Article Text

Abstract
Objective The COVID-19 pandemic resulted in prioritisation of National Health Service (NHS) resources to cope with the surge in infected patients. However, there have been no studies in the UK looking at the effect of the COVID-19 work pattern on the provision of cardiology services. We aimed to assess the impact of the pandemic on cardiology services and clinical activity.
Methods We analysed key performance indicators in cardiology services in a single centre in the UK in the periods prior to and during lockdown to assess reduction or changes in service provision.
Results There has been a greater than 50% drop in the number of patients presenting to cardiology and those diagnosed with myocardial infarction. All areas of cardiology service provision sustained significant reductions, which included outpatient clinics, investigations, procedures and cardiology community services such as heart failure and cardiac rehabilitation.
Conclusions As ischaemic heart disease continues to be the leading cause of death nationally and globally, cardiology services need to prepare for a significant increase in workload in the recovery phase and develop new pathways to urgently help those adversely affected by the changes in service provision.
- coronary artery disease
- heart failure
- delivery of care
- cardiac rehabilitation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
The COVID-19 work pattern affected the way healthcare is delivered through restructuring and prioritisation of resources. It is therefore expected that the COVID-19 work pattern will have an impact on the delivery of medical and surgical services. Quantifying this effect is necessary in order to plan how to deal with COVID-19 sequelae in the recovery phase.
What does this study add?
As ischaemic heart disease continues to be the leading cause of death in the world, assessing the direct and indirect effect of COVID-19 on cardiology through COVID-19-related cardiac diseases and through the restriction of cardiology provision is necessary to plan our services in the post-COVID-19 era.
How might this impact on clinical practice?
The impact of COVID-19 will be felt beyond the direct effect of COVID-19-related cardiac diseases. The provision of cardiac services was severely restricted due to a shift in the focus in dealing with the surge of patients with COVID-19 and patients’ reluctance to seek medical help during the lockdown period. There was therefore a reduction across all cardiology performance indicators from referrals to investigations, diagnoses and management of cardiology patients. It is therefore expected that there will be another surge of patients seeking cardiology care and that services need to plan to treat these patients early and urgently to prevent any long-term complications.
Introduction
The emergence of the COVID-19 pandemic has changed the delivery of medical care across the world. In the UK, there are 280 000 confirmed cases with more than 40 000 COVID-19-related deaths.1 This unprecedented surge in COVID-19 infections led many governments around the world to implement population lifestyle changes through social distancing, shielding and lockdown measures to limit the spread of infection. In the UK, healthcare services had to be restructured to cope with the increased pressure and demand on the National Health Service (NHS).2
Hospitals themselves can be a potential source of infection. Indeed, hospitals in Lombardy in Italy became the new epicentre of infections.3 Therefore, the healthcare system had to be restructured to minimise patient contact with healthcare professionals, limit or reschedule hospital visits and outpatient clinics, postpone non-urgent procedures, and adopt telephone and video-assisted consultations.4 The UK government used an educational campaign to reduce the spread of infection and protect the NHS by advising people to ‘Stay Home; Save Lives; Protect the NHS’. In addition, patients with pre-existing cardiovascular diseases are prone to severe complications from COVID-19 infections.5 Therefore, more extreme lifestyle changes through shielding were implemented for those deemed to be most vulnerable, such as those with cardiac transplants, complex congenital heart disease and advanced heart failure in order to reduce their exposure risk.6
In line with government guidelines, cardiology services had to alter the delivery of care by adopting virtual clinic models, redeployment of staff to the acute medical services and rescheduling of non-urgent procedures, while at the same time dealing with the cardiac complications of COVID-19 such as myocarditis, myocardial infarction and heart failure.7 8
Across Europe the surge in COVID-19 infections is now declining, giving hope that we are in the recovery phase. However, the risk of a second wave is still present. Since ischaemic heart disease is the leading cause of death,9 it is necessary to assess the impact of the lockdown and healthcare restructuring on the performance of cardiology service provision and the changes needed to prepare for the recovery phase and a potential rebound surge of clinical activity.
