Article Text

Abstract
Background Concurrent cardiac diseases are frequent among elderly patients and invite simultaneous treatment to ensure an overall favourable patient outcome.
Aim To investigate the feasibility of combined single-session percutaneous cardiac interventions in the era of transcatheter aortic valve implantation (TAVI).
Methods This prospective, case–control study included 10 consecutive patients treated with TAVI, left atrial appendage occlusion and percutaneous coronary interventions. Some in addition had patent foramen ovale or atrial septal defect closure in the same session. The patients were matched in a 1:10 manner with TAVI-only cases treated within the same time period at the same institution regarding their baseline factors. The outcome was validated according to the Valve Academic Research Consortium (VARC) criteria.
Results Procedural time (126±42 vs 83±40 min, p=0.0016), radiation time (34±8 vs 22±12 min, p=0.0001) and contrast dye (397±89 vs 250±105 mL, p<0.0001) were higher in the combined intervention group than in the TAVI-only group. Despite these drawbacks, no difference in the VARC endpoints was evident during the in-hospital period and after 30 days (VARC combined safety endpoint 32% for TAVI only and 20% for combined intervention, p=1.0).
Conclusions Transcatheter treatment of combined cardiac diseases is feasible even in a single session in a high-volume centre with experienced operators.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
Percutaneous cardiac interventions, by their less invasive nature, enhance patient comfort, accelerate recovery time and shorten hospitalisation duration. They have proven to be a valid alternative to open heart surgery for different patient and disease subsets. This becomes particularly true among patients with coexisting cardiac diseases necessitating complex combined surgical management which puts them at an additional operative risk.1 ,2 With the introduction of transcatheter aortic valve implantation (TAVI), a long neglected population of surgically high-risk and inoperable patients gained access to effective treatment for aortic valve stenosis.3 Frequently, however, these elderly patients have concurrent coronary artery disease and/or atrial fibrillation, which are both associated with an independent adverse prognosis.4–6 The management of these patients should therefore cover concurrent heart diseases to ensure an overall favourable outcome after TAVI.7 Staged or simultaneous percutaneous coronary interventions (PCI) and TAVI have been shown to be safe and feasible in different series.8 ,9 We recently described a successful first case of simultaneous TAVI, PCI and percutaneous device closure of the left atrial appendage (LAA).10 LAA occlusion has been demonstrated to be at least equally effective to long-term warfarin therapy in preventing systemic embolism among atrial fibrillation patients11 and is commonly used as a substitute for anticoagulation among selected patients not suitable for chronic anticoagulation.12 On the other hand, patent foramen ovale (PFO) and atrial septal defects (ASD) are a documented source for systemic emboli13 and their percutaneous closure is feasible and effective in reducing paradoxical embolism.14–17 We sought to investigate the feasibility of simultaneous cardiac interventions including TAVI, PCI and LAA occlusion with or without PFO/ASD closure in an elderly comorbid population.
Methods
Patient population and justification of combined procedures
Ten consecutive cases were selected from a cohort of 400 patients with severe aortic stenosis allocated to TAVI by the decision of the heart team at the Swiss Cardiovascular Center of the Bern University Hospital between 2009 and 2012. Data were entered into a prospective registry and analysed according to the criteria of the Valve Academic Research Consortium (VARC).18 Patient characteristics were compared with a pool of 100 case–control patients to match every patient with a combined intervention to a control according to the Society of Thoracic Surgeons (STS) score. Given the prospective cohort study character, there were no formal exclusion criteria. The Bern TAVI registry is part of the Swiss TAVI registry and has been approved by the local and national ethics committees. The Bern registry for LAA occlusion is also approved by the local ethics committee. For each of the combined interventions, dedicated forms listing potential adverse events, that is, the risk of the respective procedure, were provided. With regard to the risk/benefit ratio of combined versus staged interventions and especially under the aspect of avoiding several hospitalisations and general anaesthesia, the combined approach was deemed patient friendly without increasing complications and therefore recommended to the selected patients of this study.
Data acquisition
Demographic and clinical characteristics, procedural data, adverse events and outcome data of in-hospital and follow-up periods were systematically collected. After 1 and 3–4 months, a standardised follow-up examination was performed. After 3–4 months, in addition to clinical and neurological examination, a transesophageal echocardiography (TEE) was performed to ensure correct seating and freedom of relevant thrombi of the LAA closure device. All events underwent adjudication by a team of an independent cardiac surgeon and an independent interventional cardiologist. Outcome is reported according to the VARC criteria.
