Article Text

Abstract
Aim To determine the incidence, type and possible association with mortality of major bleeding in patients with non-ST segment elevation acute coronary syndrome (NSTE-ACS) treated with an invasive strategy using predominantly the radial approach and triple antiplatelet therapy.
Methods In the multicentre randomised ABOARD Study, 352 patients with NSTE-ACS were randomised to an ‘immediate percutaneous coronary intervention (PCI)’ strategy or a strategy of PCI on the ‘next working day’. Radial access was predominantly used in this study population. The present subanalysis evaluated the occurrence of major bleeding complications and their association with mortality at 1 month.
Results Patients were treated with a triple antiplatelet therapy using high loading and maintenance doses of clopidogrel and abciximab in 99% of patients receiving PCI. The trans-radial approach was used in the vast majority of patients (84%). During the first 30 days, major bleeding complications (STEEPLE definition) occurred in 5.4% of patients (n=19), with no difference between immediate and delayed intervention. The most common bleeding complications were occult bleeding (36.8% of bleeding, n=7/19) and overt gastrointestinal bleeding (21% of bleeding, n=4/19). Patients with major bleeding had a higher peak concentration of creatinine during hospitalisation (mean±SD, 170±169 vs 97±57 μmol/l; p=0.005) and a 1-month mortality of 26.3%, much higher than patients without bleeding (0.6%, p<0.0001). Major bleeding was strongly associated with 30-day mortality (OR 50.3; 95% CI 10.1 to 249.7; p<0.0001).
Conclusion Despite the predominant use of the radial approach, major bleeding (essentially occult and gastrointestinal) remains a common complication, which is highly associated with mortality in patients with NSTE-ACS treated with optimal antithrombotic therapy.
- Bleeding
- radial
- acute coronary syndrome
- coronary angiography
Statistics from Altmetric.com
In acute coronary syndrome (ACS) treated by percutaneous coronary intervention (PCI), aggressive antithrombotic regimens have significantly enhanced the prognosis of patients through a reduction of ischaemic events.1–3 However, these treatments have been constantly associated with an increased risk of bleeding complications.
A body of evidence suggests that major bleeding complications are linked to recurrent ischaemic complications and mortality.4 Therefore, minimising bleeding complications in the setting of ACS has become a critical issue.
The potential benefits of trans-radial access have been reported to be prevention of bleeding complications and other adverse events,5 and it is now the preferred approach in several countries for reducing puncture-related bleeding complications. Nevertheless, in these PCI centres that specialise in the trans-radial approach, data are lacking on the rate and types of bleeding complications and their effect on patients' prognosis.
The ABOARD (angioplasty to blunt the rise of troponin in acute coronary syndromes randomised for an immediate or delayed intervention) Study was a multicentre randomised study that enrolled 352 patients with moderate-to-high-risk non-ST segment elevation ACS (NSTE-ACS) to undergo immediate or delayed PCI. In this study, which is unique in its predominant use of radial access in patients also treated with triple antiplatelet therapy, we analysed the incidence and type of acute major bleeding complications and their potential effect on 1-month survival.
Methods
Study population and randomisation
The ABOARD Study has been published.6 Briefly, 352 patients with NSTE-ACS were randomised to a ‘primary PCI’ strategy or a strategy of intervention deferred to the ‘next working day’. The mean delays between randomisation and PCI were 70 min in the ‘primary PCI’ strategy and 21 h in the ‘next working day’ strategy. NSTE-ACS was defined by the presence of at least two of the following criteria: symptoms of myocardial ischaemia; electrocardiographic ST-segment abnormalities (depression or transient elevation of at least 0.1 mV) or T-wave inversion in at least two contiguous leads; or an elevated cardiac troponin I concentration (above the upper limit of normal). Only patients with a thrombolysis in myocardial infarction (TIMI) score of 3 or greater and an indication for catheterisation were eligible for randomisation.
Medical therapy
Patients received aspirin at an initial high loading dose of up to 500 mg, followed by low-dose aspirin at 75 mg once daily. A high clopidogrel loading dose of more than 300 mg was also recommended followed by 75–150 mg once a day. Abciximab was administered in patients undergoing PCI (0.25 μg/kg intravenous bolus immediately followed by 0.125 μg/kg per min for 12 h). The choice of anticoagulant was left to the discretion of the investigators.
