Article Text

Statistics from Altmetric.com
Learning objectives
To become familiar with the contemporary epidemiology of heart valve disease, including endocarditis;
To recognise the relationship between heart valve disease epidemiology, the ageing population and current treatment options;
To be aware of the probable future trends in heart valve disease epidemiology.
Introduction
In this review, we will discuss the current knowledge of heart valve disease (HVD) epidemiology, how it has changed over time and possible future trends. There are large differences in HVD epidemiology between high-income and low-income countries and across different forms of HVD. The majority of morbidity and mortality attributable to HVD worldwide is due to rheumatic heart disease (RHD), which is most commonly seen in low-income countries. In high-income countries, the greatest burden of HVD referred to hospital is due to calcific aortic valve disease (CAVD). Although prevalence of HVD is low compared with coronary heart disease, the requirement for long-term follow-up, and significant investigation and treatment costs, means that the impact of HVD on healthcare systems is disproportionately large. The strong association between HVD and age, combined with the rapid ageing of populations worldwide, means that HVD has been described as the ‘next cardiac epidemic’.1
Rheumatic heart disease
Current knowledge
Acute rheumatic fever (ARF) occurs a number of weeks after Streptococcus pyogenes (group A streptococcus) infection, usually in children. ARF leads to valve inflammation through molecular mimicry between the streptococcal M protein and cardiac proteins such as myosin and vimentin, although it is likely that other mechanisms are also involved.2 The requirements for ARF to lead to chronic RHD are not yet fully established but are likely to be related to repeated episodes of often subclinical secondary infection, leading to progressive valve fibrosis and self-sustaining valve inflammation. Those with repeated infections are more likely to progress to chronic RHD, and extended antibiotic prophylaxis is recommended for those with a single episode of ARF (table 1).3
Summary of recommendations for secondary prophylaxis of acute rheumatic fever