Combined interventions
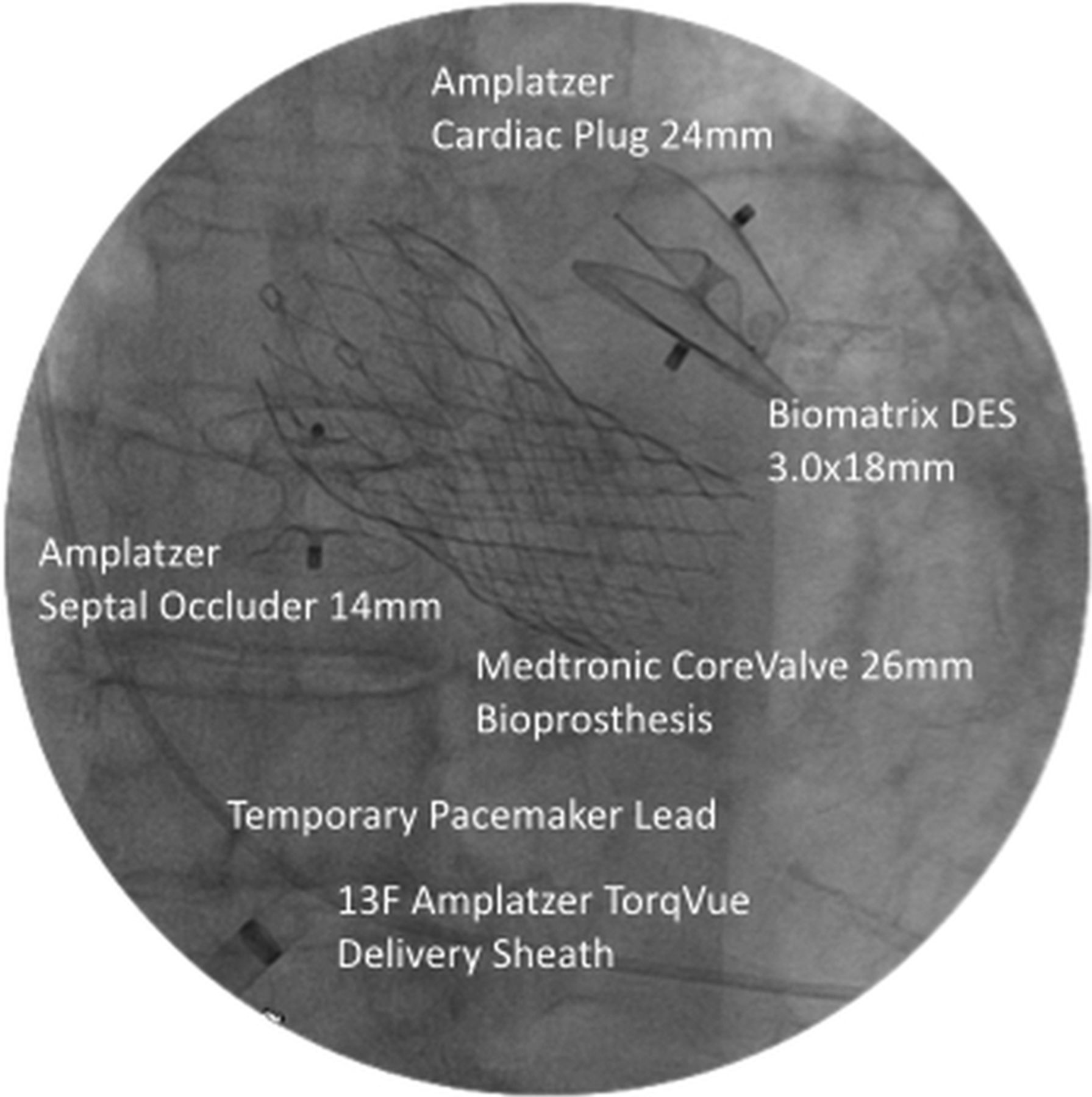
Beforehand, coronary angiography with invasive haemodynamic assessment, CT angiography (CTA) and TEE for aortic root assessment and exclusion of LAA thrombi were performed. Three of the 10 cases were transmitted live to international interventional courses. If indicated by angiographic stenosis degree, PCI was performed first by transfemoral access with 5 or 6 Fr guiding catheters and exclusively using drug-eluting stents (DES), which was the case in 6 of the 10 combined patients. Two did not suffer from CAD and in two, the CAD was treated earlier in a separate procedure. Next, TAVI was performed under mild sedoanalgaesia and inguinal local anaesthesia only via transfemoral access. A single or both femoral arteries were accessed and a suture-based vascular closure device preinstalled on the respective side of access for TAVI. Aortic stenosis was crossed using an Amplatzer left diagnostic catheter and a straight tipped wire. Via a stiff wire, balloon aortic valvuloplasty under rapid pacing (180/min) was performed. After advancement of a 16–20 F femoral sheath, the Edwards Sapien bioprosthesis (balloon-expandable titanium frame containing bovine pericardial leaflets) or Medtronic Corevalve bioprosthesis (self-expandable nitinol frame containing porcine pericardial leaflets in supra-annular position) was deployed. Selection of the device size was based on previous aortic root assessment by TEE, CTA or angiography. After TAVI, LAA exclusion and septal closure procedures followed on. In all cases the first generation Amplatzer Cardiac Plug (ACP) was used. Similar to TAVI, LAA occlusion was performed in a frugal manner without general anaesthesia or TEE guidance, that is, under fluoroscopy only: after accessing the left atrium through a trans-septal puncture or passage through a pre-existing PFO or ASD, the device size was selected based on biplane angiography of the LAA through the 9–13 F delivery sheath. After deployment, sustained tugging with the delivery cable tested ACP seating within the LAA and another biplane left atrial angiography was performed prior to the release. In case of unsatisfactory positioning or anchoring, the plug was recaptured and redeployed in a different angle or changed for a more suitable