Article Text

Abstract
Objective Owing to its variable clinical course, risk stratification is of paramount importance in non-ischaemic dilated cardiomyopathy (DCM). The goal of this study was to investigate the long-term prognostic significance of late gadolinium enhancement (LGE) as detected by contrast-enhanced cardiovascular magnetic resonance (CE-CMR) in patients with DCM.
Design Observational cohort study.
Setting University hospital.
Patients 184 consecutive patients with DCM.
Measurements CE-CMR was performed on a 1.5 T clinical scanner. Presence, extent and patterns of LGE were determined by two independent observers.
Outcome measures Patients were followed for the composite end point of cardiac death, hospitalisation for decompensated heart failure, or appropriate implantable cardioverter defibrillator discharge for a mean±SEM of 685±30 days.
Results LGE was detected in 72/184 patients (39%) and was associated with a lower left ventricular (LV) ejection fraction (31% (20.9–42.2%) vs 44% (33.1–50.9%), p<0.001), higher LV end-diastolic volume index (133 (116–161) ml/m2 vs 109 (92.7–137.6) ml/m2, p<0.001) and higher LV mass (80 (67.1–94.8) g/m2 vs 65.8 (55.2–82.9) g/m2, p<0.001). Patients in whom LGE was present were more likely to experience the composite end point (15/72 vs 6/112, p=0.002). Receiver operating characteristic curve analysis revealed a LGE of >4.4% of LV mass as optimal discriminator for the composite end point. When entered into multivariate Cox regression analysis, LGE retained its independent predictive value, yielding an associated HR of 3.4 (95% CI 1.26 to 9).
Conclusion The presence of LGE in this large DCM patient cohort is associated with pronounced LV remodelling, functional impairment and an adverse outcome. Further research is necessary to determine whether these findings will aid the clinical management of DCM patients.
- Cardiomyopathy
- dilated
- MRI
- prognosis
Statistics from Altmetric.com
Non-ischaemic dilated cardiomyopathy (DCM) accounts for a substantial proportion of cardiovascular morbidity and mortality in developed countries.1–3 Despite the overall serious prognosis, with a 10-year mortality of over 40%,4 the individual clinical course is highly heterogeneous, ranging from asymptomatic patients to those suffering from severe congestive heart failure and sudden cardiac death. Despite the identification of a series of factors that are associated with an adverse prognosis, such as age,4 male gender,2 degree of systolic dysfunction,5 QRS duration6 and cardiac biomarkers such as natriuretic peptides and troponins,7 risk stratification remains challenging, and better tools are necessary to identify highest risk patients, who are most likely to benefit from early aggressive interventions such as the implantation of implantable cardioverter defibrillators (ICDs).
Cardiac MRI has become the ‘gold standard’ for the assessment of cardiac function and mass.8 In addition, the administration of gadolinium contrast agents allows the detection of areas of late gadolinium enhancement (LGE). Originally used for the detection of myocardial infarction and viability assessment, different patterns of LGE have been found in a large number of cardiac diseases, including cardiomyopathies. McCrohon et al were the first to report the presence of a ‘mid-wall’ enhancement in patients with DCM, which was distinct from the LGE pattern seen in ischaemic cardiomyopathy.9 Subsequent studies reported the presence of LGE in up to 42% of patients with DCM.10
In addition to its diagnostic value, contrast-enhanced cardiovascular magnetic resonance (CE-CMR) has recently shown promising results in risk assessment in patients with cardiomyopathies. The presence of LGE has been shown to be associated with an increased risk of adverse events and to add independent information to established risk factors in patients with DCM,8 10 11 and more recently in patients with hypertrophic cardiomyopathies.12 13
Owing to the major impact this finding might potentially have with regard to the clinical management of DCM patients and in light of the limited number of patients included in the aforementioned studies, our goal was to assess the prognostic significance of LGE in a larger population of clinically stable patients with DCM.
