Article Text

Abstract
Objective Current guidelines recommend that most patients aged ≥65 years should undergo mitral valve replacement (MVR) using a biological prosthesis. The objectives of this study were to assess whether these guidelines are being followed in UK practice, and to investigate whether the guidelines are appropriate based on in-hospital mortality and mid-term survival.
Methods Data from the National Institute for Cardiovascular Outcomes Research Adult Cardiac Surgery Audit database from all National Health Service (NHS) hospitals and some private hospitals performing adult cardiac surgery in the UK between April 2001 and March 2011 were analysed. The overall cohort included 3862 patients aged ≥65 years who underwent first-time MVR. Propensity score matching and regression adjustment were used to compare outcomes between prosthesis groups.
Results The mean age was 73.0 years (SD 4.9) with 50% of patients having surgery with a mechanical prosthesis. This proportion decreased over the study period and with increasing patient age with marked variation between hospitals. In the propensity-matched cohort, in-hospital mortality in the biological group was 6.9%, and in the mechanical group it was 5.9% giving an unadjusted OR of 1.17 (95% CI 0.84 to 1.63). There was no significant difference in mid-term survival between the matched groups with an unadjusted HR for biological prosthesis of 1.08 (95% CI 0.93 to 1.24). Similar results were found when using regression adjustment on unmatched data.
Conclusions Current guidelines concerning age and mitral valve prosthesis choice are not being followed for patients aged ≥65 years. With regards to in-hospital and mid-term mortality, this study demonstrates that there is no difference between prosthesis types.
Statistics from Altmetric.com
Introduction
Mitral valve replacement (MVR) is performed in patients with symptomatic mitral valve disease in whom mitral valve repair is not possible. MVR can be performed using either a biological or mechanical prosthesis. Bioprostheses avoid the need for lifelong anticoagulation unless it is otherwise indicated, but carry the risk of structural valve deterioration leading to valve failure and the need for redo surgery. Mechanical prostheses rarely require redo surgery for valve failure, but do require lifelong anticoagulation.
The American College of Cardiology/American Heart Association (ACC/AHA) guidelines state that MVR with a bioprosthesis is reasonable in patients 65 years of age or older (Class IIa, level C evidence).1 The European Society of Cardiology (ESC) guidelines recommend an age cut-off of <65 years for a mechanical valve and >70 for a biological valve (class IIa, evidence level C), but stress that an arbitrary age limit should not be set, and that each patient should be considered individually weighing up the risks of structural valve deterioration and anticoagulant-related bleeding in addition to informed patient preference.2
The ESC guidelines also recommend that life expectancy should be assessed, and if this is thought to be greater than the durability of the available biological valve then a mechanical valve should be used. For patients who would be considered low risk for redo surgery, MVR with a bioprosthesis should be considered (class IIa, evidence level C). These guidelines on prosthesis choice are largely based on expert consensus due to a lack of high-quality evidence available. A previous analysis of UK data has demonstrated that the majority of patients undergoing MVR had a mechanical prosthesis inserted but that the percentage of bioprostheses inserted was increasing over time.3
Given the lack of evidence around these guidelines and the observed changes in prosthesis choice over time, the first objective of this study was to study whether the guidelines relating to age and prosthesis choice are being followed in UK practice. The second objective was to investigate whether there is any evidence that the current guidelines are appropriate based on in-hospital mortality and mid-term survival.
Materials and methods
Data collection and preprocessing
Prospectively collected Society for Cardiothoracic Surgery in Great Britain and Ireland (SCTS) data were extracted from the National Institute for Cardiovascular Outcomes Research (NICOR) National Adult Cardiac Surgery Audit (NACSA) database.4 The data extract included all cardiac surgery procedures performed in National Health Service (NHS) hospitals in England and Wales between 1 April 2001 and 31 March 2011. An algorithm was developed to clean the data by removing any duplicate records, correcting transcriptional discrepancies, and resolving clinical and temporal conflicts. At this stage and prior to any analysis, a subsample of data (1 April 2008–31 March 2011) was returned to each contributing hospital for local validation.