sized device. On the way back, a pre-existing PFO or ASD was closed by the same cable and delivery sheath using Amplatzer PFO or ASD occluders. After closure of the percutaneous arterial access and slight compression of the femoral vein, patients were posthydrated with normal saline according to the standard protocol and transferred to a cardiac intermediate care ward (see figures 1 and 2 for a representative course of action in case 2). Restart of oral anticoagulation was omitted. A dose of 75 mg of clopidogrel daily for 3–6 months and 100 mg of acetylsalicylic acid were prescribed indefinitely. For documentation of aortic bioprosthesis performance and exclusion of device displacement or pericardial effusion, transthoracic echocardiography was performed on day one after intervention and after 30 days. The patients were discharged on postprocedure days 3–7.
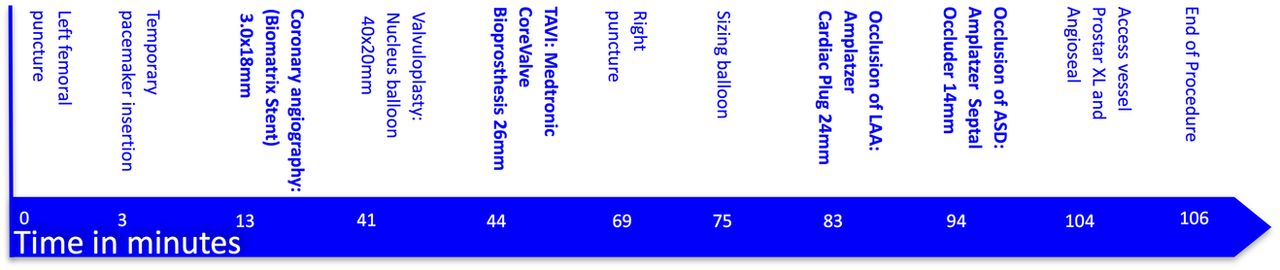
Representative course of action in case 2.
{kind=link}
{kind=link}
End result in case 2.
Matching and statistical analysis
For every combined case, 10 controls were selected from the database according to the most fitting STS score. Since the STS score contains all relevant patient characteristics and has been shown to be very accurate in predicting a 30-day outcome also in TAVI patients, it was deemed appropriate for matching. Continuous variables are presented as mean±SD and were compared using the unpaired Mann-Whitney U test. Categorical data are expressed as frequency (percentages) and were compared with Fisher's exact test. All tests and CIs are two-sided, and an α level of 0.05 was chosen to determine the statistical significance of differences. Analyses were performed using GraphPad Prism 6 (http://www.graphpad.com).
Results
Baseline characteristics and matching
Table 1 provides a brief description of each individual case and baseline characteristics are summarised in table 2. The rationale for LAA occlusion along with TAVI (5 with CoreValve, 5 with Edwards Sapien XT) and PCI were high bleeding risk in six and prior major bleeding in four patients. In 3 of the 10 patients, PFO closure (2) and ASD closure (1) were performed in addition. Matching could be performed with an excellent agreement (mean difference in STS score between cases and control groups: 0.37±1.01).
