Article Text

Abstract
Objectives To examine the relationship between periprocedural bleeding complications and major adverse cardiovascular events (MACEs) and mortality outcomes following percutaneous coronary intervention (PCI) and study differences in the prognostic impact of different bleeding definitions.
Methods We conducted a systematic review and meta-analysis of PCI studies that evaluated periprocedural bleeding complications and their impact on MACEs and mortality outcomes. A systematic search of MEDLINE and EMBASE was conducted to identify relevant studies. Data from relevant studies were extracted and random effects meta-analysis was used to estimate the risk of adverse outcomes with periprocedural bleeding. Statistical heterogeneity was assessed by considering the I2 statistic.
Results 42 relevant studies were identified including 533 333 patients. Meta-analysis demonstrated that periprocedural major bleeding complications was independently associated with increased risk of mortality (OR 3.31 (2.86 to 3.82), I2=80%) and MACEs (OR 3.89 (3.26 to 4.64), I2=42%). A differential impact of major bleeding as defined by different bleeding definitions on mortality outcomes was observed, in which the REPLACE-2 (OR 6.69, 95% CI 2.26 to 19.81), STEEPLE (OR 6.59, 95% CI 3.89 to 11.16) and BARC (OR 5.40, 95% CI 1.74 to 16.74) had the worst prognostic impacts while HORIZONS-AMI (OR 1.51, 95% CI 1.11 to 2.05) had the least impact on mortality outcomes.
Conclusions Major bleeding after PCI is independently associated with a threefold increase in mortality and MACEs outcomes. Different contemporary bleeding definitions have differential impacts on mortality outcomes, with 1.5–6.7-fold increases in mortality observed depending on the definition of major bleeding used.
- ALLIED SPECIALITIES
- MYOCARDIAL ISCHAEMIA AND INFARCTION (IHD)
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Key messages
-
▸ The strength of this systematic review was the large number of studies included with over half a million total participants.
-
▸ Another strength was that we were able to evaluate the effect of different major bleeding definitions and its impact on risk of mortality and major adverse cardiovascular events.
-
▸ This systematic review had the limitation that studies included varied in antithrombotic and antiplatelet regimes after PCI procedure.
-
▸ Another limitation was that the systematic review was unable evaluate whether the subsequent mortality was directly related to the bleed.
Introduction
Advances in antithrombotic therapy have improved the outcomes of patients undergoing percutaneous coronary intervention (PCI) through the reduction of ischaemic events at the expense of increased procedure-related bleeding complications. Major bleeding events in contemporary PCI are significant, with 30-day bleeding event rates reported between 0.7% and 1.1% in elective,1–3 0.6% and 4.7%3–6 in non-ST-elevation myocardial infarction (NSTEMI) and 0.9% and 8.9% in ST-elevation myocardial infarction (STEMI)3 ,4 ,7 ,8 depending on the definition used.
There are currently around 10 different definitions of major bleeding used in trials and registries of patients undergoing PCI9 ,10 and these definitions include various clinical events, such as blood transfusion or retroperitoneal haemorrhage, laboratory parameters, such as differing values of haemoglobin decreases, and clinical outcomes such as mortality9 resulting in significant differences in bleeding event recording across clinical trials thereby making comparisons between therapeutic strategies difficult. Furthermore, the incidence of major bleeding varies depending on definition used. In one study, the RIVAL non-coronary artery bypass graft (non-CABG) related major bleeding occurred in 0.87% in the STEMI cohort and 0.57% in the NSTEMI group, while if an ACUITY major bleeding definition was used, major bleeding occurred in 3.1% in the STEMI group and 2.26% in the NSTEMI group, respectively.