Following data cleaning and validation, all isolated MVRs with or without coronary artery surgery or tricuspid valve repair in patients aged 65 years and over were included for analysis. Patients with ischaemic mitral valve pathology were excluded from the analysis. Patients who have previously had major cardiac surgery or those undergoing any other concomitant cardiac surgical procedure were excluded. All variable definitions used for the study are available at: (http://www.ucl.ac.uk/nicor/audits/Adultcardiacsurgery/datasets).
Outcomes
The primary outcomes of the study were (1) in-hospital mortality during admission to the base hospital for cardiac surgery and (2) mid-term survival. Operative and midterm mortalities were defined as death due to any cause. Patients were followed postoperatively to discharge by the NACSA database, and postdischarge by linking the recorded NHS numbers to the database of the Office for National Statistics (ONS), which records all deaths in the UK. The last date of ONS tracking in the dataset was 18 August 2011. Where possible, the remaining missing and conflicting in-hospital mortality data were resolved by back-filling using the linked ONS data.
Missing data
Records with missing discharge status were excluded from the analysis. Missing data for the patient characteristics and operative variables were imputed using a chain equation method that generates ‘plausible’ synthetic values for each missing risk factor using predictive mean matching and logistic regression modelling. The percentage of missing data for all variables except Body Mass Index (BMI) (5.2%), angina (6.7%) and active infective endocarditis (8.8%) was <5%. In total, 74.4% of records had no missing data. Therefore, a single imputation approach was preferred over a multiple imputation approach. Variables included in the imputation routine were those listed in table 1 (except BMI2), financial year, hospital, country and discharge status.5 Height and weight were included, with their relationship to BMI preserved by passive imputation.6 All imputations were implemented using the Multiple Imputation using Chain Equations (MICE) package for R (V.2.13).6
Patient characteristics and operative variables before and after propensity score matching
Data analysis
Bar charts were used to capture the trends in prosthesis implantation rates over time and in discrete age groups. Scatterplots are used to show the relationship between hospital volume and biological prosthesis implantation rate.
Statistical analysis
There is no definitive methodology for comparing treatments in observational studies with each approach having limitations. In the interests of drawing robust inferences, we applied two common approaches: (1) propensity score matching and (2) regression adjustment. All analyses were performed in R (V.2.15.2) (http://www.R-project.org).7 In all cases, a p value <0.05 was considered statistically significant.
Propensity score matching
A non-parsimonious propensity score model was developed in order to account for the inherent confounding between the prosthesis groups.8 The propensity score was developed using multiple logistic regression with prosthesis type as the outcome, and independent variables as listed in table 1.9 A nearest-neighbour matching method using the greedy matching algorithm with a calliper equal to 10% of the SD of log-odds transformed propensity scores was applied in order to match each mechanical prosthesis record to a single biological prosthesis record. The standardised difference for each patient characteristic was calculated before and after matching with an absolute standardised difference of <10% consistent with a reasonably balanced cohort.10 Inspection of propensity score histograms before and after matching was also performed prior to accepting the final matched cohort. Propensity score matching was performed using the MatchIt package for R (V.2.4-20).11
For the all-cause in-hospital mortality analysis, the unadjusted binomial proportions were calculated in the matched cohort. The OR and 95% CI was calculated with a χ2 test used to test whether the OR was statistically significantly different from 1. For mid-term outcomes in the matched cohort, Kaplan–Meier survival curves for freedom from all-cause mortality were calculated by prosthesis type. A HR and 95% CI were calculated, and a Mantel–Cox log-rank test applied to test for equality of the survival functions.
