Article Text

Abstract
Background Cardiopulmonary exercise testing (CPET) has shown to be useful for preoperative risk stratification in various types of intra-abdominal and thoracic surgery. However, data about the predictive value of CPET for cardiovascular outcome after gastric or oesophageal cancer surgery are inconclusive. The aim of this study was to evaluate the prognostic value of CPET parameters for the prediction of cardiovascular complications in patients with this type of surgery.
Methods This is a prospective single-centre interventional cohort study including 200 consecutive patients who underwent elective surgery for oesophageal and/or gastric cancer. Symptom-limited CPET was performed preoperatively to evaluate the potential of various test-derived parameters including anaerobic threshold (AT) to predict cardiovascular complications within 30 days after surgery.
Results 200 patients (mean age 68±14.2 years) met inclusion and exclusion criteria: oesophageal surgery 54 pts, gastric surgery 132 pts and combined oesophageal/gastric surgery 14 pts. 41/200 pts (20.5%) experienced cardiovascular complications during and within 30 days after surgery including 4 non-fatal myocardial infarctions (2%), 1 stroke (0.5%); 6 dead from cardiovascular causes (3%) and less serious complications in 30 patients (15%) including angina attacks and antiarrhythmic therapy for ventricular arrhythmias or for atrial fibrillation/flutter. Results from preoperative CPET indicate that an AT level below 11 mL/kg/min was highly predictive for any cardiovascular complication (p=0.02, OR 6.33, 95% CI 1.78 to 22.47). An AT level <9.5 had the best predictive accuracy for major perioperative cardiac complications (sensitivity 93%, specificity 68%, positive predicative value 75%, negative predicative value 98.8%).
Conclusion CPET is a useful perioperative risk assessment tool for patients undergoing surgery for oesophageal and gastric cancer, which carries a particularly high risk for cardiovascular complications. An AT <9.5 mL/kg/min turned out to be the most reliable predictor for major cardiovascular complications.
- Delivery of Health Care
- Outcome Assessment
- Health Care
- General Surgery
- Acute Coronary Syndrome
- Myocardial Infarction
Data availability statement
Data are available on reasonable request. Availability of the full research protocol and data by request from the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Delivery of Health Care
- Outcome Assessment
- Health Care
- General Surgery
- Acute Coronary Syndrome
- Myocardial Infarction
What is already known on this topic
Cardiopulmonary exercise testing (CPET) has shown to be useful for preoperative risk stratification in various types of intra-abdominal and thoracic surgery. However, data about the predictive value of CPET for cardiovascular outcome after gastric or oesophageal cancer surgery are inconclusive.
What this study adds
CPET is a useful tool for perioperative risk assessment for patients undergoing surgery for oesophageal and gastric cancer. An anaerobic threshold <9.5 mL/kg/min turned out to be the most reliable predictor for major cardiovascular complications.
How this study might affect research, practice or policy
CPET might be used as perioperative risk assessment tool for selected patients undergoing surgery for oesophageal and gastric cancer in the future.
