Article Text

Abstract
Objectives This study evaluates predictors of conduction abnormalities (CA) following transcatheter aortic valve implantation (TAVI) in patients with bicuspid aortic valves (BAV).
Background TAVI is associated with CA that commonly necessitate a permanent pacemaker. Predictors of CA are well established among patients with tricuspid aortic valves but not in those with BAV.
Methods This is a single-centre, retrospective, observational study of patients with BAV treated with TAVI. Pre-TAVI ECG and CT scans and procedural characteristics were evaluated in 58 patients with BAV. CA were defined as a composite of high-degree atrioventricular block, new left bundle branch block with a QRS >150 ms or PR >240 ms and right bundle branch block with new PR prolongation or change in axis. Predictors of CA were identified using regression analysis and optimum cut-off values determined using area under the receiver operating characteristic curve analysis.
Results CA occurred in 35% of patients. Bioprosthesis implantation depth, the difference between membranous septum (MS) length and implantation depth (δMSID) and device landing zone (DLZ) calcification adjacent to the MS were identified as univariate predictors of CA. The optimum cut-off for δMSID was 1.25 mm. Using this cut-off, low δMSID and DLZ calcification adjacent to MS predicted CA, adjusted OR 8.79, 95% CI 1.88 to 41.00; p=0.01. Eccentricity of the aortic valve annulus, type of BAV and valve calcium quantity and distribution did not predict CA.
Conclusions In BAV patients undergoing TAVI, short δMSID and DLZ calcification adjacent to MS are associated with an increased risk of CA.
- Transcatheter Aortic Valve Replacement
- Aortic Valve Stenosis
- Congenital Abnormalities
- Pacemaker, Artificial
Data availability statement
No data are available. Data for this study are not available for sharing due to confidentiality reasons.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Transcatheter Aortic Valve Replacement
- Aortic Valve Stenosis
- Congenital Abnormalities
- Pacemaker, Artificial
WHAT IS ALREADY KNOWN ON THIS TOPIC
ECG, anatomical and procedural factors are associated with conduction abnormalities (CA) post-transcatheter aortic valve implantation in patients with tricuspid aortic valves.
WHAT THIS STUDY ADDS
Among patients with bicuspid aortic valves (BAV), short membranous septum (MS) length and implantation depth and device landing zone calcification adjacent to the MS are associated with an eightfold increased risk of CA. The quantity and distribution of valve calcification, eccentricity of the AV annulus or type of BAV were not associated with CA.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Larger studies examining the type of BAV and techniques to prevent CA are needed.
Introduction
With a prevalence of 0.9%–2% in the general population, bicuspid aortic valves (BAV) represent the most common congenital cardiac anomaly.1–4 BAV have a stronger tendency than tricuspid aortic valves (TAV) to cause aortic stenosis (AS), which tends to develop earlier in life.5–7 Unique anatomical differences compared with TAV pose a challenge to transcatheter aortic valve implantation (TAVI) including larger aortic root dimensions, more eccentric annulus, effaced sinuses, longer and more asymmetrical leaflets, concomitant presence of aortopathy, shorter membranous septum (MS), heavier calcific burden and the presence of calcified raphe.3 8–11 The evolution of TAVI has enabled progressively younger and lower-risk populations to be treated.12 13 Patients with BAV have been excluded from pivotal TAVI trials. However, several observational studies have evaluated the safety and efficacy of TAVI in patients with BAV demonstrating lower procedural success and higher complication rates, especially when using early-generation devices.14–17
Among these procedural complications is a significant incidence of conduction abnormalities (CA) leading to permanent pacemaker implantation (PPMI). A meta-analysis showed rates of new PPM, in BAV and TAV, respectively, of 17% and 26% using early-generation bioprosthesis, and 9.9% and 8.6% using new-generation bioprosthesis.18 Studies among patients with TAV have demonstrated ECG, anatomical and procedural factors that increase the risk of CA with TAVI.19 20 However, there is a lack of data regarding these characteristics in patients with BAV undergoing TAVI. This study examined the predictive role of pre-TAVI CT-based anatomical characteristics and peri-TAVI procedural characteristics associated with post-TAVI CA.
