Article Text

Abstract
Background The COVID-19 pandemic has disrupted healthcare systems across the world. The rate of acute coronary syndrome (ACS) admissions during the pandemic has varied significantly.
Objectives The purpose of this study is to investigate the effect of the pandemic on ACS hospital admissions and to determine whether this is related to the number of COVID-19 cases in each country.
Method Search engines including PubMed, Embase, Ovid and Google Scholar were searched from December 2019 to the 15 September 2020 to identify studies reporting ACS admission data during COVID-19 pandemic months in 2020 compared with 2019 admissions.
Results A total of 40 studies were included in this multistudy analysis. They demonstrated a 28.1% reduction in the rate of admission with ACS during the COVID-19 pandemic period compared with the same period in 2019 (total of 28 613 patients in 2020 vs 39 225 in 2019). There was a significant correlation between the absolute risk reduction in the total number of ACS cases and the number of COVID-19 cases per 100 000 population (Pearson correlation=0.361 (p=0.028)). However, the correlation was not significant for each of the ACS subgroups: non-ST-elevation myocardial infarction (STEMI) (p=0.508), STEMI (p=0883) and unstable angina (p=0.175).
Conclusion There was a significant reduction in the rate of ACS admission during the COVID-19 pandemic period compared with the same period in 2019 with a significant correlation with COVID-19 prevalence.
- COVID-19
- myocardial infarction
- acute coronary syndrome
Data availability statement
Data are available in a public, open access repository. All data included are published in previous manuscripts, included in the references.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
A COVID-19 pandemic has a huge impact on healthcare systems across the world.
What does this study add?
How did COVID-19 affect acute coronary syndrome (ACS) admissions rate globally.
There is a correlation between the drop of ACS admission rate and the number of COVID-19 cases in each country.
How might this impact on clinical practice?
It highlights the importance of increasing the public awareness about presenting with ACS during the pandemic if required.
Healthcare systems need to be prepared to face the potential consequences of late and missed ACS presentations.
Introduction
The SARS-CoV2 viral pandemic has disrupted healthcare systems across the world, forcing them to efficiently adapt to the overwhelming increase in acutely and devastatingly ill patients diagnosed with COVID-19.1–3 During this period, acute coronary syndrome (ACS) admissions have been lower than the pre-pandemic admission rates.4 This phenomenon has been observed worldwide and has been attributed to the increased patient concern of presenting to the hospital, improved medication compliance and less physical strain, and decreased levels of pollution and smoke exposure due to quarantine measures.5
The purpose of this multistudy analysis was to investigate the impact of COVID-19 pandemic on hospital admissions for ACS and study the relation to published numbers of COVID-19 infections per 100 000 of the population in each country.
Methodology
Preferred Reporting Items for Systemic Reviews and Meta-Analyses statement was followed for the conduct and reporting of this meta-analysis.6
Data source, search strategy and inclusion
To identify all the studies demonstrating the impact of the COVID-19 pandemic on the number of hospital admissions for patients with ACS, PubMed, Embase, Ovid and Google Scholar were carefully searched for any published data from December 2019 to the 15September 2020.
The following search keywords were used alone or in combination: ‘novel coronavirus’, ‘SARS-CoV2’, ‘COVID-19’, ‘ACS’, ‘cardiovascular disease’, ‘cardiac injury’, ‘STEMI’, ‘non-STEMI’ and ‘unstable angina.