Introduction
Previous studies indicate that cardiopulmonary exercise testing (CPET) is a useful tool for preoperative risk assessment for patients undergoing major non-cardiopulmonary surgery. Preoperative risk assessment is of particular importance in view of the increasing number of elderly and frail patients with comorbidities. Cardiovascular complications have been reported in up to 3.5% and fatal complications in up 1.8% of patients undergoing various types of non-cardiac surgery. Cardiorespiratory complications in non-cardiac surgery have been investigated in recent studies.1 2 The incidence of perioperative myocardial infarction with various abdominal interventions is up to 5%.3–5 The risk of surgery for cancer of stomach, oesophagus or oesophagus with transition to the cardiac part of the stomach is particularly high—up to 8% for perioperative MI or death, and therefore, the availability of a reliable tool to predict perioperative risk is of particular importance.3 6
CPET provides a whole range of physiological parameters and much of this is underused clinically. CPET allows to assess causes of reduced oxygen consumption, differentiating and determining the degree of respiratory and heart failure, and evaluation of exercise tolerance and metabolism dysfunction in muscle tissue. Among CPET parameters which are used in clinical practice, the anaerobic threshold (AT) turned out to be of particular importance: The AT is reached at the moment when the capacity of aerobic metabolism in muscle tissue becomes insufficient and the anaerobic pathway of oxidative phosphorylation is activated. The level of AT depends on the initial metabolic situation including the glycogen concentration in muscle cells, the number and density of mitochondria, and—to a lesser extent—the arterial blood flow. The prognostic value of the AT index is well known in patients with chronic heart failure and coronary heart disease.7–9 CPET allows to determine maximum oxygen consumption which reflects the function of the respiratory and cardiac system, the state of peripheral blood flow and of tissue metabolism. In addition, the method allows to determine the AT—the parameter of the readiness of metabolism for a sharp load or lack of oxygen. During major surgery, episodes of hypoxia or anaemia with increased oxygen demand combined with stress from tissue traumatisation may occur, which may lead to cardiac complications.10 CPET can be useful to predict the development of complications associated with these problems. In a study including 843 patients who underwent mixed intra-abdominal surgical procedures, an AT <11 mL/kg/min was associated with increased hospital mortality with a sensitivity of 88% and a specificity of 47%. At the same time, VE/VCO2>34 was an independent predictor of hospital mortality with a sensitivity 88% and a specificity 47%.11 Furthermore, it has been shown that patients with postoperative cardiopulmonary complications had a significantly lower _VO 2 peak.(19.265.1 mL/kg/min) than those without complications (21.46 4.8 mL/kg/min) (p=0.04)
At the same time, a leading cause for cardiovascular complications in the perioperative period including the development of myocardial infarction is metabolic failure.3 12 Therefore, the aim of our study was to identify the prognostic value of the AT level calculated during CPET in high-risk gastric and oesophageal cancer surgery.
Material and methods
This is a single-centre prospective cohort study with sequential inclusion of patients. The study was conducted at the University Clinical Hospital No. 1 of the First Sechenov Moscow State Medical University.
Study patients
The aim of the study was to include 200 consecutive patients who underwent elective surgery for oesophageal and/or gastric cancer.
Inclusion criteria were being over 18 years of age and being planned for elective surgery for oesophageal and/or gastric cancer. Exclusion criteria were contraindications to perform an elective surgical intervention6; contraindications to CPET8 and refusal of the patient to participate in the study.
The preoperative cardiovascular examination included (1) consultation with a cardiologist, (2) 12-lead resting electrocardiography (ECG); (3) transthoracic echocardiography and (4) cardiopulmonary symptom-limited exercise test (CPET).
Based on the results of the preoperative cardiovascular examination, contraindications and the need for therapeutic interventions prior to the surgery were defined. In case of a significant change of medical treatment in this preoperative period, a re-examination, including repeated CPET, was performed. The analysis included data from the last tests, done just before surgery.
Cardiopulmonary exercise testing
We used the SCHILLER CS-200 CPET system and a treadmill for exercise testing. A modified BRUCE protocol was chosen for all patients. Symptom-limited tests have been performed according to actual guidelines.5 The following parameters were measured: ventilation (VE); oxygen consumption (VO2); carbon dioxide production (VCO2); Oxygen pulse (O2-pulse). The AT level was determined by the V-slope velocity ratio method by the occurrence of a sharp increase in the ratio of carbon dioxide release to oxygen consumption.8
Definition of cardiovascular outcome
The primary endpoint was defined as
Death from cardiovascular causes (defined based on pathoanatomical findings).
Myocardial infarction (defined as increased troponin T or troponin I levels in combination with typical ECG dynamics, or based on autopsy data) either/or
stroke (diagnosis confirmed by brain tomography or at autopsy).
The secondary endpoints included:
Angina pectoris attacks (typical chest pain with ECG changes).
Ventricular arrhythmias requiring antiarrhythmic therapy.
Persistent or paroxysmal supraventricular tachycardia.
Persistent or paroxysmal atrial fibrillation/flutter.
The combined endpoint included all complications which are listed above.
Cardiac complications has been registered at the following time points: during surgery, within 30 days after surgery or until the end of the hospitalisation period if longer than 30 days.