Major periprocedural bleeding complications following PCI are predictors of mortality and major adverse cardiovascular events (MACEs),11–13 with up to 12.1% of all in-hospital mortality after PCI in the National Cardiovascular Data Registry's CathPCI Registry related to bleeding complications.14 In contrast, other studies have suggested that although bleeding may be causally related to adverse outcomes in some patients in the real-world setting, it is often merely a marker for patients at higher risk for adverse outcomes.15 ,16
Some prior studies that have reported on the prognostic impact of major bleeds have not accounted for differences in baseline covariates such as age, syndrome of presentation and comorbidities that would themselves impact on MACEs and mortality outcomes.17–21 In contrast, while other studies have adjusted for baseline covariates, different definitions of major bleeding such as TIMI,2 ,11 ,22 ,23 GUSTO,20 ,24 STEEPLE20 ,25 and BARC23 have been used, which have been shown to have differential impacts on mortality/MACEs outcomes.20 ,23 ,26 Furthermore, the timing of bleeding from index PCI procedures included in such studies has varied from 48 h,25 been limited to those that occur in hospital,23 ,27 to 30 days2 ,28 with impact on mortality and MACEs outcomes studied at different time points such as 30 days,8 ,24 ,28 6 months24 ,27 or 1 year.2 ,22 ,23 ,25
Until today, there has not been a systematic review or meta-analysis previously published studying the prognostic impact of periprocedural major bleeding events on mortality and MACEs outcomes following PCI. We have therefore undertaken a meta-analysis to systematically study the impact of major bleeding following PCI on mortality and MACEs outcomes. In this meta-analysis, we provide an overview of the cohorts evaluating the rates of major bleeding events and systematically study the differences in the prognostic impact of different bleeding definitions and the relationship between major bleeding and clinical events at different time points.
Methods
Eligibility criteria
We selected studies of patients who underwent PCI that reported on mortality or cardiovascular events among patients with and without major bleeding events. There was no restriction based on study design, definition of major bleeding or the indication for PCI or its status as an urgent or elective procedure. We excluded studies that did not report on categories of major bleeding and those that did not report either mortality or MACEs.
Search strategy
A search of EMBASE (1974 to January 2014) and MEDLINE (1946 to January 2014) was conducted on OvidSP. The search terms are shown in online supplementary figure S1. We did not use any language restrictions. We checked the bibliographies of included studies and relevant review articles found on the search for additional relevant articles.
Study selection and data extraction
Two reviewers (CSK and YKL) checked all titles and abstracts for studies that could potentially meet the inclusion criteria. We retrieved full reports of these potentially eligible studies and independently extracted data on study design, participant characteristics, interventions used, major bleeding events, follow-up, outcome events and methods of ascertaining measured clinical events on to a preformatted spreadsheet. Any discrepancies between the two reviewers were resolved by consensus after consulting a third reviewer (MAM).
Quality assessment
Risk of bias was assessed by considering four different areas: ascertainment of major bleeding events, ascertainment of outcome events, extent of loss to follow-up and the use of adjustment for confounders in the analysis. We also assess for publication bias using funnel plots when there were >10 studies available in the meta-analysis and there was no evidence of substantial statistical heterogeneity.29
Data analysis
We used RevMan V.5.1.7 (Nordic Cochrane Centre) to do random effects meta-analysis using the inverse variance methods for pooled ORs. We assumed similarity between the OR and other relative measures such as relative risk, rate ratios or HRs because cardiovascular events and death were rare events.30 The analysis was stratified based on whether the results had considered the effect of potential confounders through adjustments or propensity-matched cohorts or not. In order to reduce the risk of bias from confounding so that we have a more reliable estimate of the independent effect of bleeding on prognosis, we appraised studies with multivariate adjustments or propensity-matched cohorts separately from studies with crude or unadjusted results. We used adjusted or propensity-matched risk estimates where available. For datasets reporting multiple time points, we took the earliest time point for the primary analysis. Any later time points were subsequently analysed in the separate Forest plots stratified according to timing of outcome assessment. Where there were multiple definitions of major bleeding we choose to use the results for TIMI major bleeding.
We planned for three analyses. The primary analysis was the pooled adjusted and unadjusted risk of mortality with and without major bleed. The secondary analysis was the unadjusted and adjusted risk of MACEs with and without major bleed. In a post hoc sensitivity analysis, we conducted a pooled analysis after excluding studies where it was clear that only some (and not all) of the participants had undergone PCI.