Regression adjustment
A multiple logistic regression model was fitted to the unmatched (ie, complete) data for in-hospital mortality including all preselected patient characteristics and operative variables significantly associated with in-hospital mortality at p<0.15 on univariate analysis. Prosthesis type was forced into the model a priori. BMI was categorised into underweight (BMI<18.5), healthy (18.5≤BMI<25), overweight (25≤BMI<30) and obese (BMI≥30). Age was dichotomised as >75 or ≤75 years old. Any variables that did not yield clinically sensible inferences, and which were statistically non-significant, were removed from the model and the ORs re-estimated. The adjusted ORs for the final model are reported. For the survival analysis, a Cox proportional hazards regression model was fit to the unmatched data following the same model development strategy as per the in-hospital mortality analysis. The proportional hazards assumption was assessed using the Grambsch–Therneau test based on the scaled Schoenfeld residuals.12
Results
Patient characteristics
From the inclusion criteria, there were 4846 records. Of these, 209 had ischaemic pathology and were excluded. A further 773 records were excluded as they corresponded to redo cardiac surgery. Finally, two records were excluded because of missing discharge status. Following application of the exclusion criteria, there were 3862 patients included from 33 hospitals. Isolated MVR was performed in 2224 (57.6%) patients with 1330 (34.4%) patients undergoing