Article Text

Abstract
Aims It was predicted internationally that transthoracic echocardiography (TTE) would be vital during the SARS-CoV-2 outbreak. We therefore, designed a study to report the demand for TTE in two large District General Hospitals during the rise in the first wave of the SARS-CoV-2 pandemic in the UK. A primary clinical outcome of 30-day mortality was also assessed.
Methods The TTE service across two hospitals was reconfigured to maximise access to inpatient scanning. All TTEs of suspected or confirmed SARS-CoV-2 patients over a 3-week period were included in the study. All patients were followed up until at least day 30 after their scan at which point the primary clinical outcome of mortality was recorded. Comparative analysis based on mortality was conducted for all TTE results, biochemical markers and demographics.
Results 27 patients with confirmed SARS-CoV-2 had a TTE within the inclusion window. Mortality comparative analysis showed the deceased group were significantly older (mean 68.4, SD 11.9 vs 60.5, SD 13.0, p=0.03) and more commonly reported fatigue in their presenting symptoms (29.6% vs 71.4%, p=0.01). No other differences were identified in the demographic or biochemical data. Left ventricular systolic dysfunction was noted in 7.4% of patients and right ventricular impairment or dilation was seen in 18.5% patients. TTE results were not significantly different in mortality comparative analysis.
Conclusion This study demonstrates an achievable approach to TTE services when under increased pressure. Data analysis supports the limited available data suggesting right ventricular abnormalities are the most commonly identified echocardiographic change in SARS-CoV-2 patients. No association can be demonstrated between mortality and TTE results.
- transthoracic
- delivery of care
- tropical infections
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
SARS-CoV-2 infection is associated with increased mortality in those with underlying cardiovascular disease, as well as cardiac injury. Very few studies, however, have assessed the echocardiographic findings of this patient group. Documented abnormalities have included large pericardial effusions and right ventricular dilation or impairment.
What does this study add?
This study is the first to describe how an echocardiography service can be adapted to manage an increase in demand associated with the SARS-CoV-2 pandemic. The findings support previous results suggesting right ventricular anomalies are the most common abnormalities to be found in SARS-CoV-2 patients but question the association between viral infection and pericardial effusions.
How might this impact on clinical practice?
The paper presented acts as a guide to rapid upscaling of echocardiographic services in the context of the SARS-CoV-2 pandemic. This can be easily adapted to the readers’ own hospital. The findings also support the use of new right ventricular dysfunction as a marker of SARS-CoV-2-related cardiac injury.
Introduction
The novel coronavirus 2019 (SARS-CoV-2) is the third beta-coronavirus to have reached pandemic level spread, having taken the lives of over 2.1 million people worldwide at point of writing.1 Specific patient risk factors including older age,2–4 male gender,5 diabetes mellitus,2 6–8 hypertension2 4 6 7 9 and cerebrovascular disease2 4 9 are associated with higher risk of intensive care (ITU) stay or mortality when infected with SARS-CoV-2. However, the most significant comorbidity associated with mortality from SARS-CoV-2 is cardiovascular disease.6 Cardiac injury (CI) has also been repeatedly reported in patients with SARS-CoV-2 with an incidence rate of CI of 7.2%–27.8% in all inpatients.2 3 7 9–12 Those with cardiovascular disease are at higher risk of CI.1 13 Shi et al, however, identified CI (defined as by troponin I levels >99th percentile of upper reference limit) was an independent risk factor for SARS-CoV-2-related mortality.10
Whilst evidence surrounding the cardiac implications of SARS-CoV-2 infection is building, transthoracic echocardiography (TTE) has been viewed internationally as a critical test for those hospitalised with SARS-CoV-2, especially those requiring ITU admission.13–15 Demand has been expected to be high nationally and internationally for TTE during the pandemic in healthcare settings.13–15
The aim of this study was to report the demand and requests for TTE in two large District General Hospitals during the rise in the first wave of the SARS-CoV-2 pandemic in the UK. Additionally, the study aimed to give an overview of the clinical and echocardiographic features of our cohort, with a particular focus on any association between these features and mortality.