Methods
Study population
This retrospective, observational study included consecutive patients who underwent a TAVI for severe AS between January 2018 and December 2020 at a single centre, with a diagnosis of BAV (online supplemental figure 1). All patients underwent discussion at a multi-disciplinary team meeting to evaluate the indication, type and feasibility of valve replacement. TAVI was deemed to be the preferred treatment strategy in these patients. Patients with a BAV who were treated medically or surgically were not included in this study.
Supplemental material
Patient and public involvement
Patients and the public were not involved in the design and conduct of this study.
Clinical investigations
All CT scans were performed on a Somatom FORCE scanner (Siemens Healthineers, Erlangen, Germany). The TAVI evaluation CT protocol involves a topogram, calcium score, timing bolus, gated CT coronary angiogram acquired retrospectively, and a FLASH whole-body scan (lung apices down to the lesser trochanters). The total volume of Omnipaque 300 (iohexol) contrast (GE Healthcare, Chicago, Illinois) was fixed at 90 mL (including a 10 mL timing bolus).
All transthoracic echocardiograms were performed by British Society of Echocardiography (BSE) accredited physiologists pre-TAVI and post-TAVI. Valvular and myocardial structure and function were analysed based on BSE guidance.21
A 12-lead ECG was performed pre-TAVI and at several time points post-TAVI before the patient was discharged.
TAVI Procedure
All TAVIs were performed at single tertiary cardiac centre. Patients underwent pre-TAVI clinical investigations that included a CT scan, ECG and transthoracic echocardiogram. All patients were discussed at a multidisciplinary team meeting to evaluate their appropriateness for TAVI. Standard implantation techniques were used, with the choice of bioprosthesis left to the treating cardiologist. Patients have continuous ECG monitoring in the first 24 hours post-TAVI. This period is extended if significant CA are detected. Thereafter, patients have a daily ECG including on the day of discharge. ECGs were used to determine new CA that persisted until PPMI or discharge. Those that developed indications for PPMI had the device implanted during the same admission. The decision to do so was made by the structural intervention and electrophysiology teams, in conjunction with the patient.
Data collection
Demographic, clinical and procedural data were collected prospectively onto a local database. Multivessel coronary artery disease was defined as more than one major coronary artery with a stenosis >50% or left main stem stenosis >50%. Patients were considered frail if they had a Rockwood clinical frailty score >5. The pre-TAVI and post-TAVI (pre-discharge) 12 lead ECG were compared, and any new CA was identified. BAV morphology was defined by the Siever’s classification using CT.1 The pre-TAVI CT was used to measure the following variables:
Diameters of the aortic valve (AV) annulus, sinus of Valsalva, sinotubular junction and ascending aorta.
Area of the AV annulus.
MS length
Valve calcification (measured by Agatston score and calcium volume).
Calcium distribution (see online supplemental figure 1).
Presence of calcium in device landing zone (DLZ) of the left ventricular outflow tract (LVOT)
Aorto-annular angle.
CT image analysis
All analyses were performed using a Syngo Via platform (Siemens Healthineers, Erlangen, Germany) by two observers independently. An average of these two results was used for analysis. Where a discrepancy >10% between measurements was noted, the case was reanalysed by both observers and a third observer together until a measurement was agreed on. Using multiplanar reconstructions (MPR), cross-sectional images were used to calculate diameter and area measurements. The Agatston scores and valve calcium volume were calculated using a Hounsfield threshold of 130 HU and a non-contrast sequence. Due to the heterogeneity in BAV morphologies (number of leaflets, number of raphe, site of raphe) demarcation of calcification according to cusp becomes challenging. Instead, given that conduction tissue in the septum is an important anatomical landmark for CA, we opted for a standardised method to calculate calcium distribution according to its relationship with the MS. Calcium distribution was calculated as any calcification involving the valve itself, based on whether it was adjacent to or opposite the MS, rather than according to the cusp, thereby providing consistency in measurements. This was determined by dividing the AV in two based on the position of the MS—a virtual line that is 30°–45° to the anterior–posterior axis of the body and often follows the commissure between the left and right coronary cusp (RCC) and cuts through the non-coronary cusp (NCC) (online supplemental figure 1). In patients with type 0 BAV, this division was estimated based on the anatomical relationship between both atria and ventricles. Both Agatston score and calcium volume in mm3 were calculated. From the contrast enhanced MPR images, calcium in the DLZ of the LVOT was noted as being present or absent within the half adjacent to or opposite to the MS. Aortic annular eccentricity was calculated as the ratio between the smallest and largest diameter of the AV annulus. MS length was measured using the computerised measurement tool on Syngo Via on a contrast-enhanced coronal view using a previously described methodology.19 The MS was defined as the length of the thinnest portion of the septum, along the LVOT, from the AV annulus plane of the NCC to the boundary of the muscular interventricular septum. The aortoannular angle was measured as the angle between the longitudinal planes of the AV annulus and a point 4 cm distally in the aorta. The longitudinal plane was identified as a perpendicular line to the AV annulus and the cross section of the aorta 4 cm distal to the AV annulus. All the measurements above were determined using pre-TAVI CT scans.