Methods
Study population
The study population consisted of 184 consecutive patients with DCM who were referred to the Cardiomyopathy Center at the University Hospital Heidelberg between May 2005 and April 2008.
CE-CMR was performed in these patients as part of the standard clinical evaluation for patients with cardiomyopathy at our institution unless one of the following contraindications to MR was present: cardiac pacemaker/ICD; other metallic implants not MR compatible; lack of patient informed consent; severe claustrophobia; severe obesity preventing the patient from entering the scanner bore; pregnancy; lactation. Chronic renal failure with an estimated glomerular filtration rate <30 ml/min/1.73 m2 was added as an exclusion criterion in July 2007 as a consequence of the advisory of the European Medical Board regarding nephrogenic systemic fibrosis following the administration of gadolinium contrast media.
The diagnosis of DCM was based on the 1995 WHO/International Society and Federation of Cardiology criteria.14 Patients had to exhibit depressed systolic function (left ventricular ejection fraction (LV-EF) <50%) on a non-CMR study in the absence of significant coronary artery disease (defined as ≥50% luminal stenosis on coronary angiography and/or a history of coronary revascularisation or myocardial infarction), valvular disease, hypertensive heart disease and congenital abnormalities. All patients had chronic heart failure of at least 12 months duration and were examined in a clinically stable condition (New York Heart Association (NYHA) functional class ≤III). No patient showed signs or symptoms of ongoing myocarditis. Patients initially diagnosed as having DCM displaying a subendocardial or transmural pattern of late enhancement suggestive of myocardial infarction were excluded from the final analysis. Patients with a normal LV-EF on CMR (>55%) were also excluded.
All patients were followed by either direct communication (follow-up visit or telephone interview) for the occurrence of (cardiac) death, ICD implantation, ICD discharge, hospitalisation for decompensated congestive heart failure, or heart transplantation. Mean±SEM follow-up duration was 658±30 days. For outcome analysis, the end point was defined as a composite of cardiac death, appropriate ICD discharge for ventricular fibrillation/tachycardia, and hospitalisation for heart failure. If patients underwent heart transplantation, the follow-up data were censored at the time of transplantation.
All patients gave their informed consent. The study protocol was approved by the institutional ethics committee.
CMR scan protocol
CMR was performed on a 1.5 T clinical scanner (Achieva Intera; Philips Healthcare, Best, The Netherlands) equipped with a five-element cardiac phased-array receiver coil. Cine images were obtained using a breath-hold segmented-k-space balanced fast-field echo sequence (SSFP) employing retrospective ECG gating in long-axis planes (two-chamber, four-chamber and three-chamber views) as well as in contiguous short-axis slices (gap 2 mm) covering the whole ventricles from the annulus of the atrioventricular valves to the apex. Typical imaging parameters were: field of view 350×350 mm2; repetition time/echo time 2.8/1.4 ms; acquired voxel size 2.2×2.2×8 mm3; flip angle 60°; reconstructed voxel size 1.3×1.2×8 mm3. Delayed contrast-enhanced images were acquired 10 min after the intravenous administration of gadolinium diethylenetriaminepenta-acetate (Magnevist; Bayer Schering Pharma, Berlin, Germany; 0.2 mmol/kg) using a three-dimensional inversion-recovery gradient echo pulse sequence in sequential short-axis slices covering the whole ventricle as well as two-chamber and four-chamber views. Inversion time was adjusted to null normal myocardium and was typically 180–240 ms.
CMR analysis
All analyses were performed on a commercially available workstation (Viewforum; Philips Healthcare) equipped with semi-automated software for volumetric analysis. Results for ventricular volumes, ejection fraction and LV myocardial mass were derived from short-axis slices after manual tracing of epicardial and endocardial borders, excluding papillary muscles from the myocardium.