Methods
Study design
A prospective observational cohort study was performed across two large UK District General Hospitals in the South West of England. All SARS-CoV-2 suspected or confirmed inpatients who required a TTE between 25 March 2020 and 16 April 2020 were included. Participants were excluded if the TTE was a repeat of a previous study during that admission. Patients were observed for 30 days after TTE. While the main aim of this study was to give an overview of the lived experience of echocardiographic services during the first waves of the SARS-CoV-2 pandemic, the clinical outcome of all-cause mortality at 30 days post TTE in SARS-CoV-2 positive patients was used to demonstrate the features of our cohort. For patients with COVID-19 disease, the need for individual consent was waived by national UK guidance covering research during the COVID-19 pandemic as the data were collected by members of usual clinical care teams for the primary purposes of clinical need and/or locally approved service evaluation. The Gloucestershire Hospitals National Health Service Foundation Trust audit and governance committee gave permission to undertake this study.
Data collection
Anonymised demographic and clinical data were collected from the electronic patient record. Paper case notes were not able to be reviewed due to the requirement to enter a SARS-CoV-2 positive areas. Vascular biomarker and blood film results were collected from the initial admission with the exception of high sensitivity troponin. When a troponin was assessed on admission this has been included, otherwise the earliest troponin assessed for the patient has been collected alongside the peak value during admission. A positive diagnosis of SARS-CoV-2 was based on an upper-respiratory tract swab (both oropharynx and nasopharynx) with laboratory confirmed virus using reverse transcription PCR .16 Admissions to ITU, duration of admission and requirement for invasive/non-invasive ventilation were recorded.
Transthoracic echocardiography
In order to prepare for the local wave of SARS-CoV-2, TTE services at both centres were actively reconfigured to allow maximal inpatient capacity including daily weekday attendance in both ITUs. Additional weekend cover was also provided on an ad hoc basis. Capacity for this was created through repeat triaging of all outstanding outpatient TTE requests using a traffic light system to denote urgency. This was undertaken by a combination of British Society of Echocardiography (BSE) accredited sonographers and clinicians and resulted in the rescheduling of approximately 300 TTEs plus an additional approximately 300 other cardiac investigations (eg, ambulatory rhythm monitoring devices and transoesophageal echocardiograms).
Both institutions implemented a TTE COVID-19 scanning standard operating procedure (online supplemental appendix 1) in line with the BSE COVID-19 pathway.17 A level 1 BSE scan was performed on all patients with suspected or confirmed COVID-19 wearing national standards personal protective equipment to maximise protection and minimise contact time for the echocardiographer.18 To further reduce infection risk to sonographers, only fit tested sonographers undertook scans of confirmed or suspected SARS-CoV-2 and all required measurements were taken on returning to the cardiac investigations department. Dedicated GE Vivid q and S6 ultrasound machines (GE Healthcare, Horten, Norway) were allocated to perform all confirmed or suspected COVID-19 scans. All TTE studies were anonymously reviewed by a single BSE accredited echocardiographer. Quality was assessed according to published standards as set out by Nagata et al19
Supplemental material
Focused intensive care echocardiography scans were not included in this study as BSE level 1 protocol is not completely adhered too, meaning standardisation for the study could not be achieved.
Statistical analysis
Statistical analysis was performed using SPSS, V.22.0 (IBM). Categorical variables were reported as frequency and percentages. Comparison analyses for categorical data were performed using the χ2 or Fisher’s exact tests, dependent on appropriateness. Continuous data underwent histogram plots for assessment of normality. Normally distributed data were reported as mean and SD and comparative analysis performed using independent t-tests. Non-normally distributed data were reported as median (full range) and compared using Mann-Whitney U test. A posterior probability model, logistic regression was conducted for the covariates of age, gender and echocardiographic findings. Inclusion of further covariates was prohibited by the small sample size. A p<0.05 was considered statistically significant for all analysis. Mortality comparison was conducted including only patients which were SARS-CoV-2 positive within the study window.
Results
Patient characteristics and outcomes
Thirty SARS-CoV-2 suspected or confirmed positive patients were referred for an inpatient TTE, 27 of which proved to have been positive during the study window. Of the positive group, mean age was 62.6±11.9 years, 7 (25.9%) were female and 7 (25.9%) died within 30 days of their TTE. Table 1 provides full details of patient characteristics. Notably the group of those who died (mean 68.4±11.9 years) compared with those who survived (mean 60.5±13.0 years) were significantly older (p=0.03).