End points
The primary safety end point was the rate of major bleeding complications according to the STEEPLE definition7 during the first 30 days. Major bleeding included spontaneous, PCI-related bleeding and bleeding related to coronary artery bypass graft (CABG) and was defined as follows: bleeding that resulted in death; retroperitoneal bleeding confirmed by ultrasound or MRI, CT, surgery or autopsy; documented intracranial bleeding or intraocular bleeding; bleeding resulting in haemodynamic compromise requiring specific treatment; bleeding requiring surgical intervention or decompression of a closed space to stop or control the event; any transfusion of at least one unit of packed red blood cells or whole blood; overt bleeding resulting in a decrease in haemoglobin of ≥3 g/dl or, when haemoglobin concentration was not available, resulting in a decrease in haematocrit of ≥10%.
Patients were followed-up for 1 month. Mortality was defined as all-cause mortality.
The secondary end point was a composite of death from any cause, myocardial infarction, urgent revascularisation or recurrent ischaemia. Myocardial infarction was defined as any recurrent myocardial necrosis occurring either spontaneously or in the setting of revascularisation. Recurrent necrosis was defined by the occurrence of any of the following: new Q waves in two or more contiguous electrocardiographic leads; spontaneous or post-PCI elevation of creatine kinase activity and its MB isoenzyme to at least twice the upper limit of normal, with an increase of 50% or more over the previous value (if only creatine kinase values were available, the same rule applied, but a simultaneous increase in troponin I concentration was required).
Statistical analysis
Categorical variables are expressed as frequencies and percentages, and continuous variables are given as mean±SD. Comparisons between groups of patients according to the occurrence or absence of 30 days major bleeding were performed by t test for continuous variables and χ2 or Fisher exact test for categorical variables. Considering the very small number of events, Firth's8 approach to calculating OR was used to describe the death rate in patients with major bleeding versus patients without major bleeding. Kaplan–Meier survival curves were used to describe mortality during the 30 days of follow-up according to the presence or absence of acute major bleeding and were compared by the log-rank test. The statistical analyses were performed with SAS software, V.9.2.
Results
Baseline characteristics
Baseline characteristics, treatment received and procedural data for the 352 patients included in this study are shown in table 1. Aspirin was used in 99.7% of the population. Patients received high loading doses and maintenance doses of clopidogrel (660±268 mg and 111±40 mg, respectively); abciximab was administered for PCI, as specified in the protocol, and 99% of patients undergoing PCI were finally receiving abciximab. Low molecular weight heparin was used predominantly (68.1%), and the trans-radial approach was the most common arterial access (84%). Patients received optimal medical therapy as demonstrated by the high percentage of statins (94.6%), β blockers (86.1%) and ACE inhibitors/or angiotensin II receptor antagonist (82%).
Demographics and baseline patient characteristics of the study population and patients with and without major bleeding
Incidence and type of major bleeding complications
The flow chart of the study is presented in figure 1. During the first 30 days, major bleeding complications occurred in 5.4% of patients (n=19) with a 4.5% transfusion rate (n=16). Neither safety end point differed between the immediate and delayed intervention strategy. Non-CABG-related bleeding accounted for 68% of bleeding (n=13). Sites of major bleeding are presented in figure 2. The most common acute bleeding complications were occult bleeding (decrease in haemoglobin or anaemia requiring transfusion during hospitalisation, n=7), followed by gastrointestinal tract bleeding (n=4) and vascular access site (puncture-related) bleeding (n=4), which were all related to groin haematomas that occurred in the 16% of patients for whom the femoral approach was used. Other bleeding complications were haemopericardium (n=2), epistaxis (n=1), intracranial (n=1) and a non-access site haematoma (n=1). One of the patients had two bleeding events.

Study flow chart.
