Article Text

Abstract
Background Proprotein convertase subtilisin/kexin type 9 inhibitors (PCSK9is) are an important but underutilised option to help optimise lipid management. We developed a new service to improve patient access to these medicines in line with National Institute for Health and Care Excellence recommendations. This paper describes the model and provides lipid-lowering results and feedback from the first 100 referred patients.
Methods The service is based on a centralised multidisciplinary clinic that is the sole prescriber of PCSK9i therapy in the area. Referred patients are assessed for eligibility and given tailored, person-centred support, education and monitoring to promote treatment adherence and lipids optimisation. The clinic also supports referred patients that do not meet PCSK9i eligibility criteria.
Results Among the first 100 patients referred (n=62 male; mean age: 62.9±10.5 years), 48 were initiated on PCSK9i therapy. Mean total cholesterol decreased from 7.7±1.6 mmol/L at baseline to 4.5±1.4 mmol/L at 3 months (41% reduction), while mean low-density lipoprotein-cholesterol (LDL-C) fell from 5.0±1.6 mmol/L to 2.1±1.3 mmol/L (58% reduction; p<0.0001) and median LDL-C decreased from 4.8 mmol/L to 1.6 mmol/L (67% reduction) over the same period. These decreases were maintained at 12 months (45%, 65% and 67% reductions, respectively; p<0.0001 for the decrease in mean LDL-C from baseline). Patient feedback on the clinic was positive and overall satisfaction was high.
Conclusions This innovative, person-centred, multidisciplinary service successfully initiated PCSK9i therapy for eligible patients and drove long-term monitoring, adherence and cholesterol lowering. It also provided medicines optimisation and adherence assistance to PCSK9i-ineligible patients. The model could be used in other areas to support better uptake and optimisation of PCSK9i therapy.
- Hyperlipidemias
- Atherosclerosis
- Delivery of Health Care
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Lipid optimisation is important to reduce the risk of cardiovascular disease.
Although statins are central to lipid management, there are significant challenges; some patients report intolerance or reluctance, others poorly adhere to these medicines,and some do not achieve acceptable levels of lipid reduction on maximum tolerated therapy.
Proprotein convertase subtilisin/kexin type 9 inhibitors (PCSK9is) offer another option to better manage hyperlipidaemia but are underused despite being recommended by the UK National Institute for Health and Care Excellence (NICE).
What does this study add?
This paper describes an innovative, person-centred, centralised, multidisciplinary service that has been successfully deployed to improve PCSK9i utilisation in line with NICE recommendations, leading to improved lipid management.
The service does not focus only on PCSK9is but also attempts to address other challenges in the optimisation of lipid management, such as statin intolerance and adherence. The model was found to be cost effective and was funded by the Clinical Commissioning Group.
It also paved the way for multidisciplinary working and the implementation of more streamlined mechanisms for referring appropriate patients.
How might this impact on clinical practice?
This service improved access to PCSK9i among eligible patients—and can be duplicated in other centres to offer patients better optimisation of their lipid management.
The model is flexible enough to allow the introduction of other novel medications for cholesterol lowering—and is multidisciplinary, thereby allowing all relevant healthcare professionals to contribute to lipid management.
It can also bridge the gap for patients with statin intolerance.
Introduction
Lipid lowering is central to the management of dyslipidaemia in patients with elevated cardiovascular risk.1 2 Statins are a mainstay of the current approach,1–3 but discontinuation and non-adherence remain common challenges.4 5 Indeed, up to three-quarters of patients are believed to discontinue statins within the first 2 years.6 Furthermore, reported intolerance is high. As many as one in five patients may be unable to continue on a daily statin because of presumed intolerance issues, particularly muscle cramps,3 7 although a short ‘drug holiday’ can improve tolerance.8 In addition, some patients inevitably fail to reach low-density lipoprotein-cholesterol (LDL-C) targets despite tolerating and adhering to an optimised statin dose, even with the addition of ezetimibe.
Until recently, there were limited options for managing dyslipidaemia in patients at high risk with statin intolerance or who otherwise failed to meet their target. However, proprotein convertase subtilisin/kexin type 9 inhibitors (PCSK9is) provide an alternative. They work by acting on PCSK9, a key protein involved in the regulation of serum LDL-C through interaction with the LDL receptor.9 Two PCSK9i treatments, alirocumab and evolocumab, have been approved by the European Medicines Agency based on phase 3 trials demonstrating significant reductions in LDL-C and cardiovascular disease (CVD) events.10 The recent licensing of bempedoic acid and inclisiran in the UK (as well as Europe and the USA) provides additional options.11 12 However, these were not available when the present project was set up.