concomitant coronary artery bypass graft (CABG) and 395 (10.2%) patients undergoing concomitant tricuspid valve repair. Marginally more patients had MVR using a biological prosthesis (50.4%). The mean age at procedure was 73.0 years (SD 4.9), and the majority of patients were women (58.1%). A summary of the patient risk factors is given in table 1.
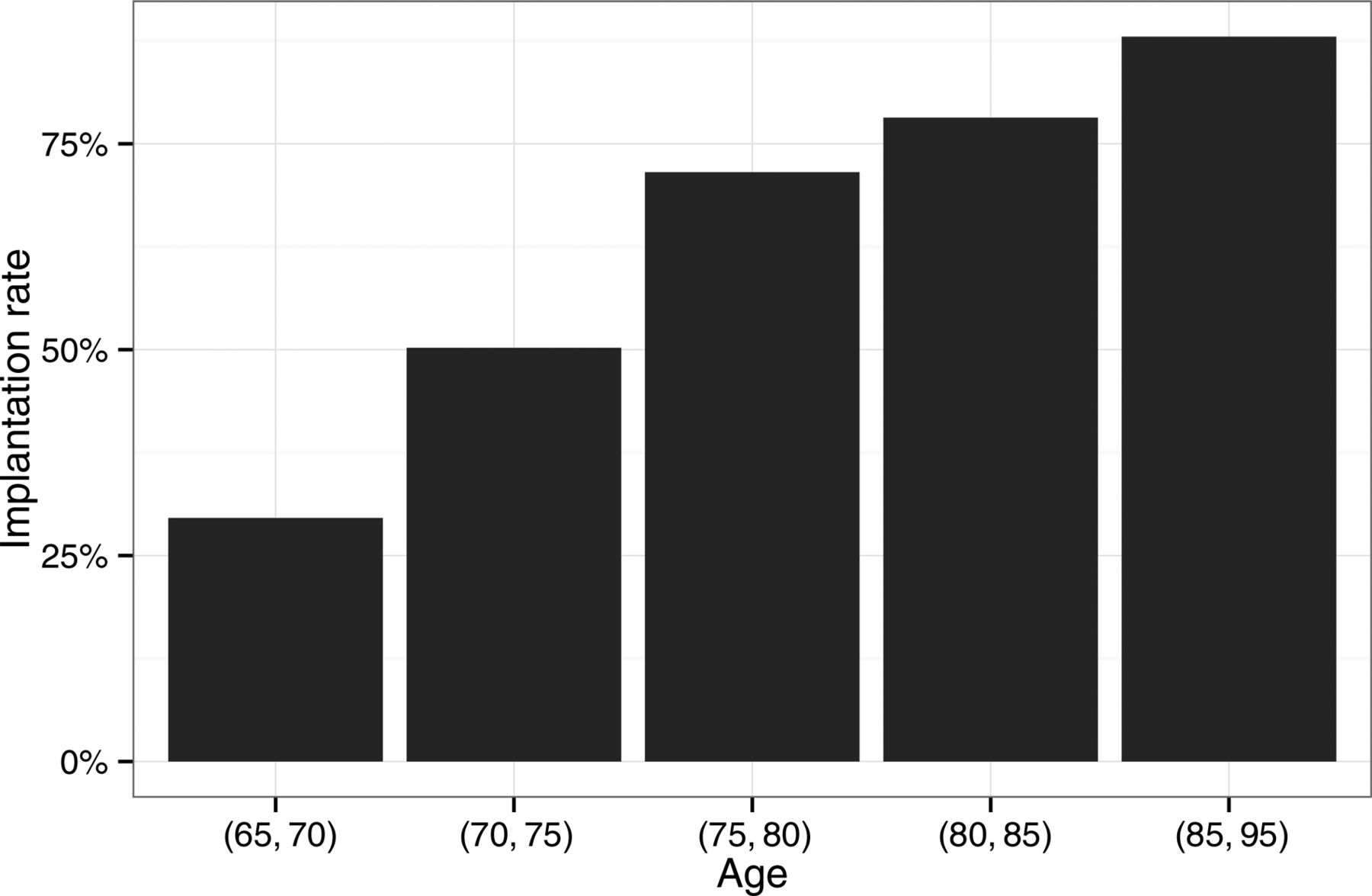
Figure 1 shows that implantation of a biological prosthesis is strongly associated with age, with 29.6% of patients aged 65–70 years receiving a biological prosthesis compared with 79.0% of patients aged over 80 years. Patients who were in atrial fibrillation preoperatively, were statistically more likely to receive a mechanical prosthesis as shown in figure 2 (p<0.001). The changes in the number of MVRs performed each year stratified by prosthesis type are shown in figure 3. The percentage of MVRs performed using a biological prosthesis has increased over time from 28.2% in 2001–2002 to 69.0% in 2010–2011. There is no evidence that hospital volume is associated with propensity for biological prosthesis implantation as shown in figure 4. The percentage of biological prostheses implanted at individual hospitals ranged from 10.5% to 77.3%.

Implantation rates of biological prostheses within discrete age groups.
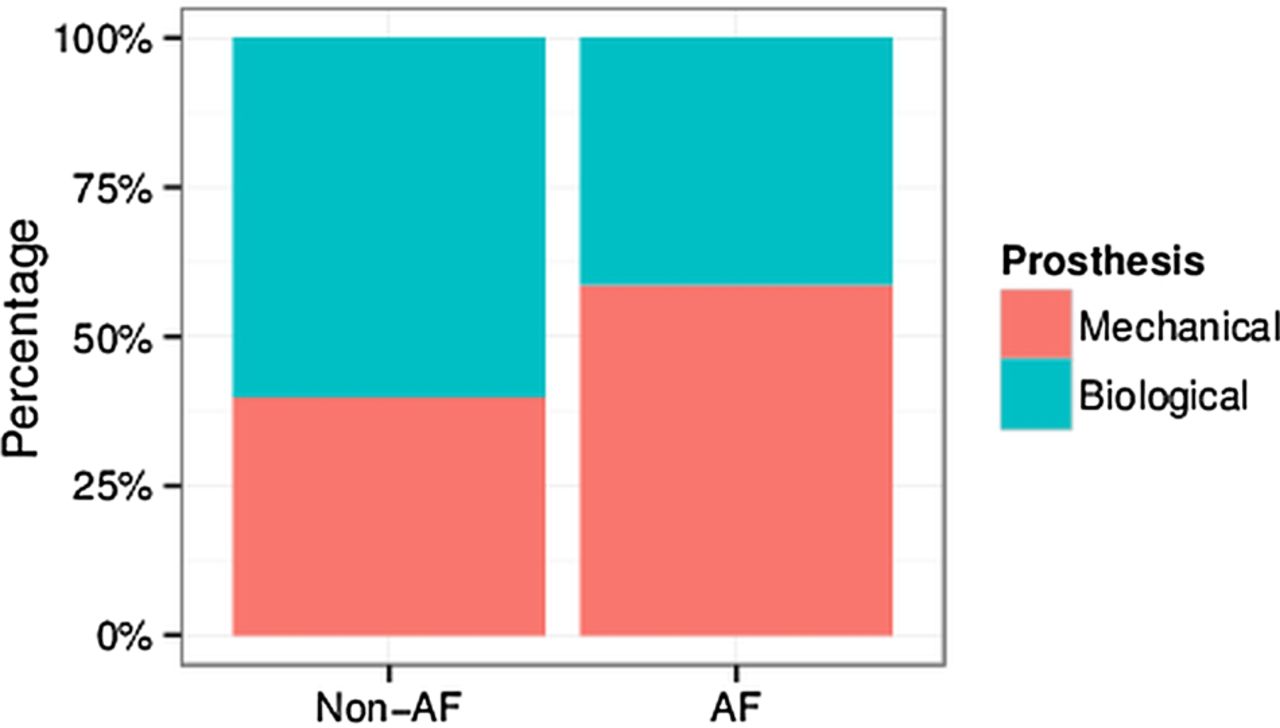
Patients with preoperative atrial fibrillation were more likely to receive a mechanical prosthesis than those who were not in atrial fibrillation (p<0.001; χ2 test).