The burden of RHD falls disproportionately on low-income countries and in low-income groups in high-income countries. Incidence of ARF has been difficult to establish globally, with estimates ranging from 10 cases per 100 000 to as high as 374 cases per 100 000 in Pacific and indigenous Australian and New Zealand communities.4 Indigenous Australians aged 5–14 years (the peak age group to develop ARF) have an incidence of 194 per 100 000.5 Similarly, in New Zealand the overall population age-standardised incidence of 17.2 per 100 000 for ARF requiring hospitalisation masks an almost 20-fold increased rate for Māori (40 per 100 000) and a 40-fold increased rate in Pacific people (81 per 100 000) compared with New Zealanders of non-Māori/Pacific origin (2.1 per 100 000).6
Systematic screening for chronic RHD using echocardiography in school-age children leads to a 10-fold higher estimation of RHD prevalence compared with clinical screening.7 A review of recent studies predominantly using echocardiography for diagnosis of chronic RHD shows wide global variations in prevalence, between 46 per 100 000 in northern India and 2400 per 100 000 in the Solomon Islands.8 The natural history of RHD has been examined in Indigenous Australians showing that 35% with a first episode of ARF developed RHD by 1 year, 51% by 5 years and 61% by 10 years.5 The only statistically significant risk factor for progression to RHD was the age at diagnosis of the first ARF episode, and this was only of marginal impact (Cox proportional HR 0.98 per year older, 95% CI 0.96 to 0.99). Peak prevalence was seen in the 45-year to 64-year age group, at 3100 per 100 000. Of those with RHD, 21% progressed to heart failure within 2 years and 27% progressed within 5 years.5
The Global Burden of Disease (GBD) study has estimated mortality from RHD and many other diseases both globally and in each country and region. The GBD derives estimates from vital registration, surveillance, verbal autopsy and other sources of data, with modelling methods used to address any deficiencies in the available data.9 The mortality rate due to RHD was 4.4 per 100 000 population in 2013, accounting for 275 100 deaths worldwide that year. Even in high-income countries, RHD mortality accounts for a large proportion of valve disease-related deaths, being third behind aortic valve disease and endocarditis in the USA in 2009 (figure 1).10
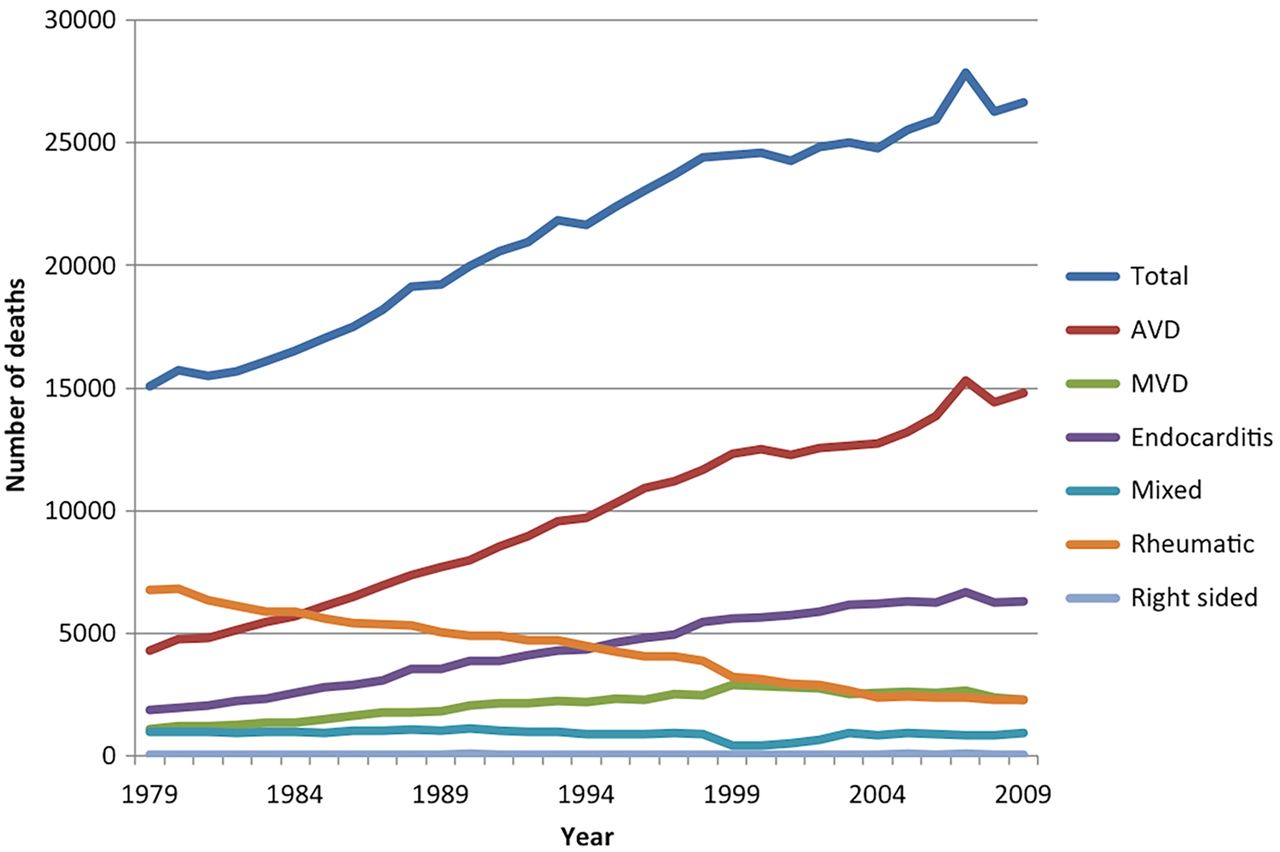
Number of deaths per year due to heart valve disease in the USA, by cause. Reproduced from Coffey et al10 under license from Elsevier.AVD, aortic valve disease.