Statistical analysis
Processing of information for statistical analysis was carried out using Microsoft Excel and a package of statistical programmes including Statistica and SPSS version 17.0. Data are presented as median, IQR (the values 25 and 75 percentiles). Characteristics of the groups were compared using the χ2 OR was calculated as (Eventstreatment / Non-eventstreatment) / (Eventscontrol / Non-eventscontrol). Fisher test was used for ordinal variables, and the Mann-Whitney U-test for continuous variables. An additional analysis was carried out using receiver operating characteristic () curves with the SPSS program. Threshold values of indicators were determined by ROC curves according to the optimal ratio of sensitivity and specificity.
Results
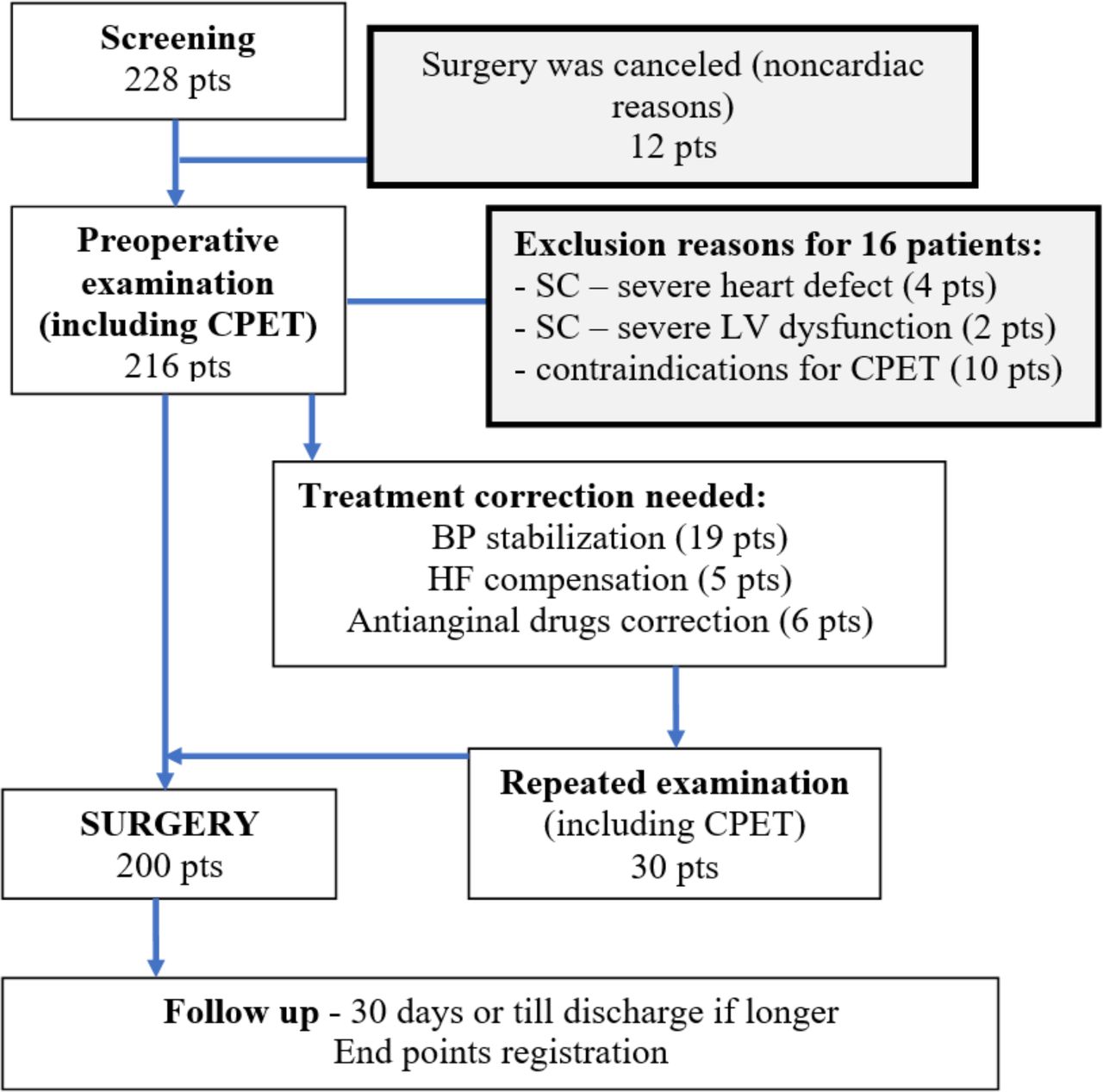
A total of 228 consecutive patients have been screened and 200 patients have been included in the study population. The study flow chart in shown in figure 1.