Current European dyslipidaemia management guidelines recommend that PCSK9is should be considered for patients at very high risk who do not achieve their LDL-C goal on a maximum tolerated dose of a statin and ezetimibe.2 The UK National Institute for Health and Care Excellence (NICE) has a different approach, as published in its technology appraisal guidance on alirocumab and evolocumab in June 2016.13 14 NICE recommends these drugs as an option for treating primary hypercholesterolaemia or mixed dyslipidaemia if LDL-C concentrations are persistently above specific thresholds (table 1), despite maximal tolerated lipid-lowering therapy, that is, if the maximum dose has been reached or further titration is limited by intolerance (defined as clinically significant adverse effects that represent an unacceptable risk or may reduce treatment adherence).15
NICE criteria thresholds for recommending PCSK9i therapy in patients with persistent hypercholesterolaemia13 14
NICE and ESC also have different cholesterol-lowering targets. ESC guidelines recommend an LDL-C reduction of ≥50% from baseline and LDL-C <1.4 mmol/L in the context of primary and secondary prevention for patients who are at very high risk of CVD. For secondary prevention among patients at high risk, an LDL-C reduction of ≥50% from baseline and LDL <1.8 mmol/L are recommended.2 NICE generally recommends a >40% reduction in non-high-density lipoproten-cholesterol (HDL-C), and for patients with familial hypercholesterolaemia (FH), NICE recommends a ≥50% reduction in LDL-C.1 15
The National Health Service (NHS) in England is legally obliged to make available to eligible patients any medicine recommended by NICE within 3 months of that guidance being issued.16 However, given the high cost of PCSK9is, the importance of ensuring appropriate prescribing and the need for substantial patient education and monitoring, it was clear to us that a bespoke management model was required. The Leeds Teaching Hospitals NHS Trust (LTHT), therefore, undertook to design an appropriate PCSK9i service for its local area. A centralised model was developed based on a person-centred approach.
The aims of the service were: to assess patient eligibility for PCSK9is in line with NICE guidance; in ineligible patients, to provide specialist input to optimise lipid-lowering treatment and ensure appropriate onward referral; and, in eligible individuals, to provide tailored support, education and monitoring to promote treatment adherence and optimisation of LDL-C.
Here, we describe the model, and provide lipid-lowering results and patient questionnaire feedback from the first 100 individuals referred to the service.
Methods
Service background
Following the publication of NICE guidance on alirocumab and evolocumab,13 14 a steering group of leading cardiologists, pharmacists and lipidologists from the Leeds area was formed. Their purpose was to design a local service for PCSK9i initiation and management in eligible patients.
The group agreed that PCSK9i prescribing should be restricted to secondary care, to ensure necessary specialist input, reduce the risk of initiation in ineligible patients and facilitate appropriate monitoring. In addition, the cost of PCSK9is is lower in secondary care, creating a saving that could be passed to local clinical commissioning groups. Commissioners were engaged early in the planning process to ensure that the service met their needs.
Service design
The model is based on a centralised multidisciplinary service hosted by the Cardiology Department of LTHT, as part of their Cardiology Outpatient Innovative Medicines Optimisation Service (figure 1). This clinic, known as the ‘Leeds Innovative Medicines Clinic’, is the sole PCSK9i prescriber in the area.
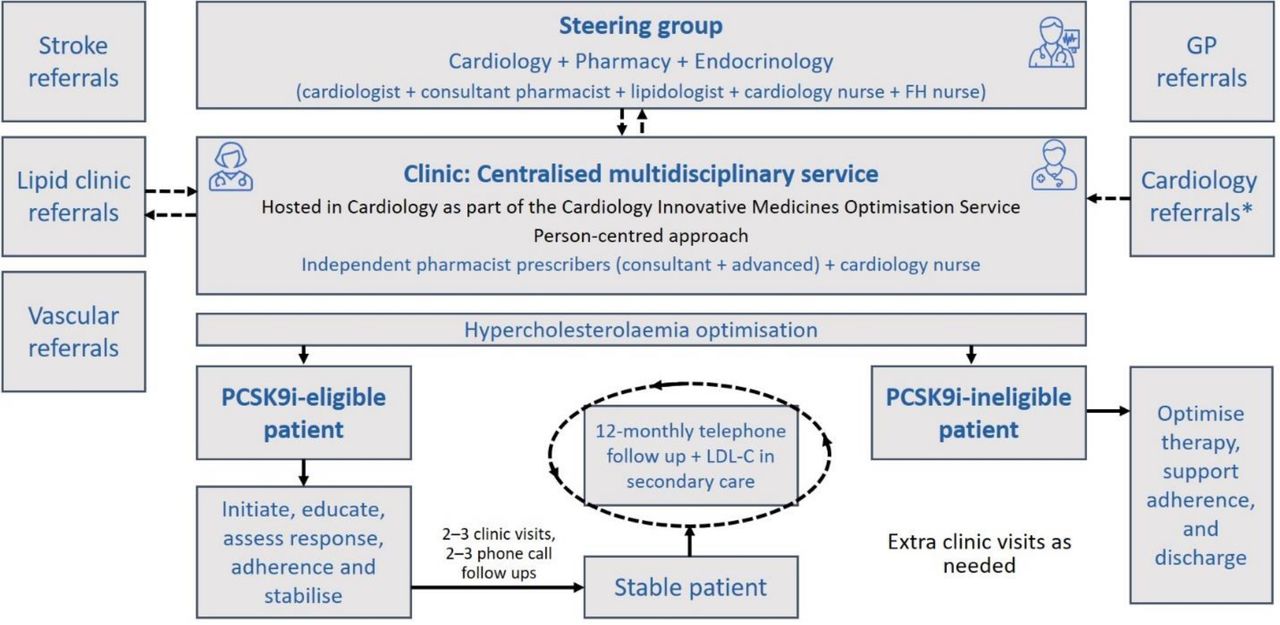
Multidisciplinary PCSK9is clinic: a schematic diagram of the overall model. GP, general practitioner; PCSK9is, proprotein convertase subtilisin/kexin type 9 inhibitors.