Trends over time
The incidence of ARF showed a dramatic decline in high-income countries from the start of the 20th century, possibly related to improved access to healthcare, or to changes in the form of streptococcal infection.11 ,12 More recently, the GBD study reported a 26% decline from 1990 to 2013 in numbers dying due to RHD worldwide and a 55% reduction in age-standardised mortality.9 These figures hide the ongoing disparities between different populations globally (figure 2). The declining incidence of ARF in high-income countries over many decades has resulted in RHD becoming relatively uncommon, with a continuing decline in RHD-associated mortality (figure 1).10 ,12 High-risk groups in high-income countries have not seen the same declines, with increasing ARF incidence from 1993 to 2009 in New Zealand Māori and Pacific people (79% and 73% increase, respectively) despite a decrease in incidence in the non-Māori/Pacific population.6 Likewise, the incidence of first episode of ARF in Indigenous Australians did not change significantly from 1997 to 2010.5 In addition, the high costs of valve interventions (accounting for 72% of the cost associated with RHD in a New Zealand-based study) are likely to be beyond the resources of many low-income countries.13

Change in age-standardised mortality rate due to rheumatic heart disease from 1990 to 2010. Data were obtained from the Global Burden of Disease study.15 The colour of the circles indicates the mortality rate category, while the area of the circle indicates number of deaths. Mortality rate can be seen to have decreased in most countries, accompanied by a reduction in numbers dying. The country with the highest numbers of deaths from rheumatic heart disease was China in 1990 and was India in 2010. An interactive data visualisation is available at: http://oxvalve.nhs.uk/research/rhdmap
Nonetheless, there have been positive results. Although it is difficult to compare between studies, evidence suggests increasing incidence of ARF over time only in the Western Pacific, with other regions having stable or decreasing incidence.14 Only four countries—Georgia, Zimbabwe, Swaziland and Burkina Faso—had an increase in RHD-associated mortality from 1990 to 2010 (figure 2).15 On the global scale, China's age-standardised RHD-associated mortality dropped to 4 deaths per 100 000, a 73% decrease since 1990, leading to a reduction in deaths from 131 394 in 1990 to 57 105 in 2010, accounting for a large proportion of the worldwide reduction in mortality over this period. In Australia, although the introduction of the Northern Territory RHD Control Program has not been associated with reduction in first incidence of ARF, it has been associated with a reduction in recurrences of ARF, which should reduce progression to RHD.5
The disease burden of RHD may continue to decrease with ongoing implementation of World Heart Federation (WHF) recommendations on diagnosis and management of RHD.16 ,17 The WHF have identified five key targets, focused on endemic areas, likely to provide the greatest benefit in its goal of reducing RHD deaths in those aged under 25 years by 2025. These are establishment of RHD control programmes, ensuring the availability of benzathine penicillin G, recruitment of a public figure to champion RHD causes, establishment of at least one major RHD hub in each geographic region, and a phase III clinical trial of a vaccine against group A streptococcus. Although not a key target, the lack of access to essential cardiac medication and to effective anticoagulation monitoring was also identified by the WHF as a barrier to reduction of RHD mortality.17 This was highlighted recently by a registry of patients from Yemen, India and 12 African countries showing only 69% of those with an indication for anticoagulation were receiving it, and of these, only 28% had an international normalised ratio within the therapeutic range.18 Control of incidence and recurrence, the main outcomes expected to be improved by implementation of the WHF recommendations, should contribute to a reduction in morbidity and mortality, initially in the under-25s and, with time, throughout the population.
Although ARF has almost disappeared in high-income countries, it is important to remain aware of RHD, which remains prevalent in migrant people. This concerns in particular young women, given the high risk of pregnancy-related complications in mitral stenosis.
Calcific aortic valve disease
Current knowledge
CAVD is a spectrum of disease, ranging from aortic sclerosis (ASc) without haemodynamic effect to severe aortic stenosis requiring valve replacement.19 ASc does not have a known direct impact on the myocardium, but is important at the population level due to its high prevalence and its association with higher risk for adverse events.20 Approximately 40% of those over the age of 75 have ASc, and this finding is associated with an increased risk of myocardial infarction, stroke and death, even after traditional cardiovascular risk factors are accounted for. The cause of this excess risk remains to be fully explained, but ASc is frequently associated with coronary atherosclerosis21 and shares elements of its pathophysiology.22
Over time, ASc progresses slowly to haemodynamically significant AS, with just under 2% of those with ASc progressing to AS per year.23 ,24 AS is, therefore, relatively uncommon in those aged under 65 years in the absence of a congenital abnormality. A meta-analysis of predominantly older studies conducted in Europe, the USA and Taiwan found a population prevalence of AS of 12.4%, and a prevalence of 3.4% of severe AS in those aged 75 years and older.25 More recent studies have shown relatively similar figures, with 4.3% in an Icelandic cohort aged ≥70 having severe AS.26 The Tromsø study showed an exponential increase in prevalence with age, with 0.2% in the 50–59-year group, 1.3% in the 60–69-year group, 3.9% in of the 70–79-year group and 9.8% of those aged 80–89 years having any AS (figure 3).27 In this study, the incidence of new AS was 5 per 1000 per year, with the initial mean age of participants being 60 years. Information from low-income countries about the burden of CAVD is very limited. AS is uncommonly the predominant valve lesion in RHD (only accounting for 9% of new cases in a large South African cohort).28

Prevalence of aortic stenosis according to age group in the Tromsø study. The percentage having surgery increases with age, but not to the same extent as prevalence. Reproduced from Eveborn et al27 under license from BMJ Publishing Group Ltd.