Demographics and baseline characteristics of all included patients
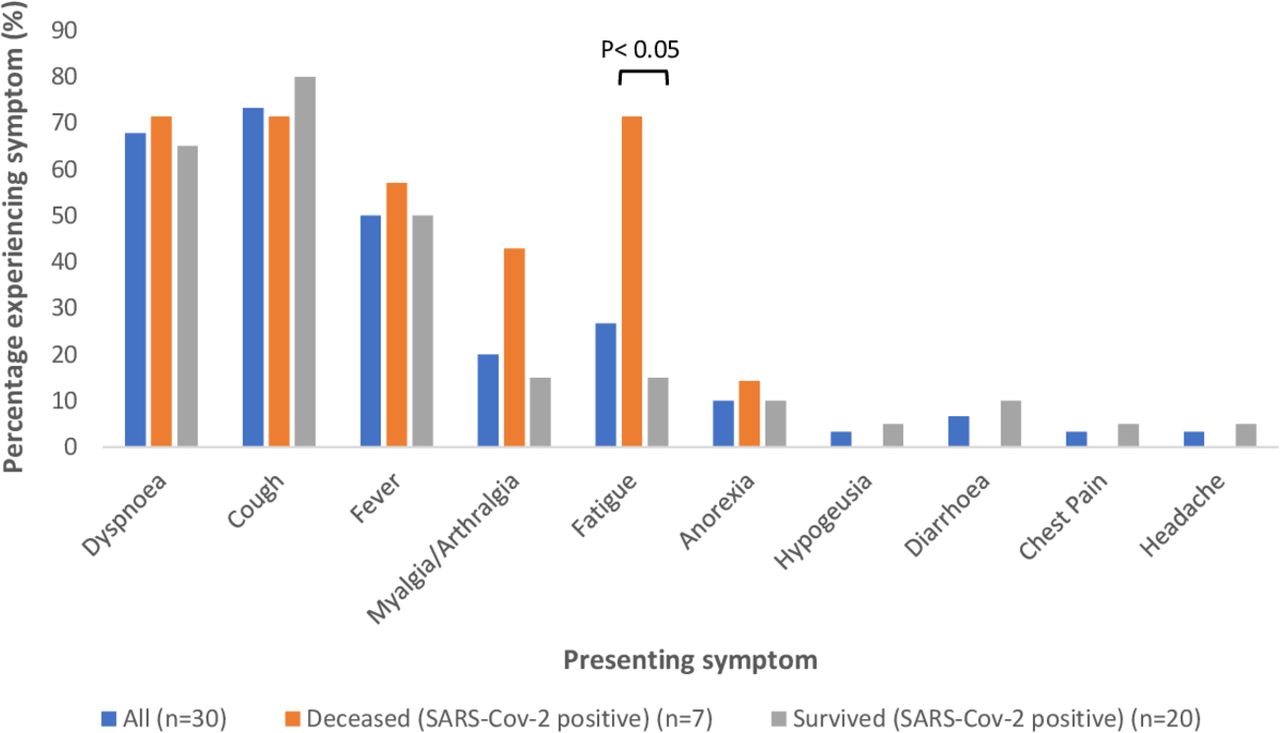
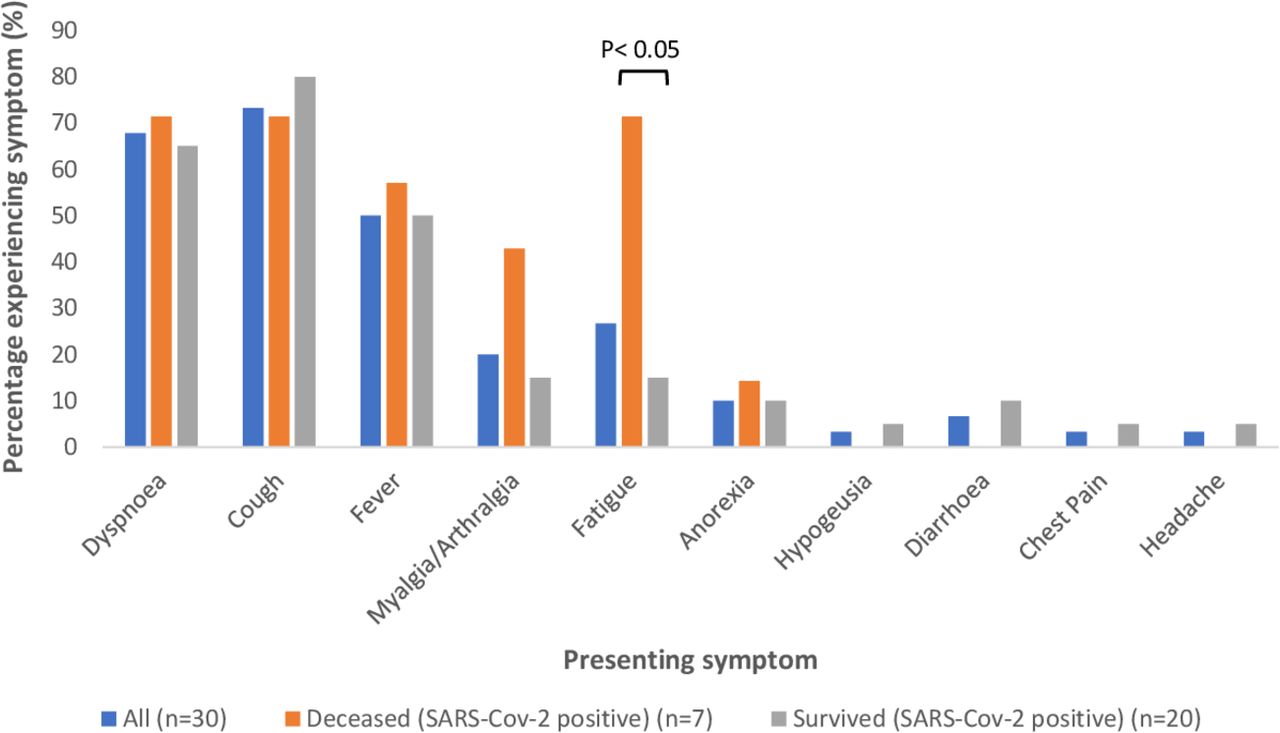
Among the SARS-CoV-2 positive patients, the most common presenting symptoms were cough (21 patients, 77.8%), dyspnoea (18 patients, 66.7%) and fever (15 patients, 51.9%). Figure 1 displays full details of presenting symptoms. No significant differences were identified in presenting symptoms during mortality comparison analysis with the exception of fatigue (p=0.01). The most common comorbidities were hypertension (11 patients, 40.7%), chronic respiratory disease (7 patients, 25.9%) and diabetes mellitus (6 patients, 22.2%), with no significant difference between those that survived and died at 30 days. Table 1 contains complete details of comorbidities.
{kind=link}
Frequency of presenting symptoms of patient cohort.
Of the 27 patients within the SARS-CoV-2 positive cohort 13 (48.1%) were inpatients at day 30, with six in ITU and seven in general medical wards. The final seven (25.9%) patients had been discharged home. With regard to treatment in the SARS-CoV-2 positive population, seven (25.9%) patients required continuous positive airway pressure during the data collection window, three (42.9%) of which died within the 30 days. Twenty (74.1%) patients required an ITU stay during the data collection window, 19 (70.4%) of which were intubated and ventilated. Mean ITU stay was 12.2 days (SD 9.70). There was no significant difference between treatment modalities or in the duration of ITU stay in mortality comparison analysis. Table 1 displays full details of treatments.
Biomarkers
Hs-cTnT was performed in 21 (77.9.6%) SARS-CoV-2 positive patients, of which four had a single measurement. Table 2 shows the full range of biomarkers in SARS-CoV-2 positive cases. Median initial and peak troponin values were 17.6 ng/L (2.5–3239 ng/L) and 48.0 ng/L (5.1–3239 ng/L), respectively. Eighty-one per cent of patients had a troponin above the 99th percentile of the upper reference limit. One significant outlier value of 3239.0 ng/L was recorded in a patient who presented with an ST-elevation myocardial infarction. No significant difference for either troponin value was identified in mortality comparison analysis.