Several key items were developed ahead of the launch:
A service guideline and clinic pathway to enable screening of referred patients against NICE criteria for PCSK9i initiation.
Full guidance on statin intolerance and its management, to ensure PCSK9i prescribing only for appropriate patients.
A registry to collect response data and patients’ treatment experiences.
Patient and public involvement
Prior research and feedback from patients attending our Post MI Medicines Optimisation clinic revealed the need for this service to fill a gap in lipid optimisation.17 There was a high prevalence of statin intolerance among this population. We sought feedback from patients who attended this new service by sending them feedback surveys to complete and post back to us using a prepaid envelope. It was then up to the patient if they wanted to complete the survey and send back. Patients will be informed of the findings in public talks and also dissemination via newsletters.
The running of the clinic
Day-to-day clinic activities are led by independent pharmacist prescribers (consultant cardiology pharmacist and advanced cardiology pharmacists), supported by a cardiology nurse and (recently) a pharmacy technician. Referrals can come from various secondary care departments, as well as primary care (figure 1). Referring physicians must provide the patient’s medical history (including a full lipid profile and any possible diagnosis of FH), lipid-lowering medicines prescribed, medicines intolerances, relevant comorbidities and the reasons for considering PCSK9i therapy. All patients are discussed by the clinic team; when necessary, the steering group can be contacted for further advice. Patients can also be discussed at biweekly multidisciplinary team meetings.
The service runs two clinics per week. Suitable patients are assessed using a person-centred approach to explore current and potential lipid medicines optimisation needs, and a decision is made on PCSK9i eligibility as per NICE guidelines.13 14
Patients deemed ineligible are provided with support to optimise therapy and adherence, and the importance of diet and lifestyle is emphasised. They are then discharged.
For PCSK9i-eligible patients, appropriate blood tests are undertaken at baseline (eg, full blood counts, full lipid profile, thyroid function tests, liver function tests and urea and electrolyte profiles). There is no preference for one PCSK9i over the other, except in cases of latex allergy, which rules out evolocumab. With alirocumab, a dose of 150 mg every 2 weeks is preferred, and the 75 mg dose is only used to address patient-related factors (eg, concerns about adverse events and reluctance to use a higher dose).
Those who agree to try a PCSK9i are provided with education on the medicine, safe storage, administration (as an injectable drug) and disposal after use. Patients administer the first dose in clinic under healthcare supervision and a second is provided for home administration 2 weeks later. All patients can call the clinic team directly, if needed. They are also followed up with at least two phone calls to check they are happy with the medicine, ensure correct usage and discuss any side effects. A final decision is subsequently made by the patient and clinic team on whether to proceed with therapy. Only then are patients supplied with further doses. The clinic team takes a proactive role in arranging prescriptions and medicine deliveries. Clinic visits are offered at 3 months and 6 months to evaluate response and address any adverse events or adherence issues. PCSK9i therapy is continued for as long as patients show a good response and are considered adherent.
Overall, the service takes a person-centred approach, providing full support to optimise adherence and reduce medicines wastage.
Impact of COVID-19 pandemic
During the pandemic, a revised method was adopted. Face-to-face clinics were replaced with telephone consultations to assess eligibility and gather clinical histories. If suitable, a nurse visited the patient (in full personal protective equipment) to provide advice on drug administration. Follow-up calls remained in place and a review was performed at 3 months to assess response. Those already established on PCSK9i therapy were converted to telephone follow-ups.