Fluoroscopy image analysis
The depth of device implantation was measured using the procedural fluoroscopic image. This was determined at the time of the aortogram and comprised the distance from the AV annulus to the deepest part of the TAVI prosthesis within the left ventricle—a methodology proven to be reliably similar to CT determined implantation dept.22 The difference between MS length and implantation depth (δMSID) was calculated to demonstrate the placement of the device relative to the MS.
Study endpoint
The primary endpoint was new post-TAVI CA defined as either new high degree atrioventricular block (complete or second degree heart block), new onset left bundle branch block with a QRS duration >150 ms or PR interval >240 ms, pre-existing right bundle branch block (RBBB) with new PR prolongation or change in axis, as observed during the post-TAVI period prior to hospital discharge. This definition was based on current guidelines.23
Statistical analysis
Normality of continuous variables was evaluated using the Shapiro-Wilk test and presented using the mean±SD for parametric variables and median (IQR) for non-parametric variables. Frequencies are presented as number (percentage). Patients were divided according to whether they developed CA post-TAVI or not. Data were compared between these cohorts using a Student’s t-test for parametric data, Mann-Whitney U test for non-parametric data, χ2 or Fisher’s exact test for frequencies as appropriate and for the distribution of calcification, the Wilcoxon signed-rank test. Univariate logistic regression was used to assess the association between various CT-derived and procedural variables and CA. Those that were significant were included into a multivariate regression model along with first degree heart block (an established predictor of CA). Area under the receiver operating characteristic curve was used to test the diagnostic ability of significant continuous variables, with the Youden’s index used to identify optimal cut-off values. A new model was created using a composite of significant predictors to quantify their impact on CA. A two-sided p<0.05 was considered statistically significant. All analysis were performed using SPSS version V.28.0 (SPSS). Data are not available for this study due to confidentiality reasons.
Results
Baseline characteristics
A total of 1856 patients had a TAVI during the study period, of which 58 patients had BAV and were included in this study, age 76.0±9.8 years, 57% male and Logistic EuroSCORE 6.5 (4.2–11.4). 20 patients (34.5%) developed CA, of which 9 patients required a PPM. Patients were divided according to presence or absence of CA and baseline characteristics were compared between the two cohorts (table 1). Overall, demographics, comorbidities (with the exception of pulmonary disease), echocardiographic and ECG findings were similar between both cohorts at baseline. Calcium distribution adjacent to versus opposite the MS was compared for the entire study population—calcium score: 974 (590–1581) vs 2020 (1129–2719) respectively; p<0.001, respectively, and calcium volume: 789 (470–1249) vs 1595 (911–2167) mm3, respectively; p<0.001.
Baseline characteristics compared between patients with and without CA
TAVI procedure
The type of TAVI bioprosthesis used was similar between those with and without CA (p=0.266). All patients had transfemoral access. 3 patients in each cohort had self-expandable valves implanted with the majority of valves being balloon-expandible (online supplemental table 1).
Supplemental material
Implantation depth of the TAVI bioprosthesis in patients without compared with those with CA was 5.79±2.89 mm vs 7.49±3.05 mm; p=0.042, respectively. δMSID was 1.03±3.69 vs -1.32±3.85 mm; p=0.032, respectively. The average length of stay post-TAVI was 4.1±6.0 days.