Number of mitral valve replacements (MVRs) performed each year stratified by prosthesis type.

Hospital MVR volume against biological valve implantation rate for participating hospitals over the duration of the study period.
Propensity score matching
Initially, the study population included 1945 patients who had a MVR using a biological prosthesis, and 1917 patients who underwent MVR with a mechanical prosthesis. A total of 764 and 736 records were discarded from each group, respectively, after matching. This left a well-balanced cohort of patients with 1181 patients in each group (2362 records in total). The postmatching patient characteristics for each group and overall are given in table 1 along with revised standardised difference values. All absolute standardised values are below the 10% level. Figure 5 provides graphical confirmation of balance in the form of a mirrored histogram of the propensity scores in each group before and after matching.

Histogram of propensity scores for biological and mechanical prosthesis groups before and after matching.
In-hospital mortality
In the propensity-matched group, the overall in-hospital mortality was 6.4% (151/2362). In the matched biological prosthesis group, in-hospital mortality was 6.9% (81/1181), and in the matched mechanical prosthesis group it was 5.9% (70/1181). The unadjusted OR in the direction of biological prosthesis was 1.17 (95% CI 0.84 to 1.63, p=0.355).
The actual in-hospital mortality rate in the complete unmatched data was 6.7% (258/3862). In the complete biological prosthesis group it was 7.8% (152/1945), and in the mechanical prosthesis group it was 5.5% (106/1917). The regression adjustment model fitted to the complete (unmatched) dataset yielded an adjusted OR for biological prosthesis of 1.09 (95% CI 0.82 to 1.45, p=0.555). The full model with adjusted ORs and 95% CIs is shown in table 2 and included the following variables significant at p<0.05: age>75 years; female gender; BMI (underweight and overweight); angina Canadian Cardiovascular Society (CCS) class IV; dyspnoea New York Heart Association (NYHA) class IV; creatinine >200 μmol/L; urgent procedure; concomitant tricuspid repair and concomitant CABG.
ORs associated with risk of in-hospital mortality from multiple logistic regression model fitted to the complete unmatched dataset
Survival
In the propensity-matched group, three records were removed due to incomplete follow-up data after procedure. The median follow-up time (defined as time from procedure to either death or last date of follow-up) was 3.9 years (1419 days) with a maximum follow-up time of 10.4 years. There were a total of 749 deaths in the matched group over the study period: 400 (from 1178 records) in the mechanical prosthesis group, and 349 (from 1181 records) in the biological prosthesis group. The Kaplan–Meier survival curves stratified by prosthesis type are shown in figure 6. There was no significant difference between the survival curves (p=0.321) and the unadjusted HR for biological prosthesis was 1.08 (95% CI 0.93 to 1.24).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier survival curves for the propensity score-matched patient cohort stratified by prosthesis type.
In the unmatched data group, there were a further three patients excluded due to incomplete follow-up data (six records in total). There were a total of 1195 deaths in the unmatched group over the study period: 585 (from 1911 records) in the mechanical prosthesis group, and 610 (from 1945 records) in the biological prosthesis group. For the Cox proportional hazards model, dyspnoea was dichotomised to NYHA class IV versus classes I–III. The baseline hazard function was stratified on angina CCS class and diabetes due to evidence of the proportional hazards assumption being violated for these variables. Biological prosthesis was not significant in the final model (HR 1.05, 95% CI 0.93 to 1.19; p=0.434). The full model with HRs and 95% CIs is shown in table 3, and included the following variables significant at the 5% level: age>75 years; BMI (underweight and overweight); dyspnoea NYHA IV; creatinine >200 μmol/L; chronic pulmonary disease; extracardiac arteriopathy; fair or poor left ventricular ejection fraction (LVEF); urgent procedure; concomitant tricuspid repair and concomitant CABG. The Grambsch–Therneau test failed to reject the proportional hazards assumption (p=0.167).