Assessments
The present analysis is a retrospective review of data from the first 100 patients referred to the service between February 2017 and July 2018.
Baseline characteristics were recorded for all patients, including sex, age, source of referral, CVD status, lipid profile and lipid-lowering treatment history. Prescribing of PCSK9i therapy was documented, as well as the impact on full lipid profile at 3 months and 12 months. Other blood tests were included for the purpose of this study as mentioned earlier, including glycated haemoglobin (HbA1c) levels at baseline and at 12 months. Any patients that discontinued or moved away were also recorded.
When necessary, statin intolerance was assessed as per guidance from NICE and the Accelerated Access Collaborative (AAC): based on the presence of clinically significant adverse effects that represent an unacceptable risk to the patient or that may reduce compliance; or adverse events considered unacceptable by the patient and/or some laboratory abnormalities, both attributed to statin treatment and leading to its discontinuation.18 According to our protocol, the patient was also required to have tried at least two statins.
After their 3-month review, patients were asked to rate their experiences using an anonymous feedback questionnaire, which was posted out for completion in their own time.
Statistical analyses
Descriptive statistics are provided throughout, including mean, SD and range for continuous variables, and frequency and percentage for categorical variables. Paired t-tests were used to assess changes in mean LDL-C at 3 months and 12 months and HbA1c at 12 months. A two-tailed p value of <0.05 was considered to be statistically significant.
Results
Referrals to the PCSK9i clinic
Among the first 100 patients referred, 62 (62%) were male and 38 (38%) were female; the mean age was 62.9±10.5 years (range: 39–83 years) (table 2). The majority were referred by a cardiologist (n=68; 68%) or lipid clinic (n=29; 29%). Eighty patients (80%) had documented CVD. In total, 21 individuals (21%) had FH, 58 (58%) had non-FH and 21 (21%) had possible FH based on Simon Broome Criteria,19 requiring further investigations. Mean total cholesterol was 6.6±1.9 mmol/L (range: 2.2–12.2 mmol/L) and mean LDL-C was 4.0±1.8 mmol/L (range: 0.7–9.8 mmol/L).
Baseline characteristics of the first 100 patients referred
Fifty-six patients (56%) were considered to have some degree of intolerance to at least one statin. On presentation, 33 patients (33%) were receiving atorvastatin and 39 (39%) were on rosuvastatin, 36 (36%) were taking ezetimibe plus a statin (atorvastatin, n=11; rosuvastatin, n=18; pravastatin, n=2; and simvastatin, n=5) and 28 (28%) were on ezetimibe monotherapy.
Patients eligible for PCSK9i
On review within the clinic, 52 patients (52%) were considered to be eligible for PCSK9i therapy based on NICE criteria (table 3).13 14 Four of the 52 patients (8%) declined due to fear of injectable medication or believing that use of injection was a marker of ‘advanced’ or ‘bad’ state; they were started on a statin. The remaining 48 were initiated on PCSK9i therapy with either evolocumab (n=33/48; 69%) or alirocumab (150 mg dose, n=9/48 (19%); 75 mg dose, n=6/48 (12%)). Of these, 36 (75%) were on a statin prior to starting PCSK9i therapy and continued this after initiation of a PCSK9i.
Prescribing based on review in the multidisciplinary PCSK9i clinic
At 3 months, 2 patients on alirocumab 75 mg and 1 on alirocumab 150 mg were started on ezetimibe due to poor response (LDL-C reduction <25%). The addition of ezetimibe produced mean reductions in LDL-C of >45%. One individual also had fenofibrate reinstated because triglyceride levels were increased. Although switching from alirocumab to evolocumab was an option for these patients, they preferred the addition of oral ezetimibe.
Seven of the 48 patients (15%) given a PCSK9i stopped treatment within the first year due to adverse events (n=5) or non-adherence (n=2). One person transferred to another centre.
Ineligible patients
The remaining 48 patients (48%) were considered ineligible for PCSK9i treatment (table 3). Twenty-five were already on a statin. Among these 48 individuals, 13 (27%) continued on the same therapy, 10 (21%) were started on ezetimibe (n=8 already on a statin and ezetimibe added and n=2 initiated as monotherapy) and 12 (25%) were started on a statin (rosuvastatin, n=11; and atorvastatin, n=1). Two patients (4%) already on statin therapy were switched to a more potent statin, and 1 (2%) had their dose doubled to optimise therapy. One patient (2%) declined pharmaceutical therapy and elected to modify their diet and increase exercise to lower cholesterol. A further 7 individuals (15%) were discharged because they were already medically optimised, and 2 (4%) declined further input.
Statin intolerance
Seventeen patients were identified as intolerant to statins. After visiting the clinic, 12 of these (71%) were initiated on a statin and tolerated it, while the remaining 5 (29%) either declined or had true statin intolerance.