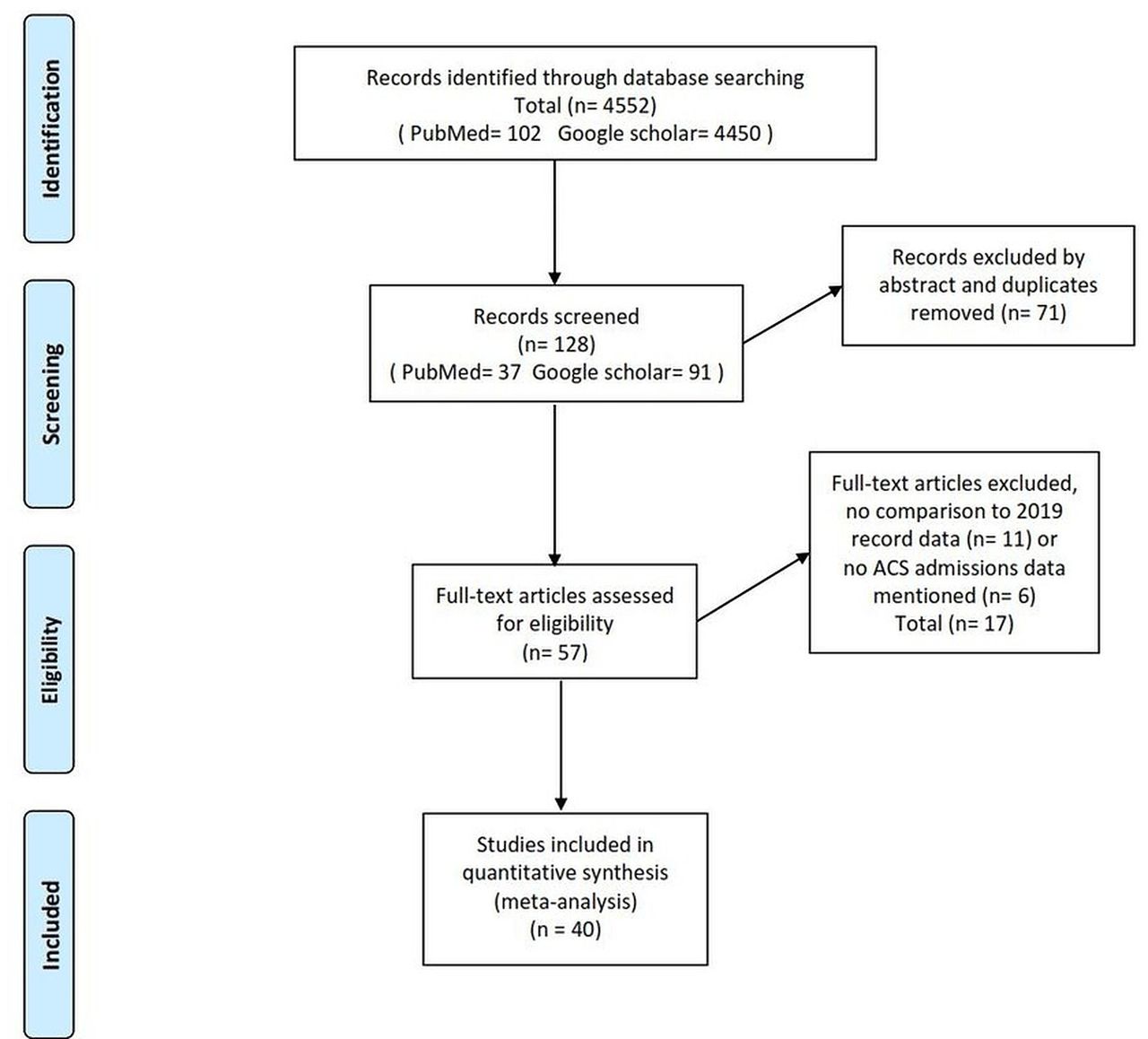
Inclusion criteria for this multistudy analysis were any comparative study published in English or has a published English translation reporting ACS admission data during COVID-19 pandemic months and comparing it to 2019 admission data. The pandemic month was identified by the detection of the first case of COVID-19 according to the study original country. Studies without adequate admission data or no comparison to 2019 were excluded.(figure 1)

Meta-analysis screening system. ACS, acute coronary syndrome.
Data extraction and study quality assessment
According to the study, any reported data for ACS, non-ST-elevation myocardial infarction (STEMI), STEMI or unstable angina (UA) admission numbers in 2019 and 2020 were extracted. In addition to the date of the first recognised case of COVID-19. The primary outcome measure was to compare the number of admissions in both years. Newcastle-Ottawa scale was used to assess the quality of the studies.