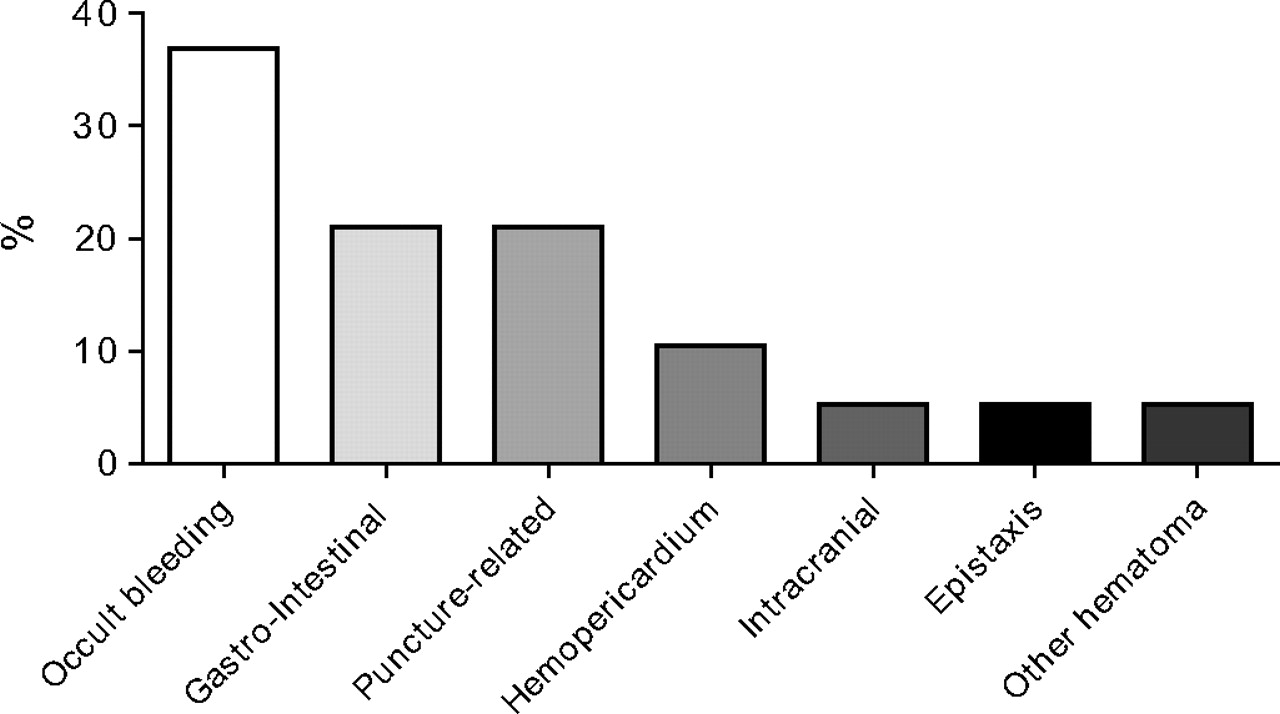
Sites of major bleeding during the first 30 days.
Outcomes
At 30 days, 11.9% (42/352) of patients had had a recurrent myocardial infarction, death or urgent revascularisation. Details of ischaemic and bleeding events are presented in table 2. The 30-day mortality was 2% (7/352). As shown in figure 3, major bleeding was associated with a higher mortality than in patients without bleeding (26.3% vs 0.6% (OR 50.3; 95% CI 10.1 to 249.7; p<0.0001)).
Treatments and bleeding and ischaemic events

{kind=link}
{kind=link}
{kind=link}
Cumulative Kaplan–Meier estimates of mortality during the first month according to the occurrence of major bleeding.
Characteristics of patients with major bleeding
Patients with major bleeding had a significantly higher baseline creatinine concentration than those without a major bleed (123±150 vs 83±31 μmol/l; p=0.05). They also had a significantly higher peak concentration of creatinine during hospitalisation (170±169 vs 97±57 μmol/l; p=0.005). Major bleeding complications were also associated with a longer hospital stay than in patients without major bleeding (13.6±9.3 vs 4.4±6 days, p<0.0001). The trans-radial approach had more commonly been used (85.5%) in patients without major bleeding than in those with major bleeding (68.4%) (p=0.05). No significant difference was found in the antithrombotic therapy between the two groups, except simultaneous use of both low molecular weight heparin and unfractionated heparin therapy was more common in patients with bleeding complications (47.4%) than in those without (25.7%) (p=0.05).