Methods
We set out to assess key performance indicators of cardiology services in a district general hospital (Dumfries and Galloway Royal Infirmary, serving a population of 149 000) and supporting tertiary services (Golden Jubilee National Hospital, Glasgow) in the periods prior to and during the COVID-19 lockdown. We compared four time intervals, each 1 month long: 21 January to 20 February 2020 (baseline); 21 February to 20 March 2020 (transition period), when concerns and expectations about COVID-19 increased and service restructuring preparations were developed; 21 March to 20 April 2020, and 21 April to 20 May 2020 (lockdown periods). Changes including reductions in cardiology service provision and clinical activity during the lockdown intervals were compared with the first interval of baseline activity.
Patient and public involvement
There was patient and public involvement (PPI) during the development of the study design and interpretation. We consulted several service users in primary and secondary care settings through cardiac rehabilitation, heart failure, outpatient and inpatient cardiology services. They were all strongly supportive of the research. We will continue to involve patients and the public in implementing the outcomes of this study.
Results and discussion
Cardiology admissions and myocardial infarction
During the first month of lockdown there was a marked reduction in chest pain/breathlessness presentations with a 53% reduction in cardiology ward and coronary care unit (CCU) admissions. Similarly, there was a 40% drop in the number of patients diagnosed with myocardial infarction (table 1). Other markers were the significant fall in the number of acute cardiac tests performed, with a 46% reduction in cardiac troponin T (cTnT) blood tests and an 87% reduction in 12-lead electrocardiograms (ECGs). Moreover, there was a 44% reduction in inpatient ECGs, and 75% fewer N-terminal-pro B-type natriuretic peptide (NT-proBNP) blood tests performed both in primary and secondary care indicating a reduction in patients presenting with symptoms and signs of heart failure (table 2).
Patient reviews (inpatient and outpatient activity), procedures performed, and staff variations for different intervals: baseline activity (green), preparation period (amber), and during the COVID-19 lockdown (red). Percentage reduction refers to the change in data from the baseline period to the period of lockdown
Diagnostic activity (inpatient and outpatient): baseline activity (green), preparation period (amber), and during the COVID-19 lockdown (red). Percentage reduction refers to the change in data from the baseline period to the periods of lockdown
Even though these reductions improved during the second month of lockdown, they were still below the baseline level of activity, indicating an ongoing decrease in the overall number of patients presenting to cardiology services.
Cardiology outpatient service
In line with NHS guidance on implementing COVID-19 work patterns, we adopted telephone and ‘Attend Anywhere’ video consultation services to minimise exposure risks to patients and staff. We were able to set up secure remote working access and establish virtual clinics using technology enabled care services (TECS). New and return clinic appointments were triaged into virtual or face-to-face clinics depending on the need and urgency of the referrals. Overall, the number of patients referred from primary care to cardiology outpatient clinics dropped by 80%. As a result, face-to-face clinics dropped by 93% and there was a substantial increase in the use of the virtual clinics (figure 1).