Data synthesis and statistical analysis
The data are described as mean±±SD, median, range and IQR or frequencies (number of cases) and percentages when appropriate. Absolute risk reduction (reduction in the number of COVID-19 cases, ARR) between 2019 and 2020 was calculated for each of the included studies. Correlation between ARR and number of COVID-19 cases/100 000 population was evaluated using Pearson moment correlation equation. Statistical calculations were performed using SPSS V.22 (IBM).
Results
A total of 40 studies were included in this analysis. They demonstrated a reduction of 28.1% in rates of admission in patients with ACS during the COVID-19 19 pandemic period compared with the same period in 2019 (total of 28 613 patients in 2020 vs 39 225 patients in 2019) (table 1) figure 2.(figure 3)
Details of the enrolled studies showing the number of ACS cases admitted during 2019 and 2020
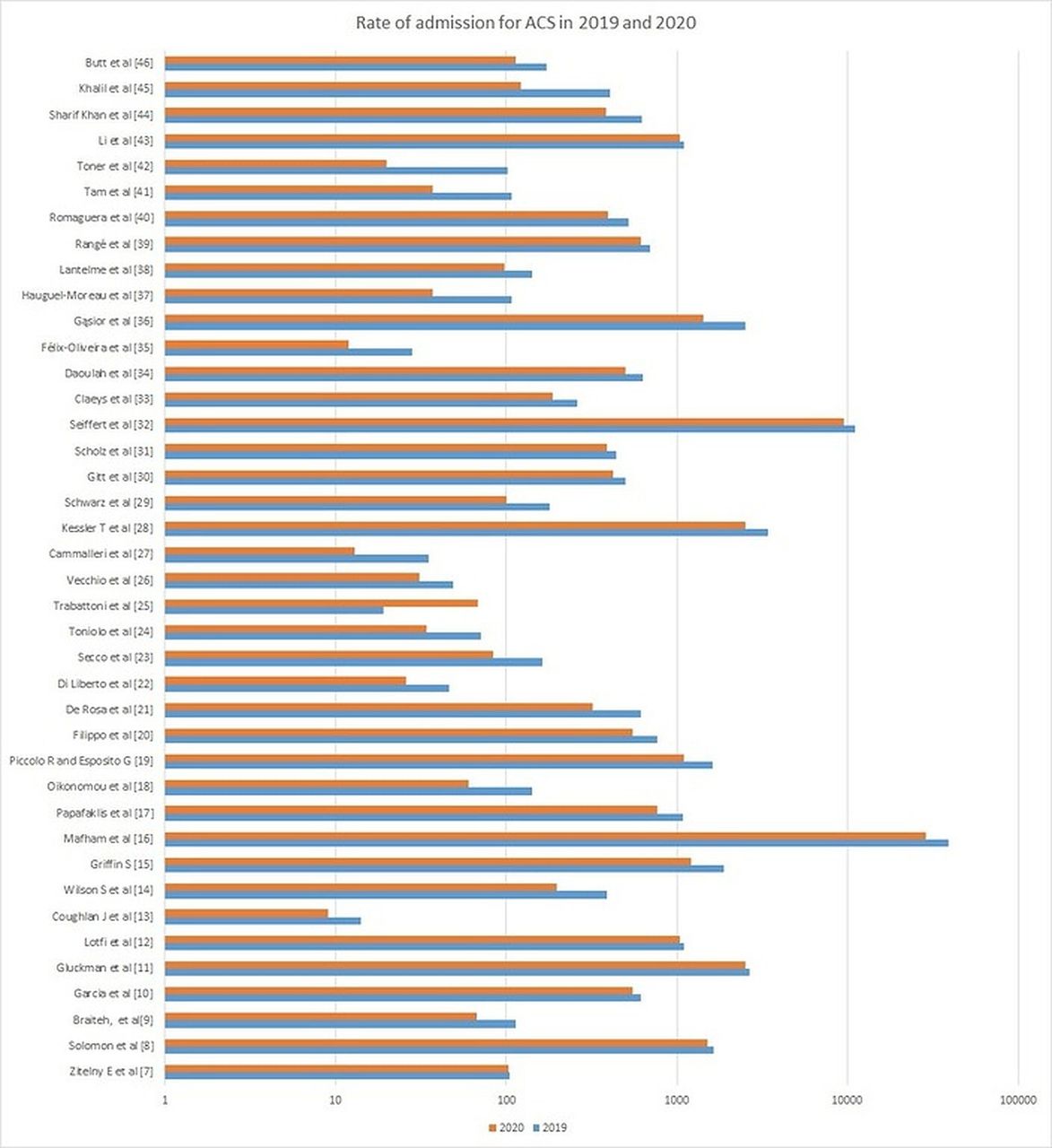
Rate of admissions with acute coronary syndrome (ACS) across all papers included.