HRs associated with long-term mortality from multiple Cox proportional hazards regression model fitted to the complete unmatched dataset
Discussion
Over the time period studied, half the patients aged over 65 years in the UK undergoing MVR received a bioprosthesis, and half received a mechanical prosthesis. However, although the overall data demonstrates an even split between bioprostheses and mechanical prostheses, the proportion of bioprostheses implanted in this group has increased over time, and older patients were more likely to receive a bioprosthesis. As expected, patients aged over 65 years, but in preoperative atrial fibrillation, were more likely to receive a mechanical prosthesis. Despite current guidelines regarding age and mitral valve prosthesis choice not being followed in the UK, no difference in either in-hospital mortality or mid-term survival was observed between the different prosthesis groups.
This study incorporates data from over 4000 patients aged 65 years and over who underwent MVR plus tricuspid repair or CABG, and represents a ‘real world’ registry study. The large dataset analysed provides complete UK national coverage with robust mid-term follow-up data. Data is validated at each centre prior to submission to the NACSA, and is returned for further validation following cleaning for analysis purposes. The database contains comprehensive data on preoperative patient characteristics, operative details and postoperative in-hospital outcomes. Survival data for the study is well completed with <0.2% of records lost to follow-up.
A limitation of the study is that data on some important long-term outcomes, such as significant thromboembolic or bleeding complications are not available. Additionally, although follow-up extends to over 10 years, the median follow-up time is just under 4 years. As degeneration of biological valves in the mitral position would be expected to occur after the study's median follow-up, mortality related to bioprosthesis degeneration is not available. While for this study we have focussed on patients aged 65 years and over which is consistent with the AHA/ACC recommendation of bioprosthesis implantation, there is, however, a grey area between 65 years and 70 years in the European guidelines. Despite this, the key study finding of lack of overall adherence in everyday practice to the available clinical guidelines regarding bioprosthesis implantation is still striking, as 38.9% of patients aged over 70 years received a mechanical prosthesis. There is also marked variation between hospitals with respect to their choice of prosthesis type.
There are two historical randomised trials comparing mechanical and biological valve use. The final report of the Department of Veterans Affairs trial at 15 years of follow-up did not report a statistically significant difference for all-cause mortality after MVR between the mechanical valve and bioprosthesis subgroups.13 In a similar fashion, data from the Edinburgh trial failed to show a significant difference in survival at 12 years for the mechanical and bioprosthetic MVR cohorts.14 This effect remained unchanged at 20 years for all survivors, although survival with an intact prosthesis or without a major event was significantly better in the mechanical MVR subgroup.15 Both trials enrolled a limited number of patients over 65 years of age, thus making meaningful extrapolation of results into guidelines practically impossible for this age group.
Mitral valve repair, when feasible, remains the procedure of choice in all age groups including the elderly.16 ,17 When repair is not an option, ‘which prosthesis type is most appropriate’, remains to be answered. In this study, in-hospital, as well as mid-term outcomes for the propensity-matched groups, did not demonstrate any difference in survival. A few groups have demonstrated similar findings when assessing the impact of valve type on survival in the elderly.18–21 The 10-year survival in patients after MVR with biologic or mechanical valve prostheses was retrospectively analysed at an institutional level for 1139 consecutive patients.22 Using propensity-matching scores, it was shown that choice of prosthesis was not a predictor of survival in patients aged 60 years or older. The limitations of this report lay in the fact that the over 60-year-group sizes for cohorts were considerably small, and the study has been conducted for two specific commercially available valves. Beyond survival, Kurlansky et al showed no advantage in quality of life when comparing mechanical versus bioprosthetic valve replacement for patients aged 65–75 years.21
Our study has demonstrated a significant increase in the proportion of bioprosthesis implanted in this cohort over time. Across the USA for the period 1998–2005, the overall use of biological prostheses doubled from 16.9% in 1998 to 36.5% in 2005.23 The implantation rate of biological prostheses for patients aged <65 years tripled, while that of patients aged ≥65 years had doubled. Further data from the Society of Thoracic Surgeons Adult Cardiac Database documented a decrease from 68% in 2000 to 37% in 2007 regarding the use of mechanical mitral prostheses.24
Guidelines such as those studied here are produced by professional societies and other organisations to help practising clinicians deliver optimal patient treatment. Infrequently, there is a large body of randomised clinical trial data that clearly indicates how clinicians should practice. In the majority of cases, there is a mixture of registry data, large and small patient series and consensus of expert opinion that is used to synthesise guidance. While healthcare is becoming increasingly regulated, it still largely remains up to individual clinicians, or clinical groups, to make judgements on how they will adopt and implement published guidance in conjunction with their patients. Full adherence to guidelines in this scenario would not be expected, as patient preference and contraindications for anticoagulation need to be considered. However, it is perhaps surprising to see such marked variability in practice in the UK with respect to prosthesis choice in the mitral position in patients aged 65 years and over. This variation is unlikely to be explained by differences in case-mix alone, and implies that the published guidance is not widely accepted.