Statistical heterogeneity
We used the I2 statistic to assess statistical heterogeneity. I2 Values of 30–60% represent moderate levels of heterogeneity.31
Results
Study selection
The process of selection of studies is shown in online supplementary figure S1. We retrieved 42 relevant studies of patients that underwent PCI (total number of participants 533 333), which evaluated the risk of adverse events with and without major bleeding.2 ,8 ,11 ,14 ,17–23 ,27 ,28 ,32–58 The number of participants in each study ranged from 352 to 280 390 and the number of major bleeding events was 66 277 (37 studies, 15.3%). A total of 40 studies evaluated mortality as an outcome and 11 studies reported on MACEs.
Description of studies included
The study designs, date of study, country of origin and indication for PCI is shown in table 1. There were 12 studies (149 650 participants), which were post hoc analyses of randomised controlled trials and 1 matched observational study (280 390 participants). Of the studies that reported number of centres, there were more multicentre studies than single centre studies (n=17 and n=13). The age and gender of participants along with the antiplatelet and anticoagulant regimes used is shown in online supplementary table S1.
Study design, year of study, country of origin and participant inclusion criteria
Table 2 shows the timing of major bleeding, definition of major bleeding used in the individual studies and the incidence of major bleeding in each study. While many of the studies did not report when assessment for major bleeding took place (n=15), 15 of the studies clearly stated that they evaluated in-hospital major bleeding. The definitions of major bleeding also varied among the included studies and formal definitions of major bleeding included TIMI, GUSTO, STEEPLE, HORIZON-AMI, CRUSADE, BARC and REPLACE-2 definitions. These definitions are summarised in online supplementary table S2. Follow-up of patients in the studies included in this analysis varied from 48 h to more than 3 years. The impact of major bleeding on clinical outcomes was adjusted for baseline covariates in 22 studies (490 699 participants) while in 20 studies (42 634 participants) only unadjusted outcomes were reported.
Timing of bleeding, definition of major bleeding and follow-up
Quality assessment
Online supplementary table S3 shows the quality assessment for included studies. Ascertainment of bleeding and mortality varied from data collection from medical record reviews to prospective evaluation in trials where independent committees adjudicated bleeding and outcome events.
Major bleeding and risk of mortality at any time point
The impact of major bleeding on mortality outcomes was studied in 40 studies reporting outcomes in 525 691 patients. In total, 66 016 major bleeds were reported. Crude rates or risk estimates for mortality in individual studies are shown in online supplementary table S4. Mortality rate was 3595/62 036 (5.8%, 28 studies) in patients who sustained a major bleed and 8937/370 522 (2.4%, 28 studies) in patients not experiencing major bleeding complications.
Meta-analysis of these data demonstrated that the overall risk of mortality was significantly greater among patients who sustained major bleeding complications periprocedurally (figure 1). The risk estimate for mortality was significantly lower in the subgroup of studies, which adjusted for potential confounders (OR 3.31 (2.86 to 3.82), I2=80%, 491 565 participants compared to the OR calculated in those studies that did not adjust for baseline covariates; OR 6.75 (4.99 to 9.12), I2=62%, 34 126 participants).