In younger age groups, clinically significant AS is due predominantly to bicuspid aortic valve (BAV) disease with tricuspid aortic valve stenosis requiring aortic valve replacement (AVR) only becoming more common over the age of 70 years.29 BAV is the most common form of congenital heart disease, being found in approximately 0.5–0.8% of the population.30–33 BAV leads to a requirement for treatment at a younger age than with tricuspid aortic valves, with a mean age at surgery of just under 50 years.34
Although moderate or severe mitral regurgitation (MR) is more prevalent than aortic stenosis in the community, AS is more important when judged by clinical impact.35 The EuroHeart study surveyed patients in secondary and tertiary care facilities, and in this setting AS is the most frequent form of HVD, accounting for 34% of the total HVD population, and even more common in those who have undergone valve intervention, accounting for 47% of this group.36 Much of the mortality due to HVD is due to AS in high-income countries. AS accounts for 45% of all deaths with HVD as the underlying cause of death in the USA and has driven most of the increase in the total number of HVD deaths seen over the past three decades (figure 1).10
No medical therapy currently exists that has been proven to affect the natural history of the disease,37–39 with clinical management relying on accurate assessment to determine whether an indication for valve replacement exists.40 The well-documented reluctance to offer older patients AVR, and the patients themselves to accept the intervention, despite a poor prognosis once an indication for AVR exists,41 ,42 may have reduced since the advent of transcatheter AVR, with its proven efficacy in higher or excessive surgical risk patients.43–45
Trends over time
Projections in high-income countries uniformly predict an increase in the burden of disease. Numbers of elderly patients with an indication for treatment (severe symptomatic AS aged 75 years and older), which is the most important group for healthcare systems due to the complexity and cost of management, are projected to more than double by 2050 in both the USA and Europe.25 Similarly, in Iceland, projections suggest a doubling in prevalence of those with severe AS aged ≥70 years by 2040 and a tripling by 2060.26
Once RHD prevalence begins to decrease, CAVD can be expected to play a relatively more important role as a cause of AS in low-income countries. In addition, the mean life expectancy in many low-income countries is currently below the age at which AS due to CAVD becomes clinically significant (eg, the average life expectancy at birth in Africa was 58 years in 2012).46 The high prevalence of risk factors for CAVD such as hypertension and increasing life expectancy mean that there is likely to be a substantial future burden of CAVD in low-income countries.
Endocarditis
Current knowledge
Endocarditis is less common than RHD or CAVD, with an incidence of between 1 and 11 per 100 000 people per year.47 However, the high associated mortality (>20%, predominantly during the first hospital admission), morbidity in the form of embolic phenomena such as stroke (16%, with most occurring within the first week) and requirement for valve surgery mean that endocarditis remains an important form of HVD.47 Limited data worldwide have been improved recently by the addition in 2010 of endocarditis to the list of diseases examined by the GBD study. This showed an age-standardised mortality rate of 1.0 per 100 000 in 2013, accounting for 65 000 deaths worldwide.9
Trends over time
The high case-fatality rate seen with endocarditis has traditionally led to recommendations for prophylactic antibiotic use in groups at higher risk, namely those with a prosthetic valve or prosthetic valve repair material, those who have previously had endocarditis and those with congenital heart disease leading to cyanosis or with prosthetic material that has not endothelialised. Over the past 15 years, this has changed, with current European recommendations limiting this recommendation only to high-risk groups undergoing high-risk procedures, particularly dental procedures involving perforation of the oral mucosa, or manipulation of the gingival or periapical region.48 In France, similar recommendations had been made in 2002, and subsequent population-based studies showed that the incidence of endocarditis did not change significantly from 1991 to 2008.49 By contrast, in the UK, the National Institute for Health and Care Excellence guidance recommended against prophylactic antibiotics in any situation.50 Despite a sceptical reception from cardiologists and cardiac surgeons in the UK, 51 ,52 the rate of prescriptions for prophylactic antibiotics dropped precipitously, and in 2013 was less than one-eighth of the rate prior to publication of the guidance in March 2008.53 The incidence of endocarditis in the UK had been slowly increasing, and the change in national guidance has been associated with an increase in this trend, although a causal relationship has not been proven.53