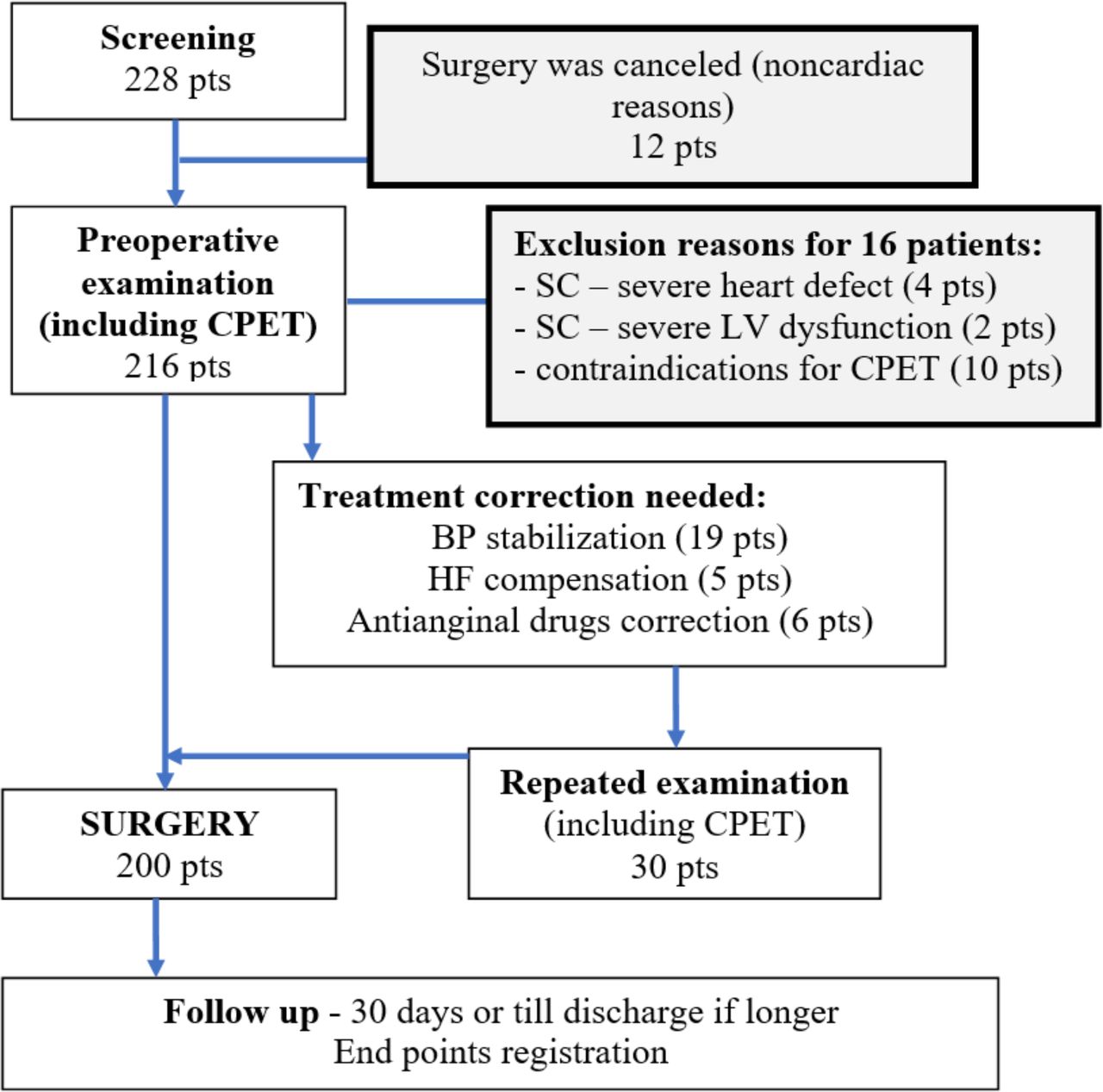
Study flow chart. BP, blood pressure; CPET, cardiopulmonary exercise test; HF, heart failure; SC, surgery contraindications, V, left ventricle.
Basic characteristics of the study patients are presented in table 1. Mean age of the patients was 68±14.2 years.