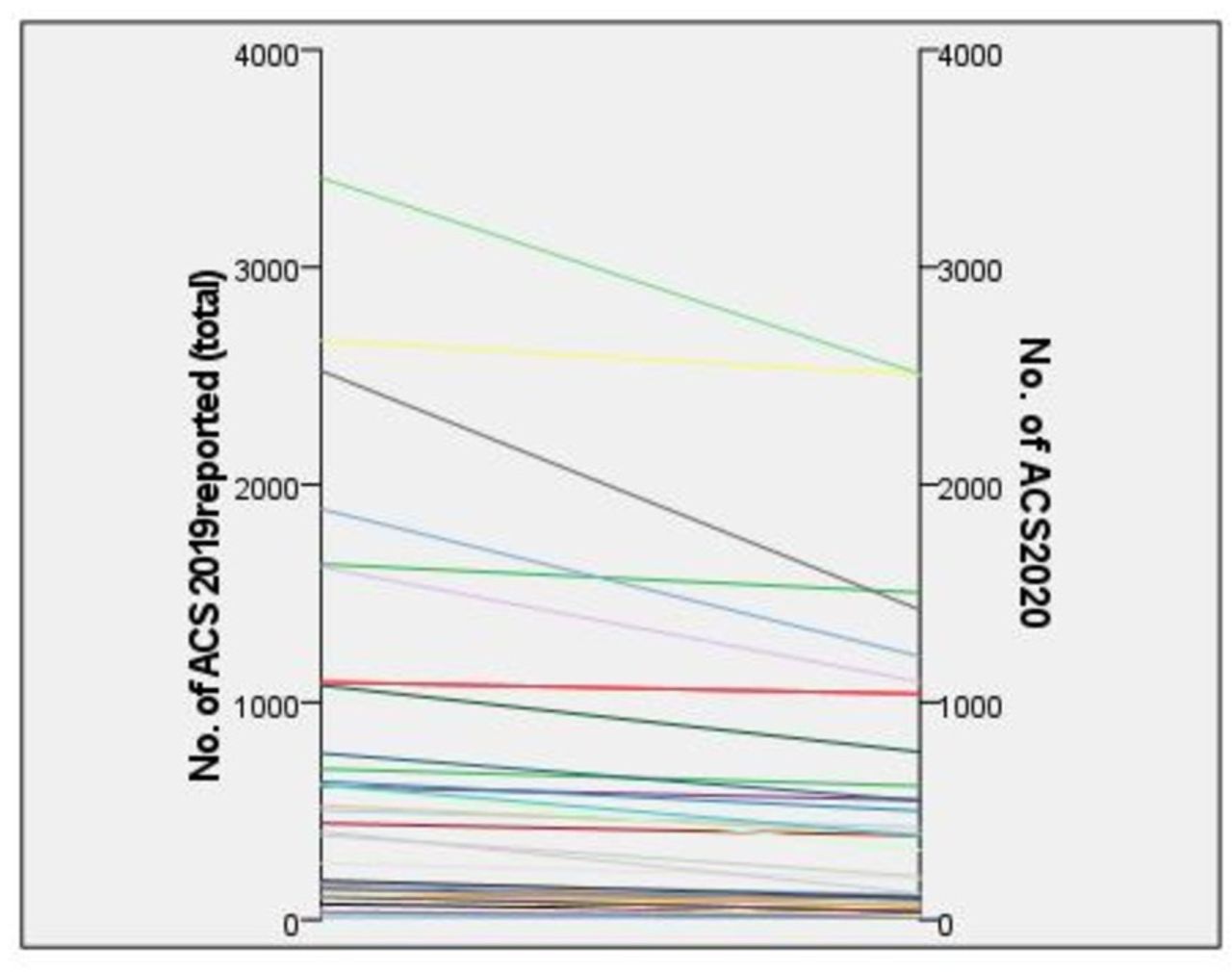
The number of acute coronary syndrome (ACS) admissions in 2019 and 2020 in each study.