Discussion
In the present analysis, we present the rate and type of major bleeding complications, as well as their association with 30-day mortality, in a population of intermediate-to-high-risk ACS patients, treated with aggressive antiplatelet therapy and trans-radial percutaneous revascularisation. The multicentre randomised study, ABOARD, represents a unique opportunity to evaluate the impact of routine radial PCI on patients' outcomes, especially on bleeding complications in NSTE-ACS treated with triple antiplatelet therapy. To our knowledge, this is the first randomised study in patients with ACS using the radial approach in such a predominant manner. This study reflects a nationwide preference for radial access in PCI, not only for elective PCI but also in the setting of emergency and/or acute cases.
The first important finding of our study is that, despite the significant reduction in access site bleeding with the use of radial access in 84% of the patients, the rate of major bleeding complications at 30 days remains significant when sensitive definitions of bleeding, such as the STEEPLE definitions, are used. The second important finding is that the most common bleeding complication is occult bleeding, corresponding to a fall of 3 g/dl in haemoglobin, often leading to transfusion of red blood cells, and in patients with overt bleeding the most commonly identified location is gastrointestinal. More importantly, we report here that, although the nature of major bleeding complications has changed with trans-radial catheterisation, they are still associated with a longer hospital stay and a significantly increased risk of death during the first 30 days. All these findings were independent of the timing of catheterisation in this randomised trial.
Major bleeding complications have emerged as a strong determinant of ischaemic events and mortality in studies evaluating patients with ACS treated exclusively with the femoral approach.9 10 It is established that, in the absence of a universal definition, the rates of major bleeding vary considerably between studies.1 7 11–14 In the present work, we report a 5.4% rate of major bleeding using the STEEPLE definitions,7 which were definitions created for PCI and which are more sensitive than other classic ACS bleeding definitions.
Major bleeding complications are influenced by high antithrombotic regimens, but they also seem to be highly influenced by the access site used for PCI. In the contemporary ABOARD trial, a strategy of triple antiplatelet treatment, with high loading and maintenance doses of clopidogrel and the systematic use of abciximab at the time of PCI, was simultaneously used with a trans-radial approach. The aim of such a strategy is to optimise the pharmacological benefits on the ischaemic side, and to draw the safety benefits from a systematic radial artery access. This practice is supported by the results of recent studies in which intense platelet inhibition was associated with improved clinical outcomes, although the risk of non-CABG-related major bleeding was increased in such studies.1 2 15 In these trials, rates with the trans-radial approach were very low, always below 10%. However, even with rates as low as 8.2% in the TRITON Study, major bleeding was lower in the radial subgroup.16 These data and our analysis, all obtained in randomised studies, are supported by the results of several recently published studies17–20 and a meta-analysis published by Jolly and colleagues.5 In the present analysis, access site haematomas, which have been the most common bleeding complications of PCI for years, only occurred in the minority of patients treated with a femoral approach. We believe that this residual rate of the femoral approach corresponds to the real life management of patients with ACS in radial centres (eg, unstable patients, patients with prior CABG, radial access failure).
The results of the present study show that major bleeding still occurs, despite the predominant use of radial access, but it demonstrates that the localisation of the complication is shifting from femoral or retroperitoneal bleeding when femoral access is predominant to occult and gastrointestinal bleeding when radial access is the default strategy. However, the impact of these new types of bleeding should not be underestimated. A recent analysis21 clearly shows that gastrointestinal bleeding is a serious complication independently associated with mortality and ischaemic complications. Furthermore, gastrointestinal bleeding is probably underestimated, if we consider that major bleeding related only to a decrease in haemoglobin concentration may often be due to non-exteriorised gastrointestinal bleeding. The high rate of occult bleeding observed in our study is consistent with the rate of occult bleeding in the recent COGENT trial,22 in which it represented 33% of gastrointestinal events. Along the same lines, in the present analysis, major bleeding is still associated with a significant increase in mortality.