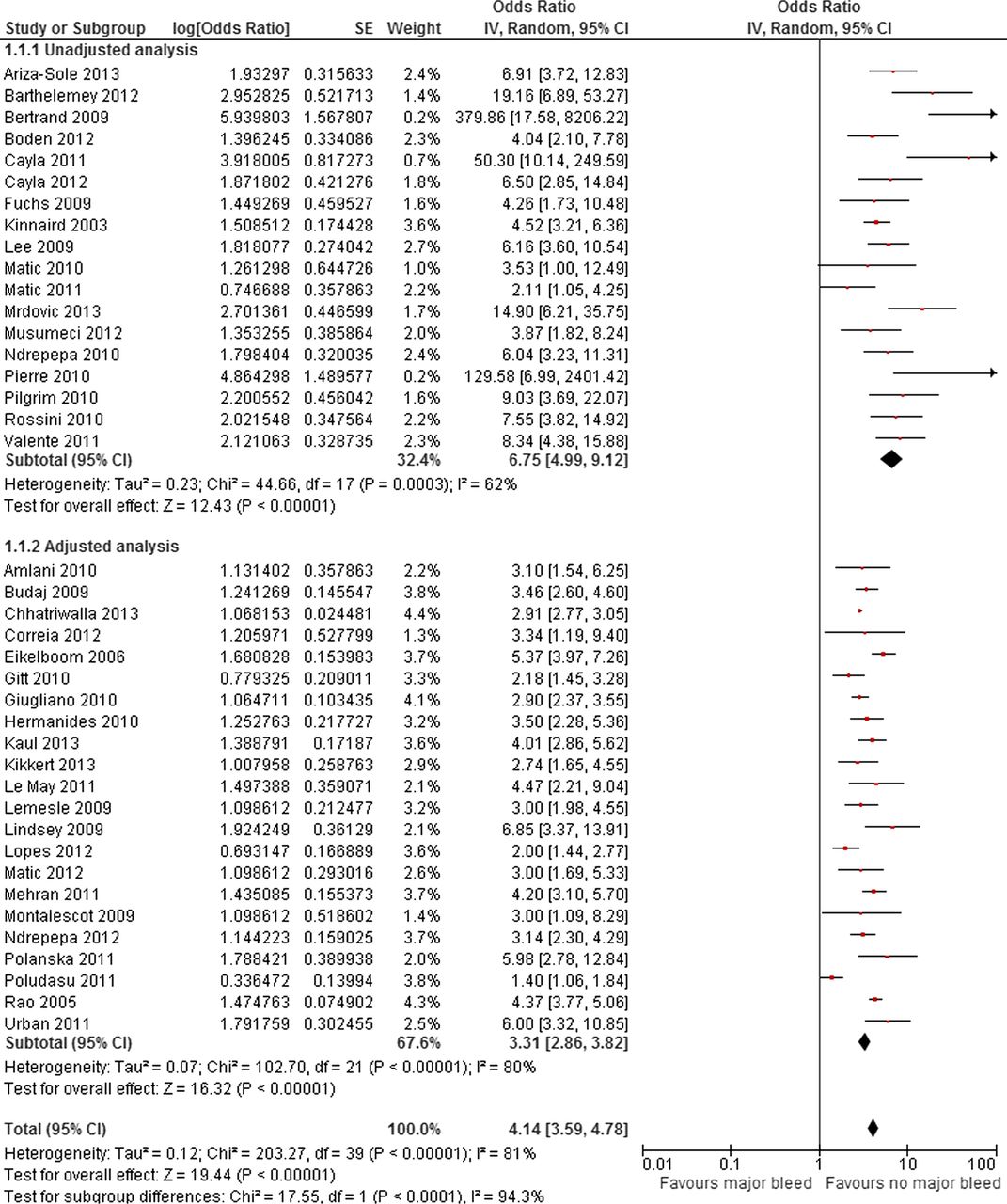
Adjusted risk of mortality with and without major bleed after percutaneous coronary intervention.
Major bleeding and risk of MACEs at any time point
The impact of major bleeding on MACEs outcomes was studied in 13 studies reporting outcomes in 69 843 patients. Crude rates or risk estimates for MACEs in individual studies are shown in tables 3 and 4; 757 major bleeds (6.8%) were reported.
Summary of risk of mortality and MACEs among patients with and without major bleed after percutaneous coronary intervention at different time points
Summary of risk of mortality and MACEs among patients with and without major bleed after percutaneous coronary intervention with different definitions of bleeding
MACE rates were 295/1701 (17.3%) in patients who sustained a major bleed and 2101/38 520 (5.4%) in patients not experiencing major bleeding complications. The overall risk of MACEs was significantly higher among patients with major bleeds (figure 2). The risk of MACEs did not significantly differ in the subgroup of studies that adjusted for baseline covariates (OR 3.89 (3.26 to 4.64), I2=42%, 25 829 participants as compared to those that did not adjust for baseline covariates OR 3.12 (2.32 to 4.19), I2=52%, 101 184 participants).