Predictors of CA
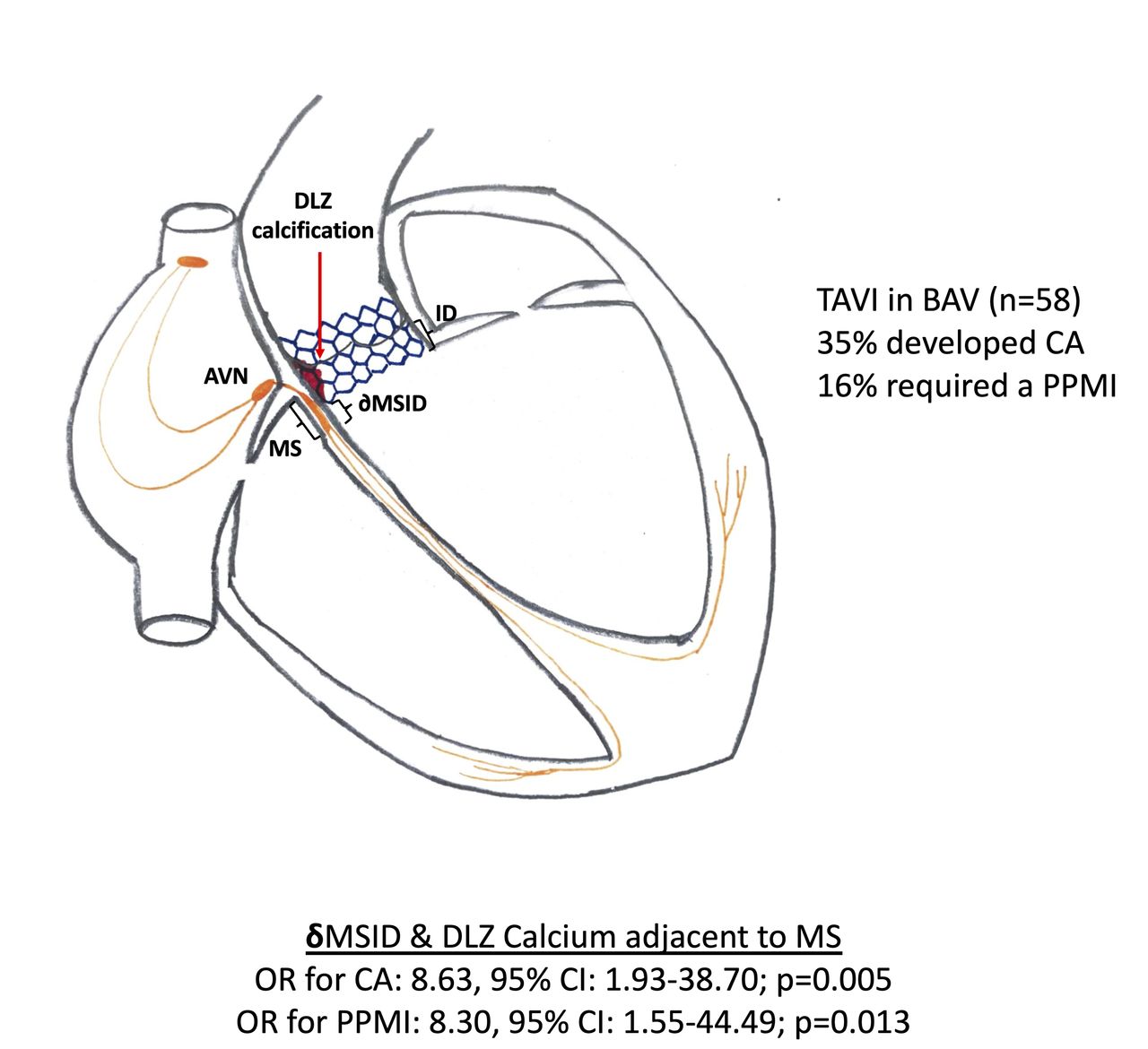
Univariate logistic regression for CA was performed on pre-TAVI CT based variables and peri-TAVI implantation depth (table 2). DLZ calcification adjacent to the MS, δMSID and TAVI implantation depth demonstrated significant association with CA (figure 1).