Only 16 studies provided a subgroup analysis for ACS which in total demonstrated a reduction in cases admitted in 2020 compared with that of 2019 with a 21.9% reduction in STEMI cases (9374 vs 11 839 patients, respectively), 27% reduction in NSTEMI (10 855 vs 14 671 patients, respectively) and 48.1% reduction in the number of patients admitted with UA (343 vs 545 patients, respectively) (figure 4).
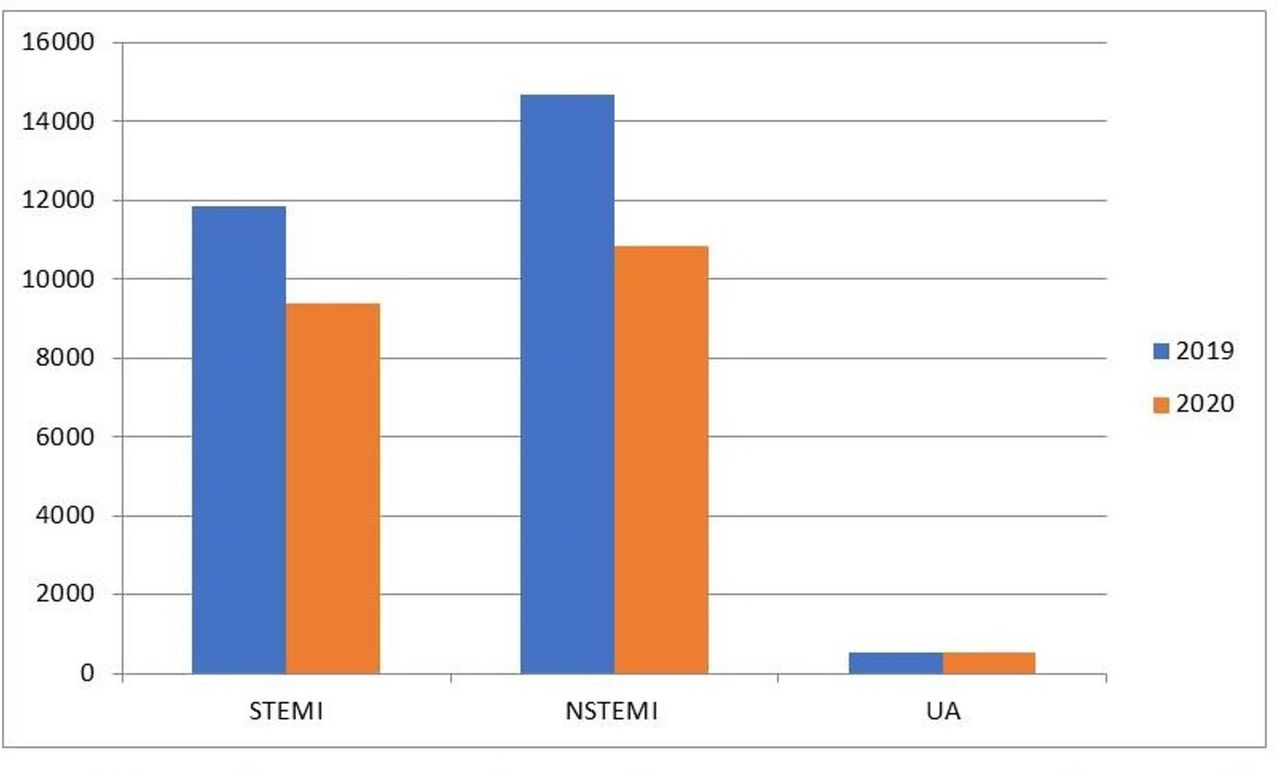
Comparison between the number of admissions with STEMI, NSTEMI and UA in 2019 and 2020. NSTEMI, non-ST-elevation myocardial infarction.