GBD 2013 data suggest a 12.7% reduction in age-standardised endocarditis mortality worldwide since 1990.9 Even so, there was a 46.3% increase in the total number of deaths. The discrepancy between these figures (even after accounting for an estimated 35% increase in the global population) may be explained by endocarditis deaths being predominantly concentrated in older age groups, where the effect on the overall mortality rate is reduced by age-standardisation to a younger population. Population-based studies suggest that the age of patients with endocarditis has increased, and (as might be expected) older age is associated with an increased mortality rate.49 In the USA, age and sex-adjusted mortality rates increased by an average of 2% per year from 1979 to 2009 in the USA, to the point that endocarditis is now, after aortic valve disease, the second leading contributor to total HVD deaths.10
The major causes of endocarditis have changed with time. Hospital-based studies suggest an increase in endocarditis due to Staphylococcus aureus and coagulase-negative staphylococcus in North America, associated with an increase in intravenous drug use-associated endocarditis.54 Different population-based studies in Europe and Australia now report Staphylococcus as the leading cause of infective endocarditis.49 ,55 ,56 It is also likely that healthcare-associated infective endocarditis contributes to staphylococcal predominance. Healthcare-associated endocarditis represents 25–30% of cases of infective endocarditis and is associated with a higher risk profile.
Cardiac implantable electronic device (CIED) infections are another major cause of endocarditis in high-income countries, with 23–37% of those with CIED infections having heart valve involvement.57 ,58 The increasing implant rate seen over the past few decades has led to a consequent increase in CIED infection in the USA.59 In addition, the increasing tendency to implant devices in patients with more comorbidities, and to implant more complex devices, has been associated with an increased rate of CIED infection since the mid-2000s.59 Other high-income countries such as the UK are also seeing a continuing increase in CIED implantation,53 and it is likely therefore that CIED-associated endocarditis incidence will continue to rise.
In the future, the ageing of the population is likely to continue to drive the increase in endocarditis-related mortality. The threat of multidrug-resistant organisms may well impact on medical management of endocarditis, possibly leading to an increasing requirement for cardiac surgery.60 There are, however, prospects that new information on, for example, early cardiac surgery on vegetations with a high embolic risk, may improve the case-fatality rate.61 In addition, the development of leadless CIEDs may reduce the rate of CIED infections in the future.62
Other valve diseases
Mitral regurgitation
Other valve diseases are more difficult to accurately describe due to a wider number of causes. Although CAVD is the most important form of HVD with regard to mortality, the most prevalent form of moderate or severe valve disease in developed countries is MR.35 In the Framingham Offspring study, MR was seen in 88% of men and 92% of women, but most of this was trivial—mild or more severe MR was seen in 19% of participants.63 Similarly, in an African-American cohort aged 50 years and older, 14% had mild MR and 0.7% had moderate or more severe MR.64
MR can be either primary (due to a problem with the valve or subvalvular apparatus themselves) or secondary (also called functional, where the valve and subvalvular apparatus appear normal but a separate LV abnormality prevents coaptation of the leaflets). The most common causes of primary MR in industrialised countries are mitral valve prolapse, RHD and endocarditis.36 Mitral valve prolapse has a prevalence of 2.4% in the population, although the degree of associated MR is most commonly trivial or mild.65 Unlike calcific aortic disease, no clinical risk factors have been clearly identified for mitral valve prolapse.
Secondary MR is a frequent finding in the setting of cardiomyopathy – 49% had mild to moderate secondary MR and 24% had severe secondary MR in one series of 1256 patients.66 No population-based study allows for a reliable estimation of the prevalence of secondary MR. However, extrapolations derived from available data suggest a high burden in the community.67 Due to the associations between MR and age,63 and between secondary MR and heart failure, there is likely to be an increase in prevalence of MR over the coming decades.
Aortic regurgitation
Aortic regurgitation (AR) can be due to a primary cause such as BAV or secondary to aortic root dilatation. AR of mild or greater severity was seen in 13% of men and 8.5% of women in the Framingham Offspring study,63 while moderate or more severe AR was estimated to be prevalent in approximately 0.5% of the total US population.35 In an African-American cohort, 9% had mild AR and 0.5% had moderate or more severe AR.64 Again, all of these prevalences increase with increasing age.