This observed variability and lack of adherence to published guidelines could reflect the relatively weak evidence from which the guidelines are derived. Other possible reasons for the greater use of mechanical prostheses in patients aged 65 years and over could be the fact that some surgeons believe inserting a mechanical prosthesis is easier and safer. Surgeons may also be inserting more mechanical prostheses because of concerns about the operative mortality associated with redo surgery in the future. Developments in anticoagulation strategies may further influence surgical decision making in favour of mechanical prostheses. However, despite encouraging large animal data for thromboembolic prophylaxis with dabigatran in the setting of mechanical heart valve replacement,25 ,26 recent data from a randomised phase 2 study has associated dabigatran with increased rates of thromboembolic and bleeding complications compared to warfarin.27 Conversely, the development of mitral valve-in-valve transcatheter implantation techniques28 may lead to an increase in the implantation of bioprostheses.
The presented data reflects the working practice within the UK, and demonstrates that the current guidelines around age and mitral valve prosthesis choice are not being followed for patients aged 65 years and over. With regards to in-hospital and mid-term mortality, this study demonstrates that there is no difference between prosthesis types. This study has not, however, addressed a number of important outcomes with regards to prosthesis choice, including structural deterioration, the need for redo surgery, and morbidity such as bleeding complications. In the future, this may be possible through the linkage of clinical and administrative datasets. Further research into why the current guidelines are not being followed would provide interesting information not just about mitral valve surgery, but also about clinical guidelines in general.
Limitations
There are a number of limitations to this study. First, the data reflects a national clinical registry. While we are able to adjust for a number of perceived confounders when comparing outcomes between biological and mechanical prostheses, it is conceivable that there are unmeasured confounding variables. On the other hand, this data reveals insight into actual real-world practice. Second, the data quality of national registries is generally not perfect. Missing data and transcriptional errors were present, and while we attempted to resolve these using reproducible algorithms and statistical imputation methodology, we have potentially underestimated the SEs. Third, cause of death could not be established using long-term tracking data; neither could other endpoints, such as valve failure or other cardiovascular events; however, it is possible that differences may exist in these endpoints.
Key messages
What is already known on this subject
-
Current guidelines recommend that most patients aged ≥65 years should undergo mitral valve replacement using a biological prosthesis.
-
It is not clear whether guidelines relating to age and prosthesis choice are being followed in UK practice.
What this study adds
-
The presented data reflects the working practice within the UK, and demonstrates that the current guidelines around age and mitral valve prosthesis choice are not being followed for patients aged 65 years and over.
-
There is no difference in short-term or mid-term outcomes for these patients, according to prosthesis choice, thereby questioning existing guidance.
References
Footnotes
-
Contributors ID, SWG, GLH and BB conceived the study, drafted and revised the paper. GLH and SWG cleaned the data. GLH conducted the analysis. RP, SL, NM and FW contributed data to the study and revised the draft paper. All authors approved the final version of the paper for submission. BB is the guarantor for the study.
-
Funding GLH was funded by Heart Research UK [Grant RG2583].
-
Competing interests None.
-
Ethics approval The NACSA has section 251 approval. As only pseudonymous, non-identifiable data were used for this study, ethical approval was not required.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement The data sharing policy for NICOR data can be found at the relevant website: http://www.ucl.ac.uk/nicor.