The results of this new analysis of ABOARD highlight the need to consider other strategies to reduce bleeding complications in addition to the use of radial access. In our study, the use of a mixed heparin regimen by switching from low molecular weight to unfractionated heparin was associated with an increased risk of bleeding complication. Although this finding may be confounded by other factors, it supports previous reports,23 24 and therefore such a strategy should be avoided. With regard to other types of antithrombotic therapy, the use of fondaparinux25 or bivalirudin11 26 has been shown to reduce bleeding complications in studies with predominant femoral access; however, their benefits remain to be demonstrated when trans-radial is the predominant approach. Attention should also be paid to the recent ESC guidelines,27 which have several suggestions including systematic assessment of bleeding risk using a dedicated score, stopping anticoagulation after revascularisation unless a specific indication exists, and selective downstream use of Glycoprotein IIb-IIIa inhibitors. A limitation to our study is related to the number of events, which was insufficient to allow a multivariate analysis and thus did not permit us to test whether or not the relationship between major bleeding and mortality was independent of the other clinical characteristics. However, the relation of bleeding to mortality still appears significant in this radial PCI study. We report major bleeding complications using the STEEPLE definition, a sensitive definition of bleeding created for PCI, which may appear to be a limitation and may have overestimated bleeding complications in comparison with more restrictive definitions such as TIMI or GUSTO (Global Use of Strategies to Open Occluded Coronary Arteries). Finally the ABOARD Study follow-up was restricted to the first 30 days, which may be another limitation to our study. However, in the Horizon Study,11 the reduction in bleeding-related mortality associated with the use of bivalirudin was mainly observed in the first month.
In conclusion, the trans-radial approach to catheterisation in NSTE-ACS is a technique that decreases access site complications, but major bleeding can still occur and appears to have the same deleterious effect on the patient's prognosis as bleeding related to the femoral approach. These bleeding events are often occult, leading to the use of transfusion, and/or have a gastrointestinal origin. Therefore the identification of patients at risk of gastrointestinal bleeding, and thus strategies to prevent it, is important.
References
Footnotes
Competing interests J-PC has received research grants (to the institution) from Bristol-Myers Squibb, Sanofi-Aventis, Eli Lilly, Guerbet Medical, Medtronic, Boston Scientific, Cordis, Stago, Fondation de France, INSERM, Fédération Française de Cardiologie and Société Française de Cardiologie, and has served as a consultant (honoraria for past 2 years) for consulting fees from Sanofi-Aventis, Eli Lilly and Bristol-Myers Squibb and lecture fees from Bristol-Myers Squibb, Sanofi-Aventis and Eli Lilly. JS has received research grants from Sanofi-Aventis, Daiichi-Sankyo, Eli Lilly, INSERM, Fédération Française de Cardiologie and Société Française de Cardiologie, consultant fees from Daiichi-Sankyo and Eli Lilly, and lecture fees from AstraZeneca, Daiichi-Sankyo and Eli Lilly. GC has received research grants from Fédération Française de Cardiologie, consulting fees from Eli Lilly, Daiichi Sankyo, CLS Behring and Abbott Vascular, and lecture fees from Eli Lilly, Daiichy Sankyo, Servier, Abbott, CLS Behring and AstraZeneca. SO'C has received research grants from A Menarini and the European Society of Cardiology. FB has received speaker honoraria from Pfizer, Astellas, Sanofi-Aventis and Roche. GM has received research grants from Bristol-Myers Squibb, Sanofi-Aventis, Eli Lilly, Guerbet Medical, Medtronic, Boston Scientific, Cordis, Stago, Centocor, Fondation de France, INSERM, Fédération Française de Cardiologie, Société Française de Cardiologie, ITC Edison, and Pfizer, consulting fees from Sanofi-Aventis, Eli Lilly, Bristol-Myers Squibb, The Medicines Company, Schering-Plough, Portola, Novartis, Menarini, Eisai, Daiichi Sankyo, Bayer and Boehringer Ingelheim, and lecture fees from Sanofi-Aventis, Eli Lilly, Bristol-Myers Squibb, Merck Sharpe & Dohme, Cordis, GlaxoSmith-Kline, Schering-Plough, Accumetrics, AstraZeneca, Daiichi Sankyo and Menarini.
Ethics approval The protocol was approved by the Comité de Protection des Personnes Ile-de France IV.
Provenance and peer review Not commissioned; externally peer reviewed.