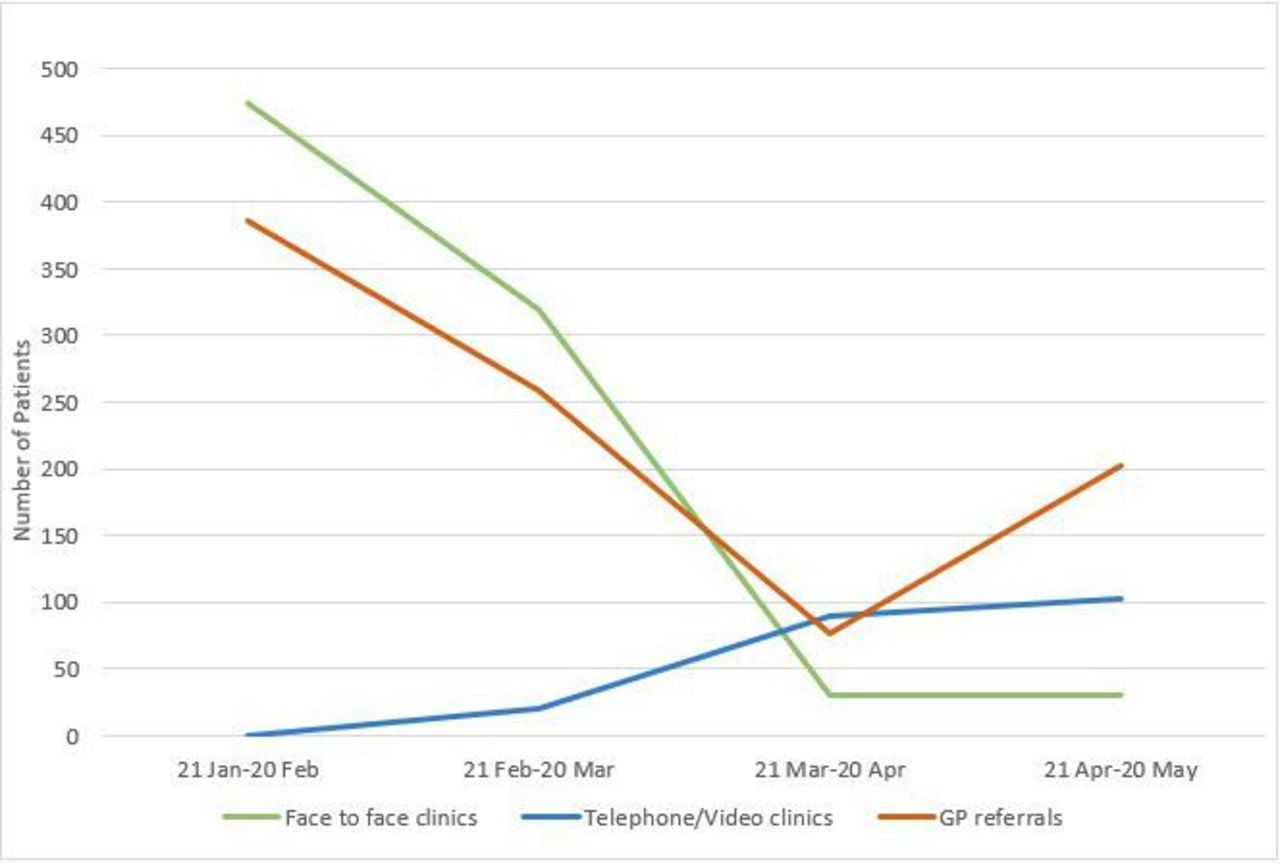
Outpatient clinics activity before and during lockdown. GP, general practitioner.
Moreover, the overriding importance of minimising potential patient exposure led to more thorough triaging of even that reduced number of primary care referrals, focusing on urgency, appropriate investigation instead of clinic assessment, and telephone consultation if necessary within 24 hours of receipt of the referral. In this way the majority of urgent referrals did not require face-to-face clinic assessment. While labour-intensive at this point of entry into secondary care, this has to be a template for future outpatient practice, which will yield dividends in reduced clinic waiting times once the ‘new normal’ becomes established.
Despite these changes to service delivery, the practice of referring and discussing patients in local and regional multidisciplinary team (MDT) meetings was maintained. However, the MDT meetings were performed via video conferencing to maintain social distancing and reduce the risk of virus transmission. The added benefit of this new method of delivering MDT meetings was the involvement of other team members from different base hospitals who were able to attend and discuss their patients remotely.
Cardiac investigations
With the exception of computed tomography coronary angiography (CTCA), all cardiac investigations were managed by the clinical physiology department. At the start of lockdown there was an increase in the number of patient cancellations to the clinical physiology department, and reduced face-to-face clinics. Many clinical physiology staff were redeployed to the CCU, the cardiology ward and acute medical wards to support existing nursing staff. For instance, the hospital telemetry system became supported by the cardiac physiologist, allowing critical care nurses to focus on looking after COVID-19 patients. Within the clinical physiology department social distancing was implemented in waiting areas and all staff wore droplet precaution personal protective equipment (PPE) with every patient. Requests for cardiac investigations during the lockdown intervals were triaged into urgent and routine, with routine investigations rescheduled. Therefore, the number of ECGs and outpatient echocardiograms dropped by more than half and the uptake of ambulatory cardiac monitors dropped by 73% (table 2).