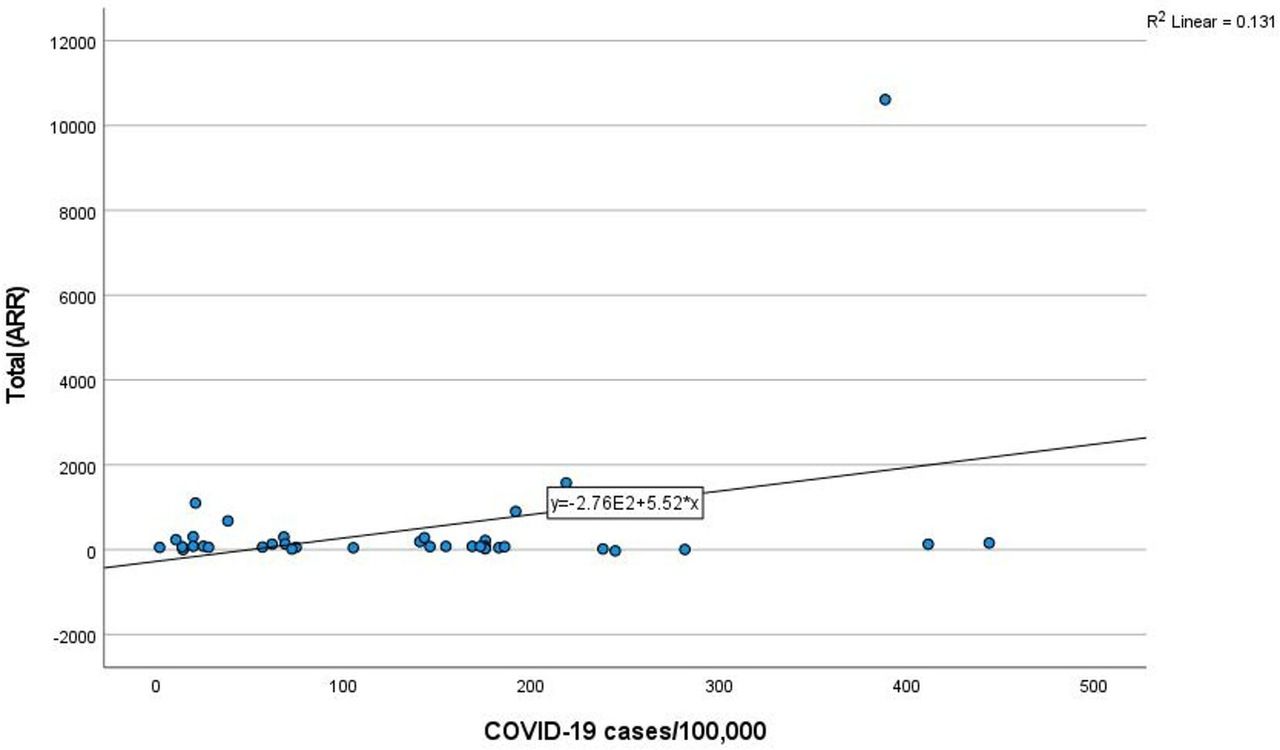
There was a positive correlation between the ARR in the total number of ACS cases and the number of COVID-19 cases per 100 000 population in published each country (Pearson correlation=0.361* (p=0.028)) (figure 5).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The correlation between Absolute risk reduction (ARR) of acute coronary syndrome admissions and the published number of COVID-19 cases in each study.
However, the correlation was not significant for each of the ACS subgroups: non-STEMI (p=0.508), STEMI (p=0883), and UA (p=0.175).