Response to PCSK9i therapy
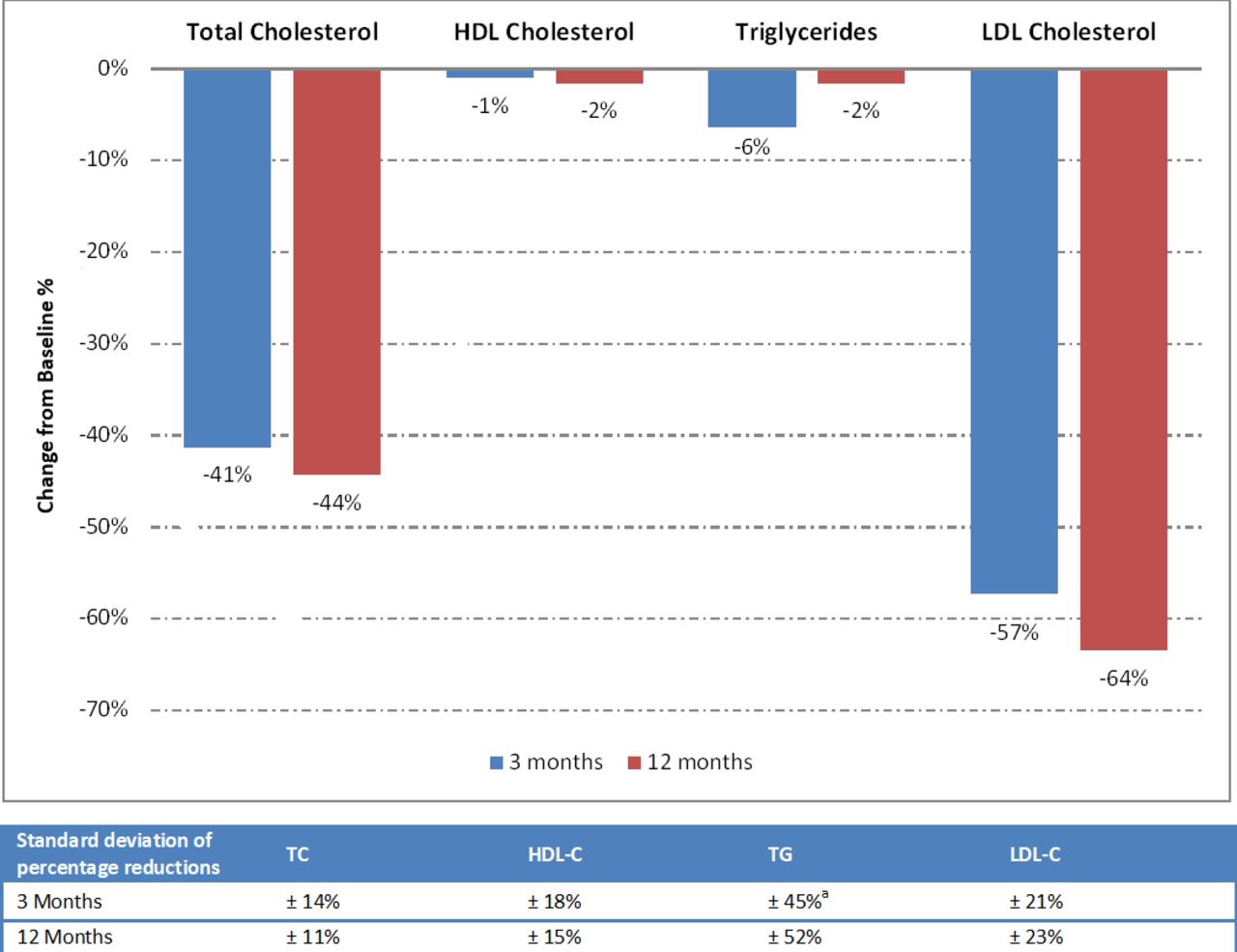
Of the 48 patients initiated on PCSK9i therapy, 40 continued treatment for 12 months in our centre (table 4; figure 2). Mean total cholesterol decreased from 7.7±1.6 mmol/L (range: 5.1–12.2 mmol/L) at baseline to 4.5±1.4 mmol/L (range: 2.4–7.7 mmol/L; 41% reduction) at 3 months, and to 4.3±1.2 mmol/L (range: 1.9–7.4 mmol/L; 45% reduction from baseline) at 12 months. Similarly, mean LDL-C decreased from 5.0±1.6 mmol/L (range: 1.4–8.9 mmol/L) at baseline to 2.1±1.3 mmol/L (range: 0.5–5.2 mmol/L) at 3 months, and to 1.7±1.1 mmol/L (range: 0.2–5.1 mmol/L) at 12 months. Thus, at 3 months, there was 58% reduction from baseline in LDL-C (p<0.0001), and at 12 months there was a 65% reduction from baseline in LDL-C (p<0.0001 vs baseline; p=0.0013 vs 3 months). Median LDL-C also decreased substantially, from 4.8 mmol/L at baseline to 1.6 mmol/L at 3 months and 12 months (67% reduction).