Basic characteristics of patients included in the study (n=200)
Surgical intervention
Surgery for oesophageal cancer was performed in 54 patients, surgery for gastric cancer in 132 patients and 14 patients underwent combined surgery for oesophageal and gastric cancer. In 28 cases, the surgical intervention was performed both from thoracic and abdominal access. Transhiatal extirpation of the oesophagus with gastric tube plastic surgery and neck anastomosis was performed in early oesophageal cancers stages (1 and 2). In cases of cancers of the body and the cardiac part of the stomach, gastrectomy was performed with extended D2 lymph node dissection and resection of the abdominal oesophagus with Roux-en-Y reconstruction. All operations were performed under a combination of general and regional (epidural) anaesthesia. General anaesthesia was induced and maintained using either intravenous or inhaled agents. The trachea was intubated and all patients were mechanically ventilated. Epidural anaesthesia was used in 112 patients to block pain sensitivity in a particular area and to reduce the need for narcotic analgesics.
Study endpoints
The distribution of study end points depending on the type of operation is presented in table 2.
Endpoints reached in different types of surgery
On the day of surgery, the following complications were registered: one nonfatal myocardial infarction, two episodes of atrial fibrillation and two episodes of sustained ventricular tachycardia which required antiarrhythmic treatment. The majority of endpoints (75.6%) were registered within 2–5 days after surgery whereas 12.2% of all endpoints ocurred 6–30 days after surgery.
All-cause mortality was 5.5% (11 patients): 3 patients died from sepsis 1–2 weeks after surgery, 2 patients died 1 day after surgery due to internal bleeding. Death from cardiovascular causes occurred in 3.0% (six patients). Combined endpoints were found in 41 patients (20.5%).
We analysed the difference in main characteristics between patient with and without EP. Patients >75 years of age experienced a primary EP significantly more often compared with patients<75 years (36.0% vs 18.7 %, p=0.023, OR 2.45, 95% CI 1.21 to 4.98). The highest risk to reach the primary EP was found in patients with previous MI, compared with patients with no previous MI (42.0% vs 20.7%, p=0.034, OR 3.0, 95% CI 1.52 to 5.98).
Echocardiography parameters did not predict the risk for primary and secondary endpoints. It has to be mentioned, that left ventricular ejection fraction did not differ between patients with EP and without them (54.5% vs 54.8%, p=0.43).