There was a parallel reduction in functional assessments of myocardial ischaemia (exercise tolerance tests (ETTs) and dobutamine stress echocardiograms (DSEs)); all routine DSEs were postponed until after lockdown. Other investigations such as transoesophageal echocardiography (TOE) and CTCA were significantly reduced, by 63% for CTCA, and cancellation of routine TOEs in line with the British Society of Echocardiography COVID-19 guidance (figure 2).10

Cardiac investigations before and during lockdown. cTnT, cardiac troponin T; ECG, electrocardiography; Echo, echocardiogram; NT-proBNP, N-terminal-pro B-type natriuretic peptide; OP, outpatient.
Cardiac procedures and interventions
Cardiac device implantation and direct current cardioversion
Cardiology procedures were triaged into priority groups. We used the British Heart Rhythm Society (BHRS) guidance to classify cardiac device implantation into ‘Priority 1’, ‘Priority 2’ and ‘Postpone’ groups.11 During lockdown we only performed pacemaker implantations within the Priority 1 group (complete heart block or symptomatic second-degree heart block). Priority 2 procedures were defined as elective procedures that could only be done during the COVID-19 period if capacity allowed, considering the risks and benefits to the patient and staff involved. These included other symptomatic bradycardia patients such as those with sinoatrial node disease or pacemaker generator replacements. Some Priority 2 procedures were done during the last few weeks of the second interval of lockdown when COVID-19 new cases started to fall following consultation with patients and management. The remaining indications for pacemaker implantation were classified as ‘Postpone’ and will be booked after the COVID-19 crisis is over. Therefore local device procedures halved while implantation of internal loop recorders and direct current cardioversions were postponed (table 1). Similarly, the number of patients transferred from tertiary care following complex device (cardiac resynchronisation therapy (CRT)/implantablecardioverter defibrillator (ICD)) implantation and electrophysiology studies dropped significantly.
The pacemaker follow-up service was also reconfigured. Pacemaker patients were established on home monitoring systems and reviews were performed via telephone consultation. Only patients with arrhythmias or battery depletion were brought into the face-to-face pacing clinic for review.
Coronary angiography and cardiac surgery
The coronary angiography services were restructured with a focus on regional centralisation and reduction of inter-hospital patient transfer. The Golden Jubilee National Hospital (Glasgow) became the main regional centre for primary and urgent percutaneous coronary interventions (PCI) for patients presenting from Dumfries and Galloway and most of the West of Scotland.
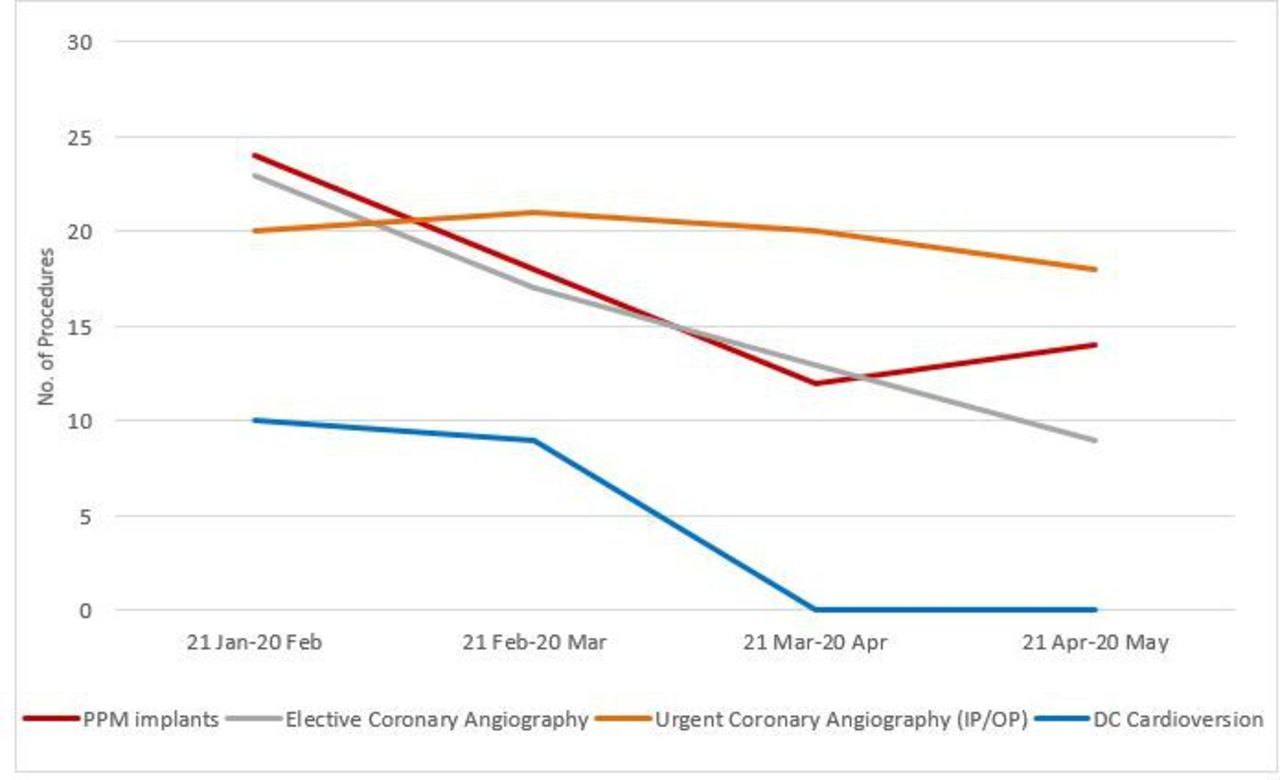
