LV dimensions or volumes as acceptable in a standard transthoracic report, with a descriptive comment regarding the classification of cavity size.17
Historically, measures of LV size and systolic function were obtained at echocardiography by M-mode from the parasternal long-axis window.24 With advances in ultrasound technology resulting in improved 2D images the benefits of increased temporal resolution with M-mode have become less important for this purpose, and given the potential inaccuracy of M-mode interrogation where the ventricle lies ‘off-axis’, LV diameter may be more reliably measured from standard 2D images.7 However, even when attention is paid to optimise settings, the technique may be susceptible to poor parasternal echocardiographic windows with reduced image quality leading to difficulty distinguishing endocardial borders.25 Furthermore, the technique retains the limitations of significant geometric assumption when extrapolated as a measure of true cavity size.
In the current era several imaging modalities are available for LV volume measurement, varying in accuracy, time, cost and radiation exposure. The use of CT and cardiac MRI has increased significantly in recent years for many reasons, including a strong body of evidence demonstrating their potential for accurate and reproducible evaluation of LV volumes and LVEF.26–32 Despite this increase in tomographic imaging, echocardiography remains the fastest and most accessible method. The availability of echocardiographic contrast allows for accurate assessment in the majority of patients even with poor echocardiographic windows.33 Previous studies have demonstrated that LV volumes obtained using Simpson's biplane calculation with contrast are more accurate than non-contrast images, with acceptable limits of agreement when compared with cardiac MRI.11 ,13–15 The technique requires increased study time for intravenous injection, additional imaging and offline tracing of endocardial borders. Nevertheless, routine contrast administration is usually feasible without significant disruption34 and should be considered where endocardial definition is suboptimal, or where accurate calculation of ventricular volumes or LVEF is required.35
Classifying LV size
Defining normal values for ventricular size is important for the standardisation of echocardiographic reporting, but is not a straightforward task. Normal and abnormal ranges depend on a number of factors including populations studied, methods used for imaging and the statistical approaches employed. Hence the ranges published in the ASE Guidelines for Chamber Quantification are ultimately determined by expert consensus, incorporating accumulated data from population distributions, and evidence regarding associated risk stratification.10
While the relation between LV diameter and volume is imperfect, the relative cut-offs for LV diameter and LV indexed volume may be a further significant factor in the discrepancies observed in classification according to each measure. A relatively high cut-off for normal LV diameter would explain in part why so many patients with a severely dilated indexed volume have a diameter in the normal range. However, it is important to recognise that the cut-off values used for ventricular volumes were obtained before the development of echocardiographic contrast.36 It has been demonstrated previously that volumes obtained using Simpson's biplane method with contrast are between 10 and 47 mL higher than with non-contrast images13–15 with the degree of discrepancy depending on the population assessed. This will increase the likelihood of having a dilated (indexed) volume when defined by currently recommended cut-off values, and might explain some of the discrepancy seen in the present study population. Indeed, with the increasing use of contrast to calculate LV volumes and LVEF, there is a need to re-establish normal and abnormal values obtained by this method. Recent advances and increased utilisation of three-dimensional echocardiography should also contribute to this field.
In this cohort, 37% of patients with dilated non-indexed volumes were classified as normal after accounting for BSA. This highlights the significance of indexing to BSA as well as the difficulty of ascribing corresponding reference ranges to indexed and non-indexed measures of LV size. In general, where volumes are used, indexing for BSA is standard practice.
While challenges remain in defining normal and abnormal ranges, the existence of large registries of patients undergoing echocardiography, combined with improved facility to obtain relevant outcome data should encourage continued efforts to refine the cut-off values for use in everyday practice.
Strengths and limitations
This study investigated measures obtained from a large population of patients undergoing clinically indicated echocardiography with contrast in a high-volume centre. It therefore represents a “real world” population and as such the results may be considered clinically applicable. Nevertheless there are some limitations which should be acknowledged. This is a retrospective analysis, with measures obtained by a variety of sonographers and reporting echocardiologists. However, image acquisition and reporting within the department are standardised as far as possible according to current ASE guidelines.10
Although normal ranges for indexed volumes were previously defined without contrast, data is lacking from this cohort to compare volumes obtained from corresponding non-contrast images. However, such analysis is not routinely performed in this institution. Likewise, data is not presented regarding measures of LV diameter with contrast; there is no good evidence to support its use for this purpose. By including only patients who were administered contrast, it is likely that the study population was preselected with poorer baseline apical image quality. Where contrast was administered for accurate LVEF calculation, a corresponding bias towards patients with LV dilation may have increased the frequency or degree of discrepancy between the different measures compared with the population undergoing echocardiography as a whole. However, it should be noted that 1571 patients (78%) had an LV diameter in the normal range. Furthermore, inclusion of patients with larger ventricular size allows a more robust assessment of the relationship between LV diameter and LV indexed volume in this group. Finally, the accuracy of LV volumes obtained in this study cannot be reliably assessed as there was no ‘gold standard’ for reference in this population. However, previous studies have shown good agreement of LV volumes measured by contrast echocardiography and MRI, and the primary aim of this study was to assess the consistency of classification by different measures obtained at the same echocardiographic investigation.
Conclusion
Currently recommended echocardiographic measures of LV size show limited agreement when classified according to cut-offs as recommended in ASE guidelines. In particular, a significant proportion of patients with LV dilation assessed by Simpson's biplane with contrast are not detected by measuring diameter alone. This study demonstrates the need at least to reassess the cut-offs for normal LV diameter in a large patient cohort, and previous studies which have cemented the role of LV diameter into clinical practice and management guidelines may need to be revisited. Ultimately, in the era of volumetric assessment, LV diameter should have an increasingly limited role in the assessment of LV size, particularly where a finding of LV dilation has important diagnostic or therapeutic implications.
References
Footnotes
-
Funding HB is supported by a grant from the Heart & Stroke Foundation of Alberta, North West Territories and Nunavut.
-
Competing interests HB reports non-financial support from Lantheus during the conduct of the study and personal fees from Bracco and Acusphere outside the submitted work. JBC reports grants from Philips Healthcare outside the submitted work.
-
Ethics approval Health Research Ethics Board at the University of Alberta.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.