Univariate analysis for CA including CT based pre-TAVI variables and peri-TAVI implantation depth
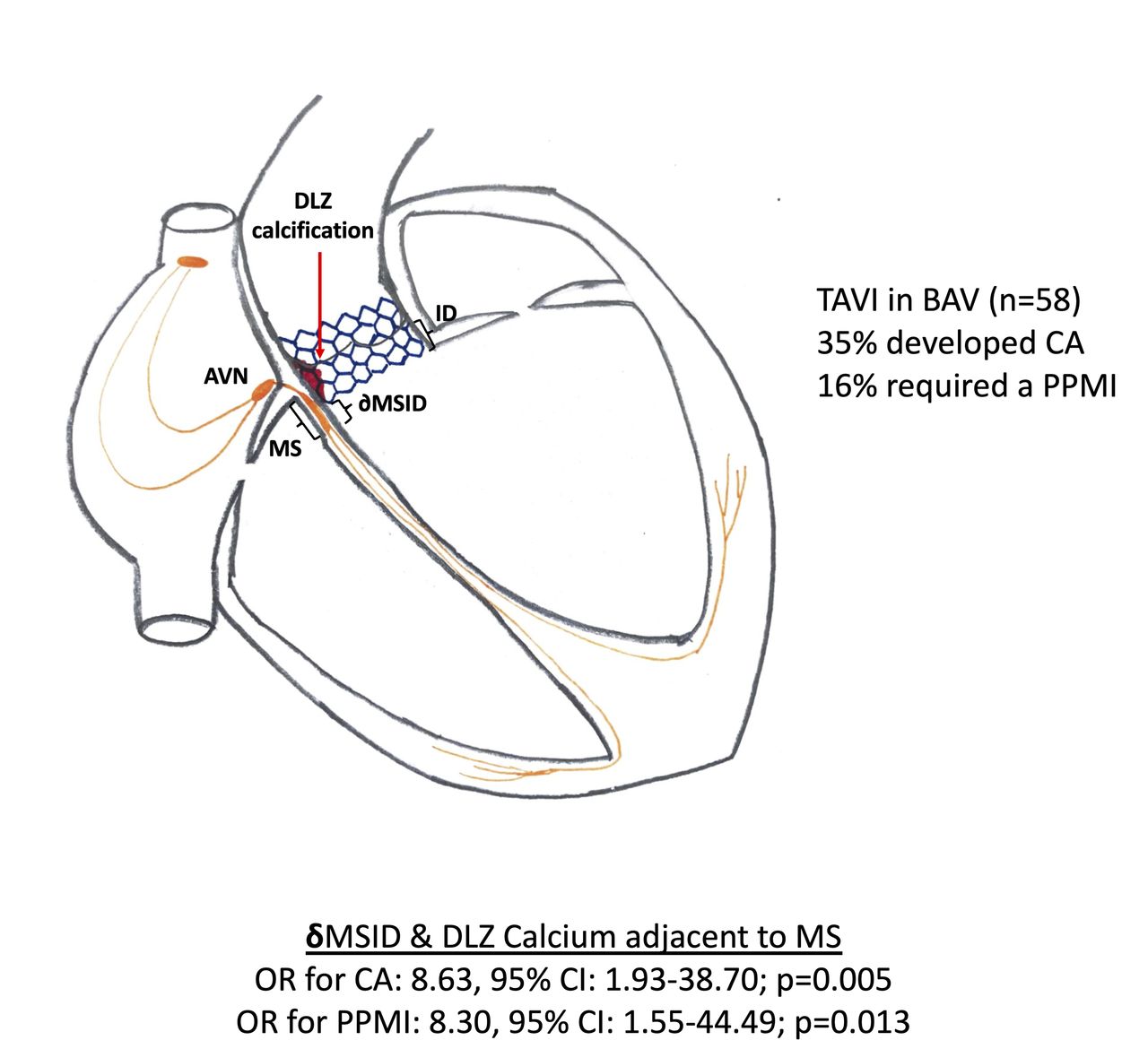
Predictors of CA in TAVI patients with bicuspid aortic valve stenosis. The figure illustrates the measurements of the MS, implantation depth and the difference between the two (δMSID). It also illustrates the anatomical relationship between the TAVI bioprosthesis and the conduction tissue. Device landing zone calcification adjacent to the MS can be seen in red. δMSID—difference between the MS depth and implantation dept; AUC, area under the curve; CA, conduction abnormalities; δMSID, MS length and implantation depth; MS, membranous septum; PPMI, permanent pacemaker implantation ROC,receiver operating characteristic; TAVI, transcatheter aortic valve implantation.