Periprocedural and 1-month follow-up
Expectedly, procedure time, use of contrast and radiation was higher in the combined group when compared with the controls with TAVI only. Despite these drawbacks, no difference in the VARC endpoints was evident during the in-hospital period and after 30 days (see tables 3 and 4).
Three-month follow-up
Table 5 illustrates the 3–4 months clinical and echocardiographic follow-up data. No patient was lost to follow-up. All patients but one (sudden cardiac death 118 days after the index procedure) were alive without events. Aortic bioprosthesis function was normal in all patients with no or mild paraprosthetic aortic regurgitation. No residual shunts or thrombi were seen after LAAO or PFO/ASD closure.
Discussion
Surgical aortic valve replacement is associated with an unadjusted operative mortality of 3% and reaches 5% when combined with CABG. The surgical mortality rate rises exponentially in patients above 80 years.19 Rates of thromboembolic complications (related to atrial fibrillation and paradoxical embolism) as well as spontaneous and iatrogenic bleeding tendency increase with advancing age as reflected in contemporary risk stratification systems. Octogenarians are reluctant to seek medical care and physicians are hesitant to apply appropriate therapeutic strategies. With the introduction of various catheter-based percutaneous structural heart disease interventions, this hitherto neglected morbid population gains access to guideline-based medical care.
In our series, all patients had severe aortic stenosis (which was treated by TAVI) and eight of them had significant coronary artery disease (of whom six were treated with DES along with TAVI). Regarding the time point of treating concomitant CAD, this should be treated at one time with the respective procedure of aortic valve replacement, irrespective of the approach selected by the heart team beforehand (ie, surgical revascularisation and SAVR or PCI and TAVI).
On top of that they had atrial fibrillation, which would have required chronic anticoagulation (CHADS2 score for all patients >1) in addition to dual antiplatelet therapy recommended for coronary stents for at least 3–6 months. Although newer data suggest safety and efficacy of a combination of clopidogrel and oral anticoagulation, many patients still receive triple oral antithrombotic therapy, which carries a significantly higher risk of bleeding than dual antiplatelet therapy20 ,21 while dual antiplatelet therapy alone is less effective than oral anticoagulation in preventing thromboembolic complications.22 LAA closure provides stroke prevention equal to that of warfarin without bleeding risk.11 Although the value of PFO/ASD closure as a primary prevention measure against paradoxical embolism is not clear, we performed this as the final step of the combined interventions among these patients because of the general ease of this intervention in the setting of LAA closure, with the appropriate gear already in place.
Compared with their matched counterparts receiving TAVI only, the combined intervention cases suffered from a higher burden of comorbidities and their procedures were longer and consumed more contrast dye. In spite of these disadvantages, the immediate and intermediate-term outcomes were not different between groups as judged by the VARC criteria. Alternatively to this single session approach a staged approach may reduce dye usage per session and hence transient kidney injury is occasionally encountered. However, this occurs at the expense of reduced patient comfort and compliance, which may lead to refraining from planned complementary interventions. Obviously, the power of the present study is too low to address the safety of increased contrast use. The combined procedures were all performed without general anaesthesia and without TEE guidance. Combining therapeutic measures becomes even more compelling if general anaesthesia and TEE guidance are deemed necessary.
Limitations
The present study has several limitations: first, the presented data reflect the experience of a high-volume tertiary care cardiology department. Second, due to the retrospective and observational character of the study, there was no prospective randomisation of cases, although the baseline STS score showed good agreement between the two groups after the performed matching process. Moreover, due to the manual matching a potential bias could have been introduced as compared with an automated process. Furthermore, the number of the reported combined cases and the respective event rates are low. Therefore, the issues of safety and net clinical benefit cannot be cleared definitively on the basis of the present study.
Conclusions
Transcatheter treatment of combined cardiac diseases is feasible even in a single session in high-volume centres with experienced operators. However, for definite proof of safety comparable to TAVI-only procedures, larger numbers of combined procedures or ideally, a controlled, prospective randomised study would be desirable.
References
Footnotes
AAK and SG contributed equally.
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
-
Competing interests BM has received lecture fees from AGA Medical; AK is a proctor of AGA's LAA occlusion programme, SW and PW have received unrestricted grants from Medtronic and Edwards Lifesciences. FN, LB and AK are proctors for Edwards and Medtronic.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.