Tricuspid regurgitation
Similarly to MR, tricuspid regurgitation (TR) is most frequently a secondary phenomenon. In the Framingham Offspring study, TR of mild or greater severity was seen in 15% of men and 18% of women,63 while in an African–American cohort, 15% had mild TR and 1.8% had moderate or more severe TR.64 As expected, the presence of TR was associated with increasing age in these studies. After accounting for ventricular function or by excluding those with abnormal LV function, severe TR is associated with increased mortality (figure 4).68 ,69 CIED leads cause TR through a variety of mechanisms (figure 5). Approximately 25–29% of patients with permanent pacemakers have TR, roughly double the prevalence in comparison groups.70 In a population predominantly comprising patients with implantable cardioverter-defibrillators, 38% of patients had a significant increase in severity of TR after CIED implantation, and this was independently associated with increased mortality.71

Survival in patients with tricuspid regurgitation on clinically indicated echocardiography. Severe tricuspid regurgitation (TR) was associated with reduced survival even after adjustment for age, LV and RV systolic function, and RV size. Reproduced from Nath et al68 under license from Elsevier.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Causes of tricuspid regurgitation due to cardiac implantable electronic device leads. (A) Direct interference with leaflet coaptation. (B) Fibrous adhesions between leaflet and lead. (C) Interference with subvalvular apparatus. (D) Leaflet perforation. (E) Annular dilatation due to chronic ventricular dyssynchrony related to RV pacing. Reproduced from Al-Bawardy et al70 under license from Wiley Periodicals.
While its clinical importance has gained more recognition recently,72 it is likely that the impact of secondary TR has been underestimated in vital statistics as deaths will have been coded according to the primary disease. Again, the ageing of the population and the projected rise in number of patients with heart failure, as well as the continued increase in CIED implantation, are likely to lead to an increase in the prevalence of TR.73
Congenital heart disease
With the improved survival of patients with congenital heart disease due to improved paediatric cardiac surgical techniques,74 it is likely that there will be an increase in the numbers of adults with HVD of congenital origin, who often have concomitant complex congenital heart problems.
Prosthetic valve disease
Prosthetic valve disease is an increasingly common reason for valve replacement or repair. Prosthetic valves may be sites for thrombus formation (particularly mechanical valves, for which anthithrombotic therapy is indicated), or pannus outgrowth, which can obstruct the normal functioning of the prosthesis.75 Physical failure is relatively rare in mechanical prostheses, but bioprostheses may undergo structural valve deterioration, resulting in stenosis, regurgitation or leaflet fracture. Valve failure can lead to a requirement for repeat valve replacement or, in those with bioprotheses, valve-in-valve insertion.76 Long-term data on transcatheter valves are limited due to both their recent introduction and the shorter life expectancy of current recipients. More common in transcatheter aortic valves is a finding of paravalvular AR, with recent studies finding that moderate to severe AR was common in the 30 days after implantation (approximately 15% of patients), was largely paravalvular, and was a strong predictor of subsequent mortality.77–79 Given the relatively short follow-up available, clinicians should remain vigilant for novel complications related to ageing transcatheter valves.
Autoimmune connective tissue diseases
Autoimmune connective tissue diseases can lead to secondary HVD (such as ankylosing spondylitis-associated aortitis leading to AR), but also through direct mechanisms, likely related to valve inflammation. Libman–Sacks endocarditis has long been recognised as a phenomenon in systemic lupus erythematosus (SLE).80 A recent meta-analysis of 1656 patients found that overall 31% had at least one valve lesion, and the risk was three times higher in SLE patients with antiphospholipid antibodies compared with those without.81 ,82 Patients with primary antiphospholipid syndrome (ie, without an associated disease such as SLE) have valve lesions detectable using transthoracic echocardiography in approximately one-third of cases, and even higher proportions detectable using transoesophageal echocardiography.83
More recently, it has been recognised that the other autoimmune connective tissue diseases also carry a significantly increased risk of HVD. For example, rheumatoid arthritis is associated with a greater than fivefold increased risk of TR and AS and more than threefold increased risk of MR.84 A low threshold for investigation of potential HVD should be maintained in these patients.