Using ROC curve analysis, the AUC for implantation depth and δMSID was 0.674 and 0.686, respectively (figure 2). The optimal cut-off for implantation depth and δMSID was identified as 7.05 mm and 1.25 mm, respectively.

{kind=link}
{kind=link}
ROC curve analysis for CA for δMSID and implantation depth. δMSID–difference between MS depth and implantation depth.
The diagnostic accuracy of these parameters was calculated using these cut-offs. Deep implantation demonstrated a high specificity (78%), but low sensitivity (60%), while low δMSID demonstrated high sensitivity (84%) and low specificity (51%) (table 3).
Diagnostic accuracy of parameters
Composite models for CA
Regression models were created incorporating the composite of DLZ calcification adjacent to the MS and the newly identified cut-offs for implantation depth (model 1) and δMSID (model 2) separately. Model 1 demonstrated an adjusted OR for CA: 11.9, 95% CI 2.0 to 70.9; p=0.006. Model 2 demonstrated an adjusted OR of 8.79, 95% CI 1.88 to 41.00; p=0.01 (table 4).
Multivariate regression models for conduction abnormalities
Compared with patients without both a low δMSID and DLZ calcification adjacent to the MS, those with only a low δMSID or only DLZ calcification adjacent to the MS did not demonstrate an increased risk of CA. Only the combination of both factors demonstrated increased risk; unadjusted OR 36, 95% CI 3.193 to 405.897; p=0.004 (online supplemental table 2).
Discussion
This study examined anatomical factors associated with post-TAVI CA in a BAV population. Our findings demonstrate that CA are associated with (1) deeper TAVI implantation, particularly in the presence of a short MS length and (2) presence of calcium in the DLZ adjacent to the MS. The composite of both factors is strongly predictive of CA. Lastly, the quantity and distribution of valve calcification, the eccentricity of the AV annulus or the type of BAV does not influence CA post-TAVI.
Although recent PPM rates have reduced with greater experience and improved technology,18 PPMI continues to place a significant burden on TAVI patients. Pacing in TAVI is associated with reduced improvement in left ventricular ejection fraction and increased rates of heart failure hospitalisation.24 Additionally, TAVI indications are expanding to include younger patients who will live longer—implying that more PPM device revisions will be required.25 Therefore, identifying patients at increased risk of CA and taking precautions to reduce this risk is important. This is particularly the case for patients with BAV, who tend to develop complications at a younger age than those with TAV. Previous studies evaluating CA post-TAVI have actively excluded patients with BAV.26–28
Our findings have important clinical implications for patients with BAV. Those with both DLZ calcification adjacent to the MS and a low δMSID have over an eightfold increased risk of developing CA. Our findings also suggest that having just one of these risk factors may not significantly increase the risk of CA (online supplemental table 2). Pathophysiologically, this implies that for the development of CA, the TAVI bioprosthesis needs to be at a certain anatomical position in order to exert a radial force on adjacent calcification that would impinge on the atrioventricular conduction tissue. We identified an implantation depth of 7.05 mm and a δMSID of 1.25 mm as the optimum cut-off values for prediction of post-TAVI CA. Similarly, another study in TAV patients, proposed similar cut-off values for implantation depth, ranging from 6.3 to 7.0 mm, depending on the type of TAVI bioprosthesis used.29
Some studies conducted in TAV patients have found a shorter MS depth to be an independent predictor of post-TAVI CA and, thus, PPMI,19 26 but our study and that of Tretter et al did not.27 There are several possible reasons that can explain this discrepancy. The location of the atrioventricular node is variable within the triangle of Koch and subsequently affects the location of the Bundle of His.30 Additionally, the depth of the conduction tissue within the muscular ventricular septum and the force exerted by the TAVI bioprosthesis on this tissue is likely to vary.27 These variations suggest that the susceptibility of the conduction tissues to impingement by a TAVI bioprosthesis may vary between populations. Within the BAV population, implantation depth and the subsequent δMSID appear to be more important than MS depth.