Adjusted risk of major adverse cardiovascular event with and without major bleed after percutaneous coronary intervention.
Mortality with major bleeding at different follow-up durations
The adjusted risk of mortality was significantly greater among patients with major bleeds at all time points evaluated (figure 3). For 30-day mortality, adjusted risk was OR 3.24 (2.73 to 3.84, I2=81%, 11 studies, 403 457 participants) and at 6 months, the OR remained elevated at 3.23 (2.92 to 3.57, I2=0%, 4 studies, 50 872 participants; table 3). At the 1-year time point, the risk of mortality was OR 3.64 (2.39 to 5.56, I2=89%, 9 studies).

{kind=link}
{kind=link}
{kind=link}
Risk of mortality with major bleed with different duration of follow-up.
MACEs with bleeding at different follow-up durations
Analysis of the impact of major bleeding on MACEs outcomes at different time points was stratified into risk of MACE <1 year and ≥1 year due to the limited number of studies presenting MACE data and its relationship with time. The adjusted risk of MACE <1 year was OR 3.96 (3.26 to 4.81, I2=53%, 2 studies, 47 422 participants) and for ≥1 year was OR 3.19 (1.89 to 5.37, 1 study, 3170 participants; table 3).
Adverse outcomes and different definitions for major bleeding
The impact of different definitions of major bleeding on mortality and MACEs outcomes are presented in table 4. REPLACE-2 (OR 6.69 (2.26 to 19.81), I2=84%, 3 studies, 17 996 participants) definition of major bleeding had the greatest impact on mortality outcomes, while the ACUITY/HORIZONS-AMI had the least impact (OR 1.51 (1.11 to 2.05), I2=12%, 1 study, 13 233 participants).
Sensitivity analysis
Sensitivity analysis excluding studies where not all participants had PCI did not significantly alter the pooled analysis for association between major bleeding and mortality (OR 3.16 (2.61 to 3.81), I2=75%, 372 449 participants).
Discussion
Advances in antithrombotic and antiplatelet therapy have improved outcomes following PCI through the reduction of ischaemic events although this has been at the expense of increased procedure-related bleeding complications. Our meta-analysis of 42 studies including over half a million patients confirms that major bleeding is independently associated with a threefold increase in mortality and MACEs outcomes, and that this increased mortality and MACEs risk observed following a major bleed is sustained for periods of over 1 year. We also show that major bleeding events as defined by different contemporary bleeding definitions have differential impacts on mortality outcomes, with 1.5–6.7-fold increases in mortality observed depending on the definition of major bleeding used.
There are a number of potential mechanisms that may underlie the relationship between major bleeding and adverse mortality outcomes. Patients that sustain major bleeding complications post PCI are more likely to be older, have renal failure, undergo PCI for STEMI/NSTEMI presentations, present with haemodynamic compromise or have a history of heart failure2 ,59 that also independently predict adverse mortality outcomes themselves. Many previous studies17–21 that have reported on the prognostic impact of major bleeds have not accounted for differences in such baseline covariates that are themselves known to impact on mortality outcomes, which would overestimate the mortality risks associated with a major bleed. For example, in an analysis from the Global Registry of Acute Coronary Events (GRACE), major bleeding was no longer associated with 6-month mortality after adjustment for the known comorbidities with the authors concluding that comorbidities associated with major bleeding accounting for the higher rate of mortality in patients who bled.15 Consistent with this, we have observed that in meta-analysis of studies that do not adjust for baseline covariates, major bleeding is associated with a sixfold increased risk in mortality, but this decreases to a threefold independent increase in mortality once baseline covariates are adjusted for, suggesting that major bleeding is independently linked to mortality and MACEs outcomes.