There was, however, a significant drop in the number of referrals for coronary angiography and cardiac surgery. This decrease was partly due to the reduction in patients presenting with chest pain and myocardial infarction but also due to the prioritisation of patients needing urgent coronary angiography. Therefore, despite a significant reduction in elective coronary angiography, there was no change in the number of urgent coronary angiography or primary PCI performed (figure 3). A possible explanation is that patients were presenting late to hospital with more severe ischaemia requiring urgent angiography, having resisted earlier appropriate admission because of fears of contracting the virus. Similarly, there was prioritisation of cardiac surgical procedures, including coronary artery bypass grafting, leading to a significant reduction in the number of cardiac surgeries performed from eight at the baseline period to only one procedure during the second period of the lockdown (figure 3).

{kind=link}
{kind=link}
{kind=link}
Cardiac procedures before and during lockdown. DC, direct current; IP, inpatient; OP, outpatient; PPM, permanent pacemaker.
Heart failure
The COVID-19 work pattern implemented restrictions on NHS services including the community heart failure service (HFS) with a cessation of face-to-face clinics and home visits. The heart failure specialist nurses were maintained within the HFS. They, however, had to participate in familiarisation training with the ward environments in anticipation of potential redeployment.
New patients referred to HFS dropped by 34% in keeping with the trends in heart failure symptom presentation and NT-proBNP measurements across primary and secondary care.
Home visits and face-to-face clinic appointments were put on hold and there was therefore an increased reliance on virtual clinics with a 66% increase in the telephone clinics and ‘Attend Anywhere’ video consultation services (table 1).
In order to optimise patients’ care during the lockdown intervals, strategies to educate and empower patients were adopted such as providing patients with blood pressure monitors and scales to facilitate the uptitration and optimisation of treatment, and forging even closer cooperation with primary care staff to monitor renal function.
Cardiac rehabilitation
Cardiac rehabilitation delivery changed from the usual face-to-face service to a virtual service via telephone call and NHS ‘Attend Anywhere’ video consultation. The last face-to-face assessments and supervised exercise sessions took place on 16 March 2020. The capacity of the service diminished substantially with redeployment of cardiology specialist and rehabilitation nurses to help with the reconfiguration of the cardiology ward to create a new four-bedded coronary care/high dependency unit, thereby freeing up capacity within the CCU. There was therefore a 45% reduction in the delivery of cardiac rehabilitation (table 1). There was a substantial growth in the exploration and adoption of healthcare technologies through the use of a digital heart manual, the use of the 'myHeart' app and online exercise programmes, and the issuing of blood pressure and heart rate monitoring machines to patients through the Integrated Community Equipment Services (ICES). These new tools have successfully been used during the COVID-19 lockdown intervals and will likely continue to be a permanent part of cardiac rehabilitation after the service is restored to full capacity.