The presence and extent of late enhancement were evaluated by two independent observers experienced in CE-CMR (SL and HS), who were blinded to clinical data and outcome. To exclude artefact, LGE was deemed present only if visible in two orthogonal views. The pattern of LGE was characterised as mid-wall, epicardial, patchy/foci, or diffuse. For quantification of fibrosis, LGE was defined as areas with a signal intensity >2 SD above the mean signal intensity of remote myocardium in the same short-axis slice.11 Areas were measured by manual planimetry and expressed as percentage of myocardial mass.
Statistical analysis
Continuous variables were expressed as mean±SEM or as median with IQR for non-parametric variables. Differences between two groups were compared using the Student t test or Mann–Whitney U test. In cases of more than two groups, differences were compared using analysis of variance or the Kruskal–Wallis test. Categorical variables were expressed as counts and percentages and compared by χ2 test or Fisher exact test, respectively. Survival curves were estimated by the Kaplan–Meier method and compared by the log-rank test. Univariate and multivariate Cox proportional hazards regression analysis was performed to calculate HRs and 95% CIs.
For all analyses, p<0.05 was regarded as significant. All statistical analyses were carried out using SPSS V.14.0.
Results
Baseline patient demographics are displayed in table 1. The majority of patients were in symptomatic heart failure (NYHA class II and III). In adherence with current treatment guidelines, almost all patients received β blockers and ACE inhibitors or angiotensin receptor blockers, respectively (table 1).
Patient demographics according to presence or absence of late gadolinium enhancement (LGE)
Late gadolinium enhancement
LGE was present in 72/184 (39%) patients (LGEpos). Of these, 27 exhibited a septal mid-wall enhancement, while 45 showed a non-mid-wall enhancement pattern (figure 1). With regard to the dichotomous presence of LGE, there was agreement between the two observers in all but one patient. This patient was assigned to the LGE-negative group (LGEneg) after a reading by a third blinded observer (DL). Compared with patients without any late enhancement, LGEpos patients showed more severe clinical heart failure, as reflected in a higher prevalence of patients in NYHA functional class III and, consequently, the more frequent use of diuretics and spironolactone. In addition, the presence of LGE was associated with higher serum levels of NT-proBNP (table 1). No significant differences were noted between patients with different enhancement patterns (online supplementary table 1A).

Presence and patterns of late gadolinium enhancement (LGE). LGE was present in 72/184 (39%) of patients with dilated cardiomyopathy. Representative short-axis slices illustrate the different patterns of LGE that were detected. In addition to the ‘classic’ mid-wall enhancement, three distinct patterns of non-mid-wall LGE were found. Arrowheads indicate areas of LGE.
With regard to quantification of LGE, linear regression analysis showed good interobserver and intraobserver reliability (R2=0.92 and R2=0.98, respectively). Among LGEpos patients, the median extent of fibrosis was 2.9% of LV mass (range 0.3–35.5%). Percentage of LGE was not related to gender, age, NYHA functional class or any other clinical baseline characteristic.
CMR parameters
Functional and volumetric CMR analysis revealed an association between the presence of LGE, more pronounced LV remodelling, and a higher degree of systolic dysfunction. As depicted in table 2, LGEpos patients exhibited larger LV volumes, a higher LV mass index and a lower LV-EF than patients in whom LGE was absent. Interestingly, no significant differences could be found with regard to right ventricular analysis. Again, CMR parameters were comparable between patients with different enhancement patterns, with the exception of cardiac index (online supplementary table 2A).
Cardiovascular magnetic resonance data according to presence or absence of late gadolinium enhancement (LGE)
Among LGEpos patients, no significant correlations between the extent of LGE and any of the functional CMR parameters could be established.
Outcome
During the follow-up period, five patients suffered cardiac death; no non-cardiac deaths were recorded. The composite end point occurred in 21 patients (table 3).