The potential mechanisms by which a major bleed adversely impacts on clinical outcomes are numerous. Major bleeds such as an intracranial haemorrhage or severe blood loss as can occur in a gastrointestinal haemorrhage may result in mortality directly, although such bleeding events would not explain the persistent mortality risk observed for over a year following a major bleeding event in our meta-analysis. Major bleeds may necessitate the discontinuation of antiplatelet or antithrombotic medications that increase the risk for stent thrombosis, a strong independent predictor of mortality outcomes in the short and longer term (>1 year).60 Furthermore, increased production of erythropoietin in response to anaemia that occurs following a major bleed may contribute to a prothrombotic systemic state beyond the acute phase through platelet activation and induction of plasminogen activator inhibitor-1 (PAI-1).61 ,62 Treatment with erythropoietin has been associated with increased risk of thrombosis in critical care patients63 and increase in the composite endpoint of death, acute myocardial infarction, stroke and stent thrombosis in patients with STEMI.64 Blood transfusions have been linked to adverse shorter and longer term mortality65 and have been shown to predict 30-day mortality66 independently of bleeding and haematocrit. Adverse mortality outcomes associated with blood transfusions occur through a number of mechanisms including prothrombotic effects mediated through acute platelet release of CD40 ligand,67 platelet activation and induction of PAI-161 an inhibitor of endogenous fibrinolytic mechanisms. These increased risks of mortality also extend to non-red blood cell transfusions such as platelets or plasma/cryoprecipitate that may also be utilised following a periprocedural major bleed.68
Our observations of a differential impact of different major bleeding definitions on mortality outcomes is particularly pertinent suggesting that the choice of bleeding definition used has significantly influenced the outcome of previous studies, since the definition employed will influence the prevalence of reported bleeds as well as their prognostic impact. For example, in the RIVAL study69 non-CABG related major bleeding as defined by the study was not significantly different between the radial and femoral arms of the study (OR=0.73, 95% CI 0.43 to 1.23; p=0.9), while use of the ACUITY major bleeding criterion was associated with a statistically significant reduction in major bleeding in the radial arm of the study (OR=0.43, 95% CI 0.32 to 0.57; p<00001). Similarly, in the SYNERGY trial that used the GUSTO and TIMI major definition of bleeding, the enoxaparin arm was associated with a significantly higher rate of major bleeding as defined by TIMI major criteria but no difference in major bleeding as defined by the GUSTO major definition. Definitions that encompass less severe bleeding events (such as the ACUITY definition) are not as strongly linked to adverse events and therefore may not be a powerful means of evaluating bleeding avoidance strategies. In order to prove efficacy for bleeding avoidance the use of a more discriminative definition would be preferable.
Our meta-analysis has a number of potential limitations. First, an inherent limitation of any meta-analysis is that of publication bias; studies that show a neutral outcome in mortality are less likely to be published than those that show a positive outcome and thus tend to bias any meta-analysis of published data towards a more positive outcome. Second, studies included in this meta-analysis often used different antithrombotic and antiplatelet regimes for the PCI procedures undertaken for different indications, hence it is unclear whether the prognostic impact of a major bleed differs with different antiplatelet/anticoagulant combinations or whether it differs in the elective/acute coronary syndrome setting. Finally, our current analysis does not provide insight into whether the timing of the major bleed in relation to the index PCI procedure has a differential impact on mortality outcomes.
In conclusion, our meta-analysis of 42 studies including over half a million patients has revealed that major bleeding is independently associated with a threefold increase in mortality and MACEs outcomes, and that this increased mortality and MACEs risk observed following a major bleed is observed for periods of over 1 year. We also show that major bleeding events as defined by different contemporary bleeding definitions have differential impacts on mortality outcomes. Given the significant impact of major bleeding on mortality outcomes, formal bleeding risk assessment should be undertaken as part of the decision-making process for PCI procedures and bleeding avoidance strategies such as optimal pharmacotherapy and access site choice should be actively undertaken, particularly in those patients at highest baseline risk for bleeding complications.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors CSK, MAM and YKL contributed to planning, conduct and reporting of the work. SVR, PKM, BK, JN, PFL and MDB contributed to the interpretation of the findings and reporting of the work. MAM is the guarantor and was responsible for the overall content.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.