Biomarkers of SARS-CoV-2 positive patients
Transthoracic echocardiogram
Thirty-one TTEs were performed during the data collection window, one of which was a repeat scan for a patient already included in the dataset and therefore was excluded from further analysis. Table 3 outlines the quality, location and indications for all TTEs. The most common indications were assessment for possible heart failure, largely in terms of left ventricular (LV) function (n=13, 43.3%), and right heart function and strain, often querying a pulmonary embolus (n=8, 26.7%). Eight patients had further imaging to investigate for a possible pulmonary embolism (largely CT pulmonary angiograms) of which two were positive (one at segmental and one at subsegmental level). Both of the positive cases had normal right ventricular size and function. The majority of the TTEs performed were of a good image quality (13 patients, 43.3%), with the remainder being fair (13 patients, 43.3%). Table 4 demonstrates the findings from the TTEs. Binomial logistic regression found no significant association between age, gender and echocardiographic result (see online supplemental appendix 2).
Supplemental material
Quality, location and. indications for all TTEs performed (n=30)
TTE findings for SARS-CoV-2 positive patients
Discussion
The SARS-CoV-2 global pandemic has seen rapid reconfiguration of services across the world to meet the predicted demand. Echocardiography was predicted to be, and has been, an essential service across healthcare to assess the potential cardiac manifestations of SARS-CoV-2.13–15 20 In the UK, the BSE outlined the expectation of higher demand and having to adapt normal routines to meet the demand.17 During the first wave of the pandemic in the UK, two centres in the South West of England performed 31 focused TTE on suspected or positive SARS-CoV-2 patients. This service was delivered through the successful rapid reconfiguration of TTE services to meet requirements. While it is always necessary to justify an investigation, never has this been truer than in the context of pandemic infectious disease. The experience described serves to highlight how close liaison with departments, for example, through daily visitation of ITU, can serve to prioritise patients with greatest need while minimising unnecessary exposure to sonographers. This is in-keeping with data presented by Ward et al which highlights an increase in the ‘appropriateness’ of TTE requests as a result of the pandemic.20
The role of echocardiography in the care of SARS-CoV-2 patients has varied across hospitals and countries during the pandemic. Drake et al, for example, describe its use in the following scenarios: assessment of patient with respiratory presentations which may or may not be secondary to SARS-CoV-2 infection; assessment for cardiac dysfunction in ITU patients with SARS-CoV-2; evaluation of volume status in patients with SARS-CoV-2.13 This not standard practice in the UK. Given the increased work load experienced by the hospitals during the pandemic, this would have been impractical to institute and would have significantly increased exposure to sonographers. The prime use of TTE in the paper presented better fits the latter two indications described above, as a large majority were performed in ITU with the primary indication of possible heart failure. A smaller number were requested exclusively for assessment of cardiac function in ITU patients; this it likely to near equate with assessment of volume status as described by Drake et al13
This paper adds to the limited data available regarding echocardiographic abnormalities identified in SARS-CoV-2 patients. The results presented mirror the few existing publications which have demonstrated rates of left ventricular systolic dysfunction of 5.4%–11%,21 22 in keeping with the 7.4% identified above. However, the LV dysfunction identified in our positive cohort were related to other mechanisms. There is no clear mechanism of CI from SARS-CoV-2 in these patients.