Incidence of cardiac events during follow-up
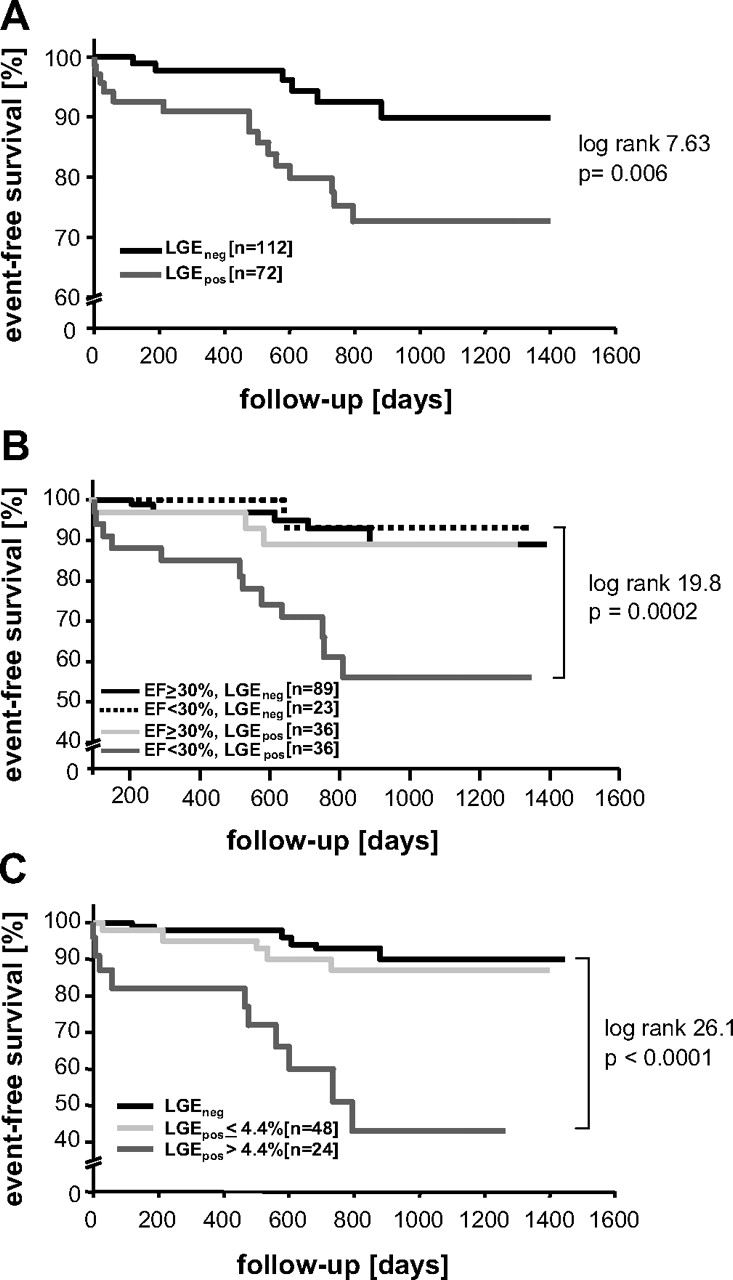
While a trend towards higher cardiac mortality among LGEpos patients could be observed, this failed to reach statistical significance in light of the small total numbers (4/72 LGEpos patients vs 1/112 LGEneg patients, p=0.08). However, the presence of LGE was associated with a markedly higher risk for the predefined composite end point (15/72 LGEpos patients vs 6/112 LGEneg patients, p=0.002). Kaplan–Meier analysis revealed a significantly worse event-free survival rate during long-term follow-up among LGEpos patients (figure 2A). Interestingly, when patients were further stratified according to degree of systolic dysfunction, the prognostic value of LGE was limited to those patients with a severely impaired LV function (LV-EF <30%) (figure 2B). The incidence of adverse cardiac events was not associated with specific LGE pattern (online supplementary table 3A).