Conclusions
To our knowledge, this is the first study in the UK to assess the impact of COVID-19 on the provision of cardiac services and clinical activity. Analysis of this UK single-centre experience showed that the COVID-19 pandemic has led to a significant reduction in all sections of cardiology services including referrals to outpatient clinics, investigations, cardiology admissions, number of patients diagnosed with myocardial infarction, cardiac procedures, interventions and community services such as heart failure and cardiac rehabilitation. The findings are consistent with the recently published results of the haematology team in Oxford University Hospitals indicating a significant drop in the blood tests performed, referrals to haematology services and diagnoses of haematological malignancies as a result of the COVID-19 lockdown measures.12 Therefore, it is likely that similar changes will be seen in other medical and surgical specialties and that assessment, preparation and restructuring of these services for the recovery phase should be based on these findings.
The reasons for these reductions are multifactorial and include the restructuring and prioritisation of NHS services, reduced access to primary care, and patients’ reluctance to seek medical help due to fear of contracting the virus. At the height of the pandemic, it is acceptable to deviate from the standard level of care and agreed guidelines in order to prioritise the delivery of essential services. However, adverse consequences for some patients presenting with worsening of their underlying cardiac conditions have been inevitable. Consequently, cardiology services should be ready to offer them urgent input and early intervention.
The second interval of lockdown showed a gradual increase in patients referred to cardiology services and a rise in the investigation and diagnosis of myocardial infarction compared with the first interval of lockdown. There is therefore an expectation of a rebound surge of increased workload on cardiology services, which need to restructure in preparation for this scenario.
The COVID-19 work pattern established technology at the heart of the delivery of care where virtual clinics using telephone and video consultation will be a long-lasting legacy and MDTs and meetings using video conferencing will be the norm.13 The use of these communication technologies was positively received by healthcare workers and patients. However, it also highlighted the need to develop a communication infrastructure to ensure that these services can be delivered to all parts of the community regardless of geographic or economic background.
The COVID-19 pandemic has also highlighted the versatility of the NHS and the readiness of its staff to adapt quickly and face new challenges. The pandemic has ignited the need to develop new pathways of care models and protocols and has prompted a new era of medical–nursing collaboration and resilience. The experience gained from the current outbreak will be vital in dealing with any future challenges.
Acknowledgments
The authors would like to acknowledge Kim Heathcote and Adam Khengui for the collection of biochemical data; Shafiq Ahmed, Kirstin Nelson, Melanie Branney, Fiona McManus, Jill Craig, Lorri Kirkaldie, Cynthia Hart, Pam Houston, Linda Houston, Issy Bate and Louise Plummer for cardiology admissions data; Fiona Ross, Mieke McKend, Jill Pagan and Hayley Birrell for clinical physiology service data; Hazel Hughes, Mairi Smail, Angela Allan and Maggie Morrison for heart failure and cardiac rehabilitation data; Paul Wilson, Stacy Huntly and Jayne Durham for computed tomography coronary angiography and pacing data; Ken Donaldson, Heather Currie and Carol Morton for manuscript review; and Alex McGuire and Martin Dawes for coronary angiography and cardiac surgery data (Golden Jubilee National Hospital, Glasgow).
Supplementary materials
Press release
Footnotes
Contributors The study was conceived and designed by OF, SB, RN, KM, CB and AM. Data collection was carried out by RN, CB, BD, VG and VW. Data analysis was carried out by OF, SB and AJ. The initial manuscript was compiled by OF, SB, RN, KM and CB. AM contributed substantially to critical revision of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval NHS Dumfries and Galloway Clinical Audit Approval Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. No additional data are available.