The most common abnormality seen in the existing literature is often right ventricular dysfunction or dilation as demonstrated here.21 23 The exception to this is the high rate of pericardial effusions >0.5 cm (19.6%) seen in one study during the Wuhan outbreak.22 The result of this study, therefore, adds to the existing evidence suggesting significant myocarditis is not a common feature of SARS-CoV-2 infection as had been previously feared.3 22 Whether the right ventricular systolic dysfunction can explain the raised troponins seen in many SARS-CoV-2 patients2 3 7 9–12 and the increased risk of mortality10 is debatable as correlations with raised troponins have been conflicting.21 23 Certainly, the lack of difference between the TTE findings in the above mortality analysis would not support this as a theory. Comparatively, another paper to conduct mortality analysis on TTE data identified only low left ventricular ejection fraction, raised E/e’ ratio, elevated right ventricular end diastolic area and higher Tei index as being associated with fatality.23 It is likely that the small sample size of the cohort presented explains the lack of association between echocardiographic findings and mortality which has been found by others.23
The pathophysiology of CI associated with SARS-CoV-2 is likely multifactorial. Potential mechanisms for right ventricular dysfunction include elevated pulmonary vascular resistance secondary to higher left atrial pressure, pulmonary vascular disease (including pulmonary emboli) and parenchymal lung disease.21 23 With regard to CI overall, many have cited indirect damage as a result of the exaggerated inflammatory response seen in SARS-CoV-224 25 as a causative pathway,26–30 mediated in part by the resultant prothrombotic state and vascular inflammation (and so plaque instability) generated.27 29 Evidence for this can be seen in the correlation between elevated cardiac biomarkers and ECG abnormalities with higher inflammatory markers.30
Direct viral infection of myocytes via ACE2 receptors has also been widely theorised to be responsible for SARS-CoV-2-related CI.26 28–31 Given severe acute respiratory syndrome also acts via AEC2 receptors32 33 and has been identified in cardiomyocytes on postmortem analysis34 35 this seems plausible. By comparison, while fatalities of the SARS-CoV-2 pandemic have shown cardiac pathological changes from mild interstitial inflammation to myocyte necrosis,29 there is no evidence as yet of SARS-CoV-2 identified within cardiac tissue of patients in postmortem studies. One study has, however, successfully demonstrated direct infection of human cardiomyocytes in vitro and additionally found this occurs in an ACE2 and cathepsin-dependent fashion.36
Finally, cardiac stress secondary to hypoxaemia and resultant oxygen supply and demand mismatch,30 31 37 stress-induced cardiomyopathy,29 31 viral induced vasculitis31 and iatrogenic causes secondary to drug side effects28 37 have all be debated as possible mechanisms for SARS-CoV-2-related CI.
Limitations
Our study has several limitations, which must be considered when interpreting the results. First, the number of patients included is small, most likely as the South West of England had relatively low rates of SARS-CoV-2 compared with other UK regions during the first wave38 As the aim of the study was to demonstrate the demand and service adaptions required during the increase in cases of SARS-CoV-2, data collection was only undertaken during this peak escalation window. The resultant small numbers are likely to explain the higher incidence of right ventricular abnormalities and higher peak troponin in the group surviving at day 30. The design of the study also prohibited the performing of echocardiograms on day one of admission in order to obtain a baseline image set, as was conducted in one published study.23 While this has obvious benefits, on average the patients included had experienced symptoms for 9 days at the point of admission. As a result, it is highly possible that even day one TTEs may already reflect damage resulting from SARS-CoV-2 infection.
A second limitation of the study was the absence of blinding of the echocardiographers to the patient infection status potentially introducing interpretation bias. A second blinded reviewer confirmed the findings generated to attempt to partially overcome this issue. Third, only BSE level 1 scans were performed as per the local and national standard operating procedure.17 No point of care ultrasound scans was included, potentially limiting our numbers of patients. However, standardisation would have been more difficult if these had been included. Finally, it is broadly recognised that the SARS-CoV-2 viral swabs have a sensitivity of approximately 70%39 and so, by using swab results to define the patient cohort for this study it is possible some cases may have been missed. Within the conducting trust, however, it was common practice to take multiple swabs from patients who had an initial negative result but had a clinical phenotype highly likely to represent SARS-CoV-2 infection. As such, it is hoped the impact of this inclusion criteria is small.
Conclusion
The study demonstrated a TTE service in a UK district general hospital can be adapted to meet the demands of a rapidly progressing international health crisis. Our echocardiographic data observed right heart dilation and strain most commonly on our small cohort, this is hypothesised to be related to raised pulmonary artery pressures. There was no association between SARS-CoV-2 patients’ echocardiographic findings and mortality, unlike other papers recently published.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @DrChrisMcAloon
Contributors The idea for this article was contributed by CJM who also oversaw the creation of the article. Data were collected by RLC, MG and HW. The paper was written and the statistics completed by RLC. All other authors contributed to the echocardiographic service and to the coordination of data collection.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The internal audit and governance committee gave permission to undertake this study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as online supplemental information. Discussion of the data used is welcome.