Emerging HVD
Radiation and drug-induced valve disease (DIVD) are relatively recent phenomena.85 ,86 Both may raise diagnostic problems with other restrictive valve diseases, particularly RHD, highlighting the importance of interpreting echocardiographic findings according to the clinical context. The response to associations with DIVD has varied according to country—fenfluramine and benfluorex, appetite-suppressing drugs closely linked with DIVD, were withdrawn from sale after the association with HVD was recognised,87–89 while the ergot-derived dopamine agonist pergolide was withdrawn from sale in the USA but remains available in other markets, albeit with new warnings.90 The European Medicines Agency recommends an echocardiogram at baseline and regularly during treatment for patients prescribed pergolide or another DIVD-associated dopamine agonist, cabergoline.90 Low-dose cabergoline, used for the treatment of prolactinomas, has not been definitively associated with DIVD.86 DIVD appears histologically identical to carcinoid valve disease and so it is not surprising that serotonin, via the serotonin 2B receptor, is the culprit mechanism.91 Fortunately given the very large number of prescriptions worldwide, selective serotonin reuptake inhibitors do not appear to cause DIVD.92 ,93 As with autoimmune connective tissue diseases, a high index of suspicion for HVD is required in patients who have had exposure to drugs linked with DIVD.
Conclusions
Of the different forms of HVD, RHD appears to be slowly coming under control, even in some high-risk populations. As RHD mortality and morbidity has decreased, it has been overtaken by ‘degenerative’ causes of HVD, particularly CAVD. The burden of mortality and morbidity associated with these age-related diseases can be expected to increase worldwide due to increasing life expectancy.
Key messages
Rheumatic heart disease primarily affects those in low-income countries and high-risk groups in high-income countries, and led to an estimated 275 100 deaths worldwide in 2013.
The incidence of acute rheumatic fever in high-risk groups in high-income countries has either remained unchanged or increased in the past two decades, while data from low-income countries are limited.
Rheumatic heart disease mortality is decreasing in both high-income and low-income countries worldwide.
In high-income countries, aortic stenosis is the largest contributor to deaths due to heart valve disease.
In those with tricuspid aortic valves, although progression of aortic stenosis is an active process, calcific aortic valve disease presents primarily as a disease of old age.
Mitral regurgitation is a particularly heterogeneous group, comprising diverse aetiologies of organic mitral regurgitation and the possibility of regurgitation through a structurally normal valve, secondary to LV remodelling.
The ageing of the population, especially in high-income countries, is predicted to lead to a significant increase in the burden of aortic stenosis and endocarditis over the coming decades.
You can get CPD/CME credits for Education in Heart
Education in Heart articles are accredited by both the UK Royal College of Physicians (London) and the European Board for Accreditation in Cardiology—you need to answer the accompanying multiple choice questions (MCQs). To access the questions, click on BMJ Learning: Take this module on BMJ Learning from the content box at the top right and bottom left of the online article. For more information please go to: http://heart.bmj.com/misc/education.dtl
RCP credits: Log your activity in your CPD diary online (http://www.rcplondon.ac.uk/members/CPDdiary/index.asp)—pass mark is 80%.
EBAC credits: Print out and retain the BMJ Learning certificate once you have completed the MCQs—pass mark is 60%. EBAC/ EACCME Credits can now be converted to AMA PRA Category 1 CME Credits and are recognised by all National Accreditation Authorities in Europe (http://www.ebac-cme.org/newsite/?hit=men02).
Please note: The MCQs are hosted on BMJ Learning—the best available learning website for medical professionals from the BMJ Group. If prompted, subscribers must sign into Heart with their journal's username and password. All users must also complete a one-time registration on BMJ Learning and subsequently log in (with a BMJ Learning username and password) on every visit.
References
Footnotes
Twitter Follow Sean Coffey at @drseancoffey and Benjamin Cairns at @bj_cairns
Contributors The manuscript outline was designed by SC and BJC. SC performed the initial literature search and wrote the first draft. BJC and BI revised the manuscript critically. All authors reviewed and approved the final version.
Funding SC is supported by the National Institute of Health Research (NIHR) Oxford Biomedical Research Centre Programme. BJC acknowledges support from the British Heart Foundation Centre of Research Excellence, Oxford (British Heart Foundation grant no. RE/13/1/30181).
Disclaimer The views expressed in this publication are those of the authors and not necessarily those of the Department of Health.
Competing interests BI has received consultant fees from Abbott, Boehringer Ingelheim, Valtech, and speaker's fees from Edwards Lifesciences.
Provenance and peer review Commissioned; externally peer reviewed.