{kind=link}
{kind=link}
Change from baseline in lipid profile among PCSK9i-treated patients. aOne patient was on fenofibrate, discontinuation of fenofibrate led to significant elevation of TG at 3 months and, therefore, fenofibrate was reinstated before the 12 months reading. This result was excluded from the graph. HDL-C, high-density lipoprotein-cholesterol; LDL, low-density lipoprotein-cholesterol; PCSK9i, proprotein convertase subtilisin/kexin type 9 inhibitor.
Lipid profile among PCSK9i-treated patients
Among the 40 patients receiving 12 months of PCSK9i treatment, 25 were on a statin at the time of initiation and 15 were not. Reductions in LDL-C at 3 months were higher among those receiving combination therapy versus PCSK9i alone. In the combination group, mean LDL-C fell from 4.9±1.8 mmol/L (range: 1.4–9.8 mmol/L) at baseline to 1.7±1.4 mmol/L (range: 0.4–4.1 mmol/L) at 3 months, representing a 65% reduction. By comparison, in patients initiated on PCSK9i without a statin, mean LDL-C decreased from 4.9±1.5 mmol/L (range: 2.4–8.9 mmol/L) to 2.0±1.0 mmol/L (range: 0.5–4.9 mmol/L), equivalent to a 59% reduction.
Nineteen of the 40 (48%) patients on PCSK9i had FH (n=8 primary prevention and n=11 secondary prevention) and 21 (52%) were non-FH (all secondary prevention). At 12 months, the mean reduction in LDL-C from baseline was 62% in the FH primary prevention group (from 6.0±1.1 mmol/L to 2.3±1.4 mmol/L), 66% in the FH secondary prevention group (from 5.9±2.6 mmol/L to 2.0±1.3 mmol/L) and 71% in the non-FH secondary prevention group (from 4.4±0.8 mmol/Lto 1.3±0.6 mmol/L).
Of the 48 patients initiated on PCSK9i treatment, 11 (23%) had diabetes, 10 (21%) had pre-diabetes and 27 (56%) did not have diabetes. Mean HbA1c levels were not significantly different between baseline (46.3±12.8 mmol/mol) and 12 months (45.4±11.7 mmol/mol; p=0.46).
Meeting targets
Fifteen patients (79%) with FH (both primary and secondary prevention) met the NICE target of ≥50 reduction in LDL-C, and 19 (91%) of the patients with non-FH (secondary prevention) met the NICE target of >40% reduction in non-HDL-C. Patients who did not meet NICE targets were on PCSK9i monotherapy and declined the use of statins or ezetimibe due to a history of intolerance.
With regard to ESC targets, 3 patients at high risk (37%) achieved an LDL-C reduction of ≥50% and LDL-C <1.8 mmol/L, and 15 patients at very high risk (40%) achieved an LDL-C reduction of ≥50% and LDL-C <1.4 mmol/L. Except for one patient, all those who did not meet the ESC targets were either on PCSK9i monotherapy or PCSK9i+ezetimibe (every other day or once weekly regimen). One patient was on alirocumab 75 mg, ezetimibe and low-dose statin.
Safety
Among the 48 patients initiated on PCSK9is, most reported transient adverse events, including injection-site reactions (n=2/48; 4%), influenza-like symptoms (n=12/48; 25%), fatigue/lethargy (n=10/48; 21%) and musculoskeletal pain (n=4/48; 8%) (table 5). Six individuals (13%) reported transient nausea within the first month of treatment. All of these subsided for patients within the first 3 months of use and patients continued with therapy. Fourteen out of the 48 patients (29%) did not report having any transient side effects or any reaction. As a result of possible minor treatment-related side effects (injection-site tenderness and lethargy), 2 individuals were switched from evolocumab to alirocumab 75 mg and were able to continue therapy as side effects subsided.
Adverse events with PCSK9is
Patient feedback
Feedback forms were provided to all patients who attended the clinic. Of the first 77 to attend, 31 completed the questionnaire (40% response rate) (table 6). Twenty-three respondents had been prescribed a PCSK9i.
Results from the anonymous feedback questionnaire
Among those responding, 20/23 (87%) agreed or strongly agreed that the medicine was easy to administer, and 22/23 (96%) were happy with their PCSK9i and felt it fulfilled its purpose. Almost all (n=22/23; 96%) were satisfied with the information provided regarding storage, administration, disposal and possible side effects of PCSK9i.