Among the various CPET indicators obtained, only a few were significantly associated with EP development (tables 3 and 4).
CPET parameters associated with the primary endpoint
CPET parameters associated with the secondary endpoints
Parameters of CPET associated with combined endpoint were just similar for those for secondary end points: AT (p=0.02), maximal load (p=0.02).
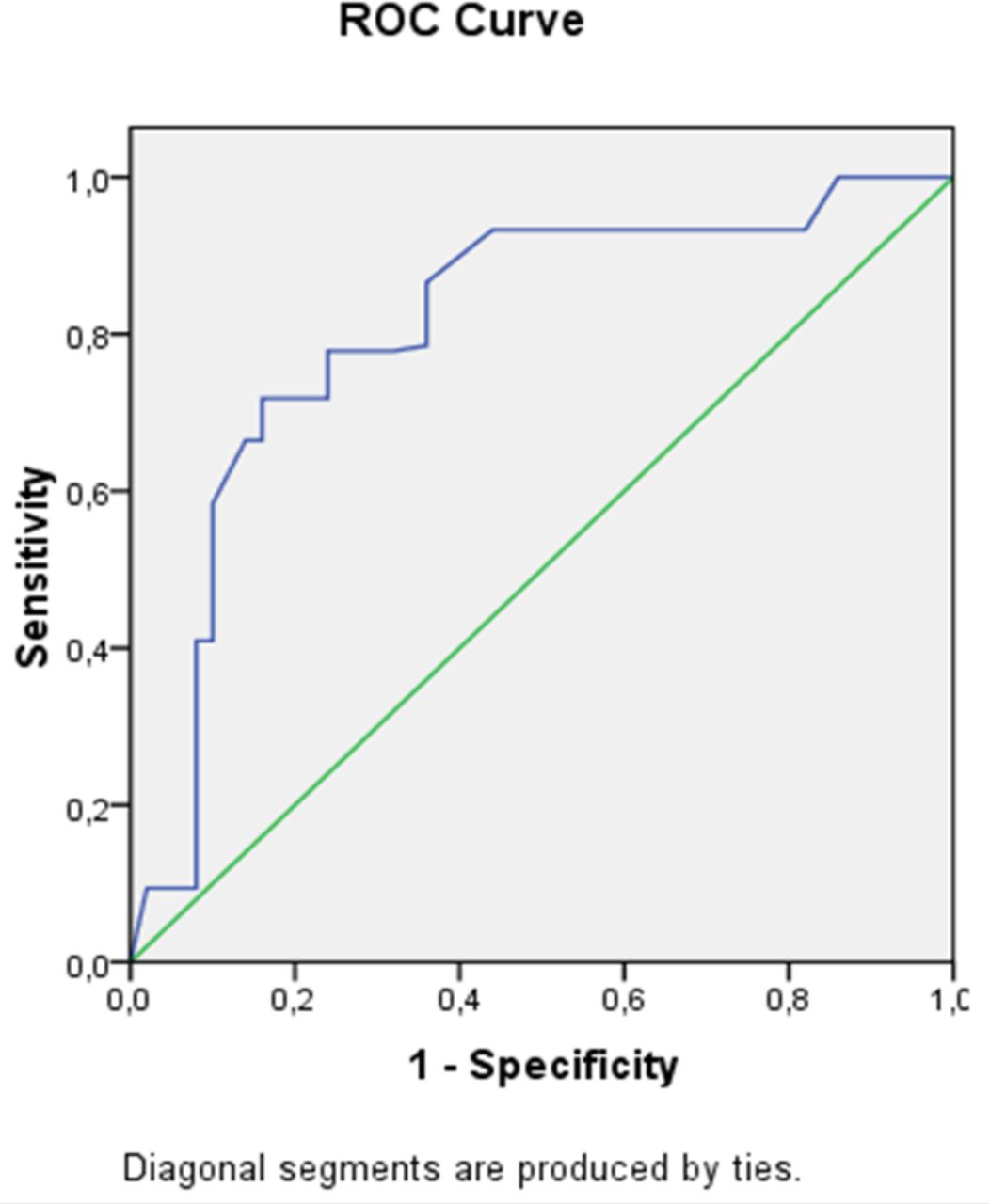
ROC analysis of AT was performed to determine the sensitivity and specificity in PEP prognosis in the perioperative period (figure 2).

{kind=link}
{kind=link}
Anaerobic threshold at for prognosis of primary cardiovascular endpoints (death from cardiovascular cause, perioperative myocardial infarction or stroke) in patients before surgery for oesophageal or gastric cancer. ROC, receiver operating characteristics.
AT level <9.5 mL/kg/min had the best sensitivity (93%) with moderate specificity (68%). Positive predicative value was—75.0%, negative predicative was value—98.9%.
An AT level <11 had the highest diagnostic accuracy for the occurrence of a primary EP : sensitivity was 88% and specificity 79%. The positive predicative value was 66.7%, the negative predicative value—97.4%.
AT did not prove to be an independent predictor for the occurrence of a secondary EP or for combined EP.
Discussion
Our results indicate that the AT derived from CPET is a useful perioperative risk assessment tool for patients undergoing surgery for oesophageal and gastric cancer. An AT <11 mL/kg/min turned out to be the most reliable predictor for minor and AT <9 mL/kg/min. for major cardiovascular complications.
Our findings confirm current knowledge indicating that oesophageal and gastric surgery is associated with a high risk of cardiovascular complications and is therefore classified as a high cardiovascular risk group in current guidelines (risk of death, heart attack and stroke >5%).13–15 However, available scales for preoperative risk evaluation are based on limited functional parameters or by complex echocardiographic examinations, and not on the evaluation of functional capacity by CPET.3–5 Besides, it is known that surgical risk doesn’t only depend on the type of surgery, but also differs between surgical centres and operation techniques. Furthermore, particularities of tumour localisation and type, spreading to adjacent tissues and other individual features are known to have a great impact on the result of surgery and complications. Therefore, we decided to perform our study as a prospective single centre study with a homogenous team of surgeons, anaesthesiologists, medical staff and the same treatment plans to acquire risk factors and risk rates under controlled conditions.