{kind=link}
{kind=link}
Event-free survival according to presence and extent of late gadolinium enhancement (LGE) and late ventricular ejection fraction (LV-EF). Kaplan–Meier analysis illustrates the worse long-term outcome in LGEpos patients with regard to incidence of the composite end point of cardiac death, appropriate implantable cardioverter defibrillator discharge, and hospitalisation for decompensated heart failure (A). The prognostic value of LGE strongly depends on underlying systolic dysfunction and appears to be confined to patients with a LV-EF < 30% (B). When LGEpos are further stratified into those with an area of LGE above or below the receiver operating characteristic curve specified discriminator of 4.4% LGE of LV mass, it becomes evident that those with only mild LGE have a prognosis comparable to those in whom LGE is absent (C).
With an associated HR of 3.5, the presence of LGE was among the strongest univariate predictors for the combined end point, surpassed only by age ≥70 years. The multivariate model contained all univariate predictors in addition to NYHA class and male gender. LGE remained an independent predictor in addition to age and LV end-diastolic volume index (table 4).
Proportional hazard regression analysis for incidence of the composite end point
Among LGEpos patients, a strong association between the extent of LGE and the incidence of the combined end point could be noted (5.6% (2.7–11.4%) vs 2.6% (1.4–4.4%), p=0.01). Receiver operating characteristic curve analysis revealed a LGE percentage of 4.4 as optimal discriminator (area under the curve 0.71±0.08, p=0.01) for the occurrence of the combined end point with an associated HR of 5.28 (95% CI 1.8 to 15.5). Notably, when patients were divided into three groups according to (1) absence of LGE, (2) LGE ≤4.4% of LV mass and (3) LGE >4.4% of LV mass, Kaplan–Meier analysis revealed a difference of event-free survival only for the third group (figure 2C).
Discussion
The findings of this study support the use of CMR as a risk-stratification tool in chronic heart failure. In this largest cohort of patients with DCM so far studied, the presence of LGE was associated with pronounced LV remodelling and constituted an independent predictor for adverse cardiac outcome.
Fibrotic changes in hearts of patients with DCM have been recognised in histopathology for decades15 16 and can be classified into either diffuse (interstitial) or segmental (replacement) fibrosis.17 18 The mechanisms believed to contribute to the development of myocardial fibrosis are multiple and include inflammation, neurohumoral changes and microvascular ischaemia.19 While its limited spatial resolution does not permit the visualisation of interstitial fibrosis, macroscopic areas of replacement fibrosis can reliably be detected by CE-CMR in patients with DCM. In the present cohort, LGE was found in 39% of patients, which is comparable to previous studies reporting incidences between 26% and 42%,6 10 and in line with findings from explanted hearts of patients with DCM in whom segmental fibrosis can be detected in 33%.17
The process of adverse cardiac remodelling—that is, the increase in ventricular volumes and myocardial mass and the change in chamber geometry—is central to the current pathophysiological understanding of chronic heart failure. On a cellular level, the remodelling process is characterised by several changes, including cardiomyocyte hypertrophy and fibroblast proliferation.19 20 In the present study, LGE was associated with marked increases in ventricular volumes and myocardial mass as well as severely impaired systolic function, providing further evidence for the close relationship between myocardial fibrosis and adverse remodelling, which has been observed in both animal and human myocardium.21 22
Despite the close association between presence of LGE and unfavourable ventricular function and geometry, it retained an independent prognostic value with an associated HR of 3.4 for the composite end point. Of note, the extent of fibrosis appears to be a critical factor for an adverse outcome. Among the LGEpos patients in our study population, only those with fibrosis extending to 4.4% of LV mass had an unfavourable prognosis, supporting earlier results from Assomull et al.11
Why is the presence of LGE an independent predictor for adverse clinical outcome? Among others, one likely explanation is the promotion of re-entry mechanisms by focal fibrosis, causing malignant arrhythmias. Areas of fibrosis detected by CMR have been identified as substrates for inducible ventricular tachycardia in patients with ischaemic heart disease23 and, more recently, in patients with DCM.24 These findings are supported by data from DCM patients undergoing ICD implantation.10 In addition to the impact on the electrophysiological properties of the heart, increasing amounts of fibrosis also lead to elastomechanical alterations, with a loss of ventricular compliance25 and subsequent increases in filling pressure, promoting the development of pulmonary and peripheral oedema.