Regardless of PCSK9i prescribing, 26/26 respondents (100%) agreed or strongly agreed that their medicine-related questions and concerns were addressed. Almost all respondents agreed or strongly agreed that: they were provided with clear plans and goals around their cholesterol-lowering medicines, any tests that they needed, and their health as a whole (n=28/29; 97%); after attending the clinic, they fully understood their cholesterol-lowering medicines and why they were prescribed (n=30/30; 100%); and they were confident about using the medicines provided (n=28/29; 97%). All respondents felt supported and listened to (n=31/31; 100%), and found the clinic valuable (n=30/30; 100%). When asked to rate the overall service received, 30/31 (97%) were satisfied or very satisfied.
Discussion
We have developed a novel, person-centred, centralised, multidisciplinary clinic for the assessment and follow-up of patients potentially eligible for PCSK9i therapy. The model ensures that individuals are assessed by relevant specialists in secondary care, and only those meeting NICE criteria13 14 are initiated on a PCSK9i. Data from the first 100 patients suggest that the model is suitably discerning—only around half of those referred were ultimately offered a PCSK9i.
Appropriate patient selection for PCSK9i treatment is particularly important given their high cost and the overall burden of education and monitoring. This aligns with current international guidelines from Europe2 and the USA,20 which advise restricting their use to appropriately selected patients at high risk in order to optimise economic value. Once a PCSK9i is initiated at our centre, patient follow-up, monitoring and support are actively undertaken within the clinic framework. This may help to maximise benefit, bolster adherence and reduce medicines wastage.
Access to PCSK9is has become a key priority in the UK after figures showed that initial uptake was disappointing: around 70% lower than expected over the first 2 years.21 Recent Europe-wide data from the DA VINCI observational study also showed low use of PCSK9is, even though it was associated with increased achievement of LDL-C goals.22 This suggests that many patients are missing out on effective treatment. The UK AAC—which brings together the NHS, government and industry to remove barriers to the uptake of novel medicines—has selected PCSK9i treatment as a focus area.23 The role of the AAC is to facilitate increased adoption, optimised process development, and the generation of real-world data. The LTHT model supports these goals.
Specific barriers to PCSK9i use highlighted by the AAC include21 23: limited and inconsistent access pathways; lack of incentives and initiatives driving cholesterol management; lack of routine recording of LDL-C levels required to initiate a PCSK9i; restricted prescribing, leading to long waiting times; and limited awareness among healthcare professionals of the unmet need that can be addressed with PCSK9is. Our model has the potential to address all of these barriers, and indeed has already successfully eradicated some within our centre.
The multidisciplinary nature of the service is valuable in allowing all relevant healthcare professionals to contribute to lipid management. Nonetheless, on a day-to-day basis, it is led by pharmacist prescribers (consultant and advanced), with consultant cardiologists and lipidologists available when needed. Respondents to the patient feedback questionnaire expressed no dissatisfaction with this arrangement. Importantly, the pharmacist-led model frees up time in cardiology and lipidology clinics, creating greater outpatient capacity. Pharmacist-led PCSK9i provision has previously been successfully implemented at centres in the USA.24 25 The focus of these US pharmacy models was on screening for eligibility, recommending alternative lipid-lowering therapies for ineligible patients, facilitating insurance claims and delivery of PCSK9i supply. In our model, pharmacists reviewed patients in clinic, prescribed PCSK9i and other lipid-lowering therapies, monitored for safety and efficacy, and closely followed up patients to address concerns, support adherence and further optimise lipid-lowering therapy where needed; treatment response and patient satisfaction with the service were formally evaluated. We have also successfully deployed a similar pharmacist-led model of medicines optimisation in patients with post-myocardial infarction.26
Our real-world data suggest that PCSK9i therapy was effective, leading to large and sustained reductions in total and LDL-C. In patients treated for 12 months, mean LDL-C levels fell from 5.0 mmol/L to 2.1 mmol/L, substantially closer to the target levels proposed in international guidelines.2 Furthermore, with regard to NICE targets, 79% of patients with FH (both primary and secondary prevention) achieved a ≥50% reduction in LDL-C, and 91% of patients with non-FH (secondary prevention) attained a >40% reduction in non-HDL-C. Achievement of ESC targets was somewhat lower (37% in patients at high risk and 40% in patients at very high risk) demonstrating that these are more challenging to achieve. Patients who could not meet either NICE or ESC targets were mainly on PCSK9i monotherapy. These findings show that meeting NICE and ESC targets requires the use of multiple lipid lowering therapies concomitantly.