Discussion
The emergence of Coronavirus SARS-CoV-2 in Wuhan, China in December 2019 has led to global healthcare system changes. One of which is the number of patients admitted in hospitals including ACS cases. How COVID-19 is affecting admissions and management of myocardial infarction is a matter of concern, as medical resources have been massively reorientated, and the population has been in lockdown.
Nearly all studies reported a decrease in ACS cases except for two studies undertaken in Australia and Taiwan where early measures were taken to limit the virus spread.7 8 However, in Greece where similar early precautions were implemented, there was still a significant reduction in admissions recorded as well.9 10
Some viral illness, like SARS-CoV and MERS-CoV, was noted to increase in acute cardiovascular events rate in infected patients. Similar effect was expected in patients with SARS-CoV-2 infections who also develop general proinflammatory and hypercoagulative status, explaining the frequent in-hospital acute coronary events observed.11 The paradoxical phenomenon of decline was observed after the first disease outbreak news from the WHO had been issued 5 January, 2020 and by the beginning of nationwide lockdowns, suspension of elective procedures and precautionary stay at home measures following declaration of COVID-19.12 These measures, however, helpful in reducing the diffusion of SARS-CoV-2 infection, significantly modified patients’ responses to non-SARS-CoV-2 medical conditions, including ACS. Whether this decrease was due to the lockdown measures implemented, fear of Hospital transmission or decrease in stressors and environmental pollution and triggers for ACS remains to be investigated.
There have been suggested reasons for the decline of ACS admissions; however we do not have any data to say which were more important. Avoidance of hospitals and adherence to social distancing recommendations might be one of the important causes since the highest decline was observed mainly in the early weeks of the pandemic in most countries as well as the positive correlation we identified between the burden of COVID-19 cases and the absolute reduction in ACS cases. Even though the reduction was still found in countries spared by COVID-19 infection or where the infection was minimal,9 13 the inability to find transportation to hospitals and the overwhelming of healthcare systems remains a vital reason in most countries.
Globally, minimising symptoms, reluctance and fear of reaching out to hospitals expressed by delays in symptom to hospital times for fear of infection is probably the cause in many cases; driven by overwhelming messages from authorities and the media about COVID-19, especially that the reduction for ACS types with less severe clinical presentation/symptoms (ie, NSTEMI and UA) was more pronounced. Although an increase in out of hospital cardiac arrest, mortality,14 15 complications and more frequent left ventricle systolic impairment16 were observed, no correlation has been established so far and this link was denied in some countries10 17 and the correlation might be hard to establish.
However, a reason which causes worry might be misdiagnosis and underdiagnosis by doctors who are COVID-19 minded along with overstretched healthcare system since it was emphasised from the very beginning that dyspnoea and chest discomfort were the dominant symptoms of the viral infection, which obviously could be misleading for many patients with ACS.
In Belgium, a decrease in pollution and lower levels of NO2 was found have contributed to a true decrease in ACS cases.18 Other factors suggested are the decrease in physical strain, sympathetic activity and change in diet, less smoking, more adherences to medications, sleep time and reduced common stressors known to cause ACS most notably in the early phases of the lockdown. These factors started to decline in the later weeks due to increased anxiety because of financial insecurity,19 relative liberation of social restriction measures20 as well as increased encouragement of patients with symptoms or signs of ACS to seek immediate medical attention.21
The consequences of this decline of ASC admissions could have a detrimental impact on ACS outcome in terms of increased myocardial impairment, mortality and morbidity. The later can represent a challenge to the cardiology community after the marked reduction in ACS complications in the past decade.
Conclusion
A total of 40 studies from different countries all over the world have shown a reduction in rates of admission in patients with ACS during the COVID-19 pandemic period compared with the same period in 2019, with a positive correlation with the published figure of COVID-19 infection.
Data availability statement
Data are available in a public, open access repository. All data included are published in previous manuscripts, included in the references.
References
Footnotes
AH and LS are joint first authors.
Contributors All authors have contributed equally to this work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.