One important observation of this study is that the prognostic significance of LGE is dependent on the degree of underlying LV dysfunction. Subgroup analysis revealed that the presence of fibrosis is associated with an unfavourable outcome only in patients with severely impaired LV function, which may reflect greater vulnerability to the above effects of fibrotic changes on electrophysiological and mechanical properties. Conversely, patients with a LV-EF <30% and no evidence of fibrosis on CMR had a fairly benign outcome, supporting the additive prognostic impact of LGE.
The patterns of LGE observed in patients with DCM are distinct from that seen in myocardial infarction, making CE-CMR a valuable tool for determining the aetiology of impaired systolic function.9 Interestingly, whereas some groups have reported the presence of only mid-wall enhancement in patients with DCM,9 11 others, including us, have found a variety of enhancement patterns, including not only mid-wall but also epicardial, diffuse and focal patterns.6 10 The reasons for this discrepancy are not yet clear. Histopathological examination of explanted hearts of patients with DCM shows patterns of fibrosis that conform with all of the observed LGE characteristics.15 16 20 At this point, it is not clear whether the various fibrotic patterns have different underlying causes or even represent different aetiologies of DCM. Although mid-wall enhancement is often observed in patients with myocarditis26 and may persist in patients who develop DCM, it is not specific to myocarditis, but can also be observed as a characteristic finding in certain familial DCM forms such as lamin mutations.27 Furthermore, epicardial and patchy patterns have also been described in DCM as well as myocarditis. In the present study, there is no evidence that the prognostic significance of LGE is limited to certain patterns, which is in line with the findings of Wu et al.10 However, these analyses need to be interpreted with caution because of the small number of patients and events.
Limitations
Although CE-CMR is a valuable tool for detecting segmental fibrosis in patients with DCM, its limited spatial resolution does not allow the evaluation of diffuse fibrosis. The presence of LGE on CMR alone correlates only poorly with the collagen volume fraction calculated from endomyocardial biopsies.18 One promising approach for the evaluation of microscopic fibrosis is the implementation of post-contrast T1 mapping sequences, which use the concept that gadolinium accumulation in interstitial fibrosis leads to shortening of T1 relaxation times.28–30 Endomyocardial biopsies were not routinely performed for the diagnosis of DCM in this patient cohort, in conformation with current guidelines. None of the patients had signs or symptoms of ongoing myocarditis; however, it is very likely that a subset of the patients in this study had myocarditis which developed into DCM. Previous studies reported that myocarditis is the cause of fibrosis in ∼10% of patients with DCM.4
A general limitation of the use of CE-CMR as a risk-stratification tool in patients with DCM is the current restrictions on application of gadolinium contrast agents in patients with chronic renal insufficiency because of the risk of nephrogenic systemic fibrosis. It is known, however, that patients with chronic renal failure together with heart failure are at high risk.31
Conclusions
The use of CE-CMR for risk stratification of patients with CCM has produced promising data in single-centre studies. Results seem to be especially encouraging with regard to the identification of patients at high risk of developing malignant arrhythmias. However, there is a need for larger, multi-centre trials to confirm these findings and to determine whether they will aid therapeutic decisions.
Acknowledgments
We thank Birgit Hörig and Angela Stöcker-Wochele for excellent technical assistance with acquisitions of all MR scans.
References
Supplementary materials
Web Only Data hrt.2010.205542
Files in this Data Supplement:
Footnotes
Competing interests None.
Ethics approval This study was conducted with the approval of the ethics committee of the University of Heidelberg.
Provenance and peer review Not commissioned; externally peer reviewed.