There were no major safety concerns with PCSK9i therapy, and <10% of patients experienced (transient) musculoskeletal pain even though some had experienced such symptoms with prior statin therapy. This aligns with data from the GAUSS-3 trial, which showed modest rates of musculoskeletal AEs—and very few resulting discontinuations (<1%)—in patients with muscle-related statin intolerance who were then initiated on evolocumab.27
Our clinic also offers medicines optimisation and adherence support in PCSK9i-ineligible patients. This includes issues around statin intolerance, and many individuals were able to restart statin therapy having previously been considered intolerant. There are data to suggest that stopping and then re-initiating statins can result in improved tolerance. For example, in a study of 11 124 patients in whom statins were discontinued at least temporarily because of clinical events or symptoms believed to have been caused by statin use, 92% of those who were rechallenged were still taking a statin 12 months after the initial event.8
Overall patient satisfaction with the clinic model and PCSK9i therapy was high. Questionnaire respondents who initiated a PCSK9i were almost all happy with the drug and felt that it fulfilled its purpose. Furthermore, irrespective of PCSK9i prescribing, clinic attendees agreed that they felt listened to, were provided with clear lipid-lowering plans, and would recommend the service to others. The clinic model aligns with local and international guidance on person-centred care and shared decision-making.28 29
Our model was considered to be cost effective by the commissioners for multiple reasons:
The prescribing of PCSK9i in secondary care under the patient access scheme (as per NICE13 14) provided a discount on the cost of PCSK9i injections.
It reduced wastage of PCSK9i by providing limited supply and following patients regularly.
The service supported improved adherence to PCSK9i (although there is potential for adherence to decrease in the long term).
It improved the lipid management of patients who were not eligible for PCSK9i, thus providing additional lipid-lowering benefit.
Overall, the service succeeded in lowering LDL-C among PCSK9i-treated patients by an average of around 3 mmol/L. If these reductions are maintained, they would be expected to bring important clinical benefits, with a stepwise decrease in atherosclerotic CVD risk as LDL-C is reduced. Indeed, it has been estimated that each 1 mmol/L reduction in LDL-C is associated with a 22% relative risk reduction for major vascular events.30
Because the NICE threshold for initiating PCSK9i is higher (our patients had a mean baseline LDL-C of 5.0±1.6 mmol/L), we would expect favourable cost effectiveness based on the findings of the ODYSSEY OUTCOMES cost-effectiveness analysis for PCSK9i, which found it to be cost effective in patients with an LDL-C ≥2.6 mmol/L.31
We should acknowledge the limitations of this study. The sample size was small and only around half were offered PCSK9i, so care should be taken in extrapolating to larger populations. Furthermore, the study design was retrospective and had no comparator arm. A prospective, randomised controlled trial would be valuable. In addition, not all patients completed the feedback questionnaire and those that did so may have been somewhat self-selecting for greater satisfaction with the service. Nonetheless, the response rate was acceptable and the questionnaire results align with wider anecdotal opinions.
Overall, the data suggest that our innovative, centralised, pharmacist-led, multidisciplinary clinic can be successfully employed to select patients for PCSK9i therapy—and drive long-term monitoring, adherence and ultimately LDL-C lowering. Importantly, the service also addresses statin intolerance and provides appropriate medicines optimisation and adherence assistance even in PCSK9i-ineligible patients. The model is flexible enough to allow the introduction of other novel medications for cholesterol lowering, and this is now happening following the recent incorporation of bempedoic acid and inclisiran into the clinical pathway. These new agents have been shown to significantly reduce LDL-C,32 but outcomes data have not yet been reported.
In line with the goals of the AAC, our model could be duplicated elsewhere in the country to support better uptake and optimisation of PCSK9is and other novel treatments.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
The study was conducted in accordance with the Declaration of Helsinki. As this was a service development programme, no ethics ccommittee approval was needed, in line with local policy. However, the steering group continues to regularly monitor the service.
Acknowledgments
We thank Shaista Afzal, Eman Ali, Charlotte Daniel, Emily Cutts and Harrison Mycroft for their help with data collection, and Biological Communications for medical writing support, funded by Leeds Teaching Hospitals NHS Trust.
References
Footnotes
Twitter @DrRaniKhatib
Contributors RK led and coordinated the project and drafted the manuscript. EI screened the studies for eligibility and collected and extracted data. MK extracted and synthesised the data. MK and RK led interpretation and discussion of the results. All authors MM, AH and CB critically revised the manuscript. All authors approved the final version of the article. RK is the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors. However, the service was commissioned and fully funded by the Leeds Clinical Commissioning Group based on the data presented in this article.
Competing interests Nothing to declare. RK received speaker fees from Sanofi.
Provenance and peer review Not commissioned; externally peer reviewed.