A study among TAV patients demonstrated greater LCC calcification as a predictor of post-TAVI CA requiring PPMI.31 This finding can be explained by the anatomical location of the atrioventricular conduction tissue within the interleaflet fibrous triangle that separates the NCC from the RCC and opposite the LCC.32 More calcification of the LCC may potentially push the TAVI bioprosthesis towards the atrioventricular conduction axis, disturbing the bundle of His. BAV valves are known to be heavier, suggesting more calcification and fibrosis, compared with TAV,33 with calcification described as asymmetrical and most commonly affecting the fused raphe and LCC.34 In line with this, our findings demonstrated greater calcification opposite the MS. However, contrary to previous findings in TAV,31 this asymmetrical distribution of calcification was not associated with CA in patients with BAV.
Conversely, we found DLZ calcium adjacent to the MS had a significant impact on CA, a finding similar to a previous study among TAV patients.26 The most plausible explanation for this, is that the radial force exerted by the bioprosthesis impinges the calcium onto the atrioventricular conduction tissue. Our study did not find any difference in CA between the different BAV morphologies, or due to aortic annular eccentricity.
Study limitations
This study is limited by its population size—58 patients, of which 20 suffered from post-TAVI CA. Consequently, this restricted our multivariate models to two covariates. The study population was derived from a TAVI cohort which is older and at higher surgical risk, limiting its generalisability to other patients with BAV. We predominantly used balloon expandible valves. Oversizing of valves was not measured in this study and has been shown to be an important determinant of post-TAVI CA.22 Additionally, we had a predominance of type 0 and type 1 (L-R) within our population. Larger studies need to evaluate whether certain morphologies increase the risk for CA. Pre-TAVI RBBB and self-expanding valves were not well represented in this population—two and six patients, respectively. Therefore, the lack of association between these variables and CA should not be interpreted as unimportant factors in the BAV population. Defining the AV annulus in order to measure implantation depth and MS depth can be challenging, especially in patients with type 0 BAV as only 2 cusp edges are available. However, by using three independent observers to analyse the data, we minimised the risk of inaccuracies. We did not consider post-discharge CA or PPMI as part of the endpoints, which can occur among TAVI patients. However, majority of CA do take place during the immediate post-TAVI period, implying that most events would have been captured in this study.
Conclusions
In patients with BAV undergoing TAVI, low δMSID and DLZ calcification adjacent to the MS are associated with an increased risk of CA. The quantity and distribution of valve calcification, eccentricity of the AV annulus or type of BAV were not associated with CA.
Data availability statement
No data are available. Data for this study are not available for sharing due to confidentiality reasons.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by North West-Greater Manchester South Research Ethics CommitteeReference number: 21/NW/0182The North West-Greater Manchester South Research Ethics Committe waived the need for informed consent given the retrospective, observational nature of the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @bartstrctural
GE and NK contributed equally.
Contributors GE and NK were first joint authors of this study. GE, NK, KPP, MM, AC and AM were involved in the genesis and design of this study. All authors contributed to the data collection, GE, NK, MS, FP and KPP were involved in the CT analysis. GE, NK and KPP were involved in the statistical analysis. GE, NK, MM and KPP were involved in writing the initial draft of this manuscript. All authors read, edited and approved the manuscript. KPP is the guarantor.
Funding FP has received research support from Siemens Healthineers. AWCC has received Research grant from Boston Scientific and Abbott. AM is employed by Abbott Medical UK. MM has received grants and personal fees from Edwards Lifesciences and personal fees from Abbott Vascular. KPP is funded by a British Heart Foundation clinical research training fellowship grant (FS/19/48/34523) and has an unrestricted research grant from Edwards Lifesciences.
Competing interests All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work. FP has received research support from Siemens Healthineers. AWCC has received Research grant from Boston Scientific and Abbott. AM is employed by Abbott Medical UK. MM has received grants and personal fees from Edwards Lifesciences and personal fees from Abbott Vascular. KPP is funded by a British Heart Foundation clinical research training fellowship grant (FS/19/48/34523) and has an unrestricted research grant from Edwards Lifesciences.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.