CPET allows to assess the functional reserve of the body and the presence and degree of cardiac, respiratory and metabolic insufficiency.8 14 Decreased metabolic activity in cells, decreased efficiency of oxygen consumption, and decreased functionality of muscle tissue with hypoxia are the major underlying causes for an increased risk of perioperative cardiovascular complications. Therefore, it is most important to determine the functional state of the patient before surgery. Several systematic reviews have been performed over the past few years to evaluate the role of CPET as a risk-assessment method in patients undergoing intra-abdominal or other non-cardiopulmonary surgery.2 16–21 Results confirm that functional capacity evaluated as AT and peak oxygen uptake (VO2peak) have a high predictive value for postoperative morbidity and mortality in the majority of surgical cohort studies. However, it is not unexpected that results differ according to the type of surgery and to cohort characteristics. At the same time, only few studies are dedicated to the evaluation of the cardiovascular risk related to upper gastrointestinal surgery. Nagamatsu et al found that VO2max was lower in patients with cardiopulmonary complications.22 In contrast, Moyes et al reported that VO2peak was not associated with cardiopulmonary complications but AT was associated with morbidity.20 It should be noted that most of the studies aimed to determine the risk factors for cardiopulmonary complications. As pulmonary complications are not uncommon in the postoperative period, our study differs by having a major focus on cardiovascular complications.
A main reason to determine the prognostic value of CPET parameters for high-risk surgical interventions in patients with cancer of the abdominal cavity is that they are generally weakened, starving and/or with anaemia before surgery.20 Such patients do not tolerate maximal exercise load. Parameters of maximum exercise tolerance and oxygen consumption are reduced not primarily because of cardiac pathology, but because of general weakness in these cancer patients. Under these circumstances, indicators of the AT depend not primarily on the maximum load tolerance, but on the functional reserve of muscle cells, the energy activity of mitochondria, and the concentration of glycogen in the liver and in the muscles. Therefore, it could be expected that the AT turns out to be an independent prognostic predictor for severe perioperative complications in our study. According to our data, a decrease in the AT below 11 mL/kg/min predicts the development of major cardiac complications with an OR=6.3 (p=0.001). Thus, the obtained data allows us to identify patients with an increased risk of surgery. Our findings can be used for clinical decision-making and for planning of perioperative care. It is of special note that most of the complications did not develop during the operation, but rather on the first postoperative day and then for another 3–5 days. This finding has important implications for the postoperative monitoring patients with higher cardiovascular risk which may be planned for up to 5 days from the date of surgery to allow timely intervention in case of deterioration during this critical period.
The major strength of the study is the relatively large number of consecutive cancer patients with the same type of surgery in the setting of a single surgery department with a stable team of surgeons and well defined operational and treatment procedures. Another strength is the relatively large number of CPET which have been performed using the same procedures and the same protocol by a single team. Furthermore, there was no lost to follow-up.
A limitation of the study is the fact that the numbers of events are rather low to make more deep statistical analysis for some subgroups of patients. This does not allow to make meaningful adjustments of the results for factors such as age (although patients aged >75 years met primary EP more frequently (OR=2.45)), gender, tumour stage or comorbidities.
Conclusion
CPET is a useful perioperative risk assessment tool for patients undergoing surgery for oesophageal and gastric cancer, which carries a particularly high risk for cardiovascular complications. An AT <11 mL/kg/min turned out to be the most reliable predictor for minor and AT <9 mL/kg/min. for major cardiovascular complications.
Data availability statement
Data are available on reasonable request. Availability of the full research protocol and data by request from the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Ethics Committe of the Sechenov University, Moscow RUID 11.12.2013, protocol 12-13. Participants gave informed consent to participate in the study before taking part.
References
Footnotes
Twitter @hugo saner
Contributors PC acts as a guarantor; PC, MP, PK and DA were involved in the planning of the study; PC, DV did the data acquisition; PC, MP, PK and HS were involved in data analysis and interpretation of data; all authors were involved in the manuscript writing, all authors reviewed and approved the manuscript.
Funding This work was financed by the Ministry of Science and Higher Education of the Russian Federation within the framework of state support for the creation and development of World-Class Research Centers 'Digital biodesign and personalized healthcare' #075-15-2020-926.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.