Article Text

Abstract
Obejctive To compare left ventricular (LV) systolic performance and contractility in patients with heart failure and normal ejection fraction (HFNEF), compared with patients with heart failure and reduced ejection fraction (HFREF) and healthy subjects using newer echocardiographic techniques.
Design A case–control trial.
Setting University teaching hospital (tertiary referral centre).
Patients Sixty healthy control subjects (53±10 years), 112 patients with HFNEF (74±12 years) and 175 patients with HFREF (67±13 years).
Interventions All underwent standard two-dimensional, Doppler and speckle-tracking echocardiography.
Main outcome measures Effective arterial (Ea) and LV end-systolic elastance (Ees), stress-corrected mid-wall shortening, preload recruitable stroke work, two-dimensional strain and torsion. Comparisons were adjusted for age, gender and body size.
Results Besides diastolic dysfunction, patients with HFNEF had impaired load-independent ventricular contractility with a progressive decrease of the corrected Ees from controls (2.9±0.8 mm Hg/g) to HFNEF (2.2±0.9 mm Hg/g) followed by HFREF (0.8±0.3 mm Hg/g; all p<0.001). Ventricular-arterial coupling ratio was preserved in the HFNEF subgroup (normal 0.48±0.09 vs 0.65±0.16; p=NS) at the expense of both increased LV systolic stiffness and Ea. In addition, there was progressive decrease of global 2D circumferential, radial and longitudinal strain as well as torsion from normal, HFNEF to HFREF groups, even after adjustment for LV end-systolic wall stress or end-diastolic volume (all p<0.01). About 50% of patients with HFNEF had ≥1 global strain or torsion parameter depressed below normal after correction for LV end-systolic wall stress, with >85% falling below their corresponding stress-corrected mean.
Conclusions Impaired myocardial contractility is evident in many patients with HFNEF and this may contribute towards pathophysiology of HFNEF more than previously thought.
- Contractility
- heart failure
- echocardiography
- tissue Doppler
Statistics from Altmetric.com
Introduction
About half of patients with heart failure have a normal or near-normal left ventricular (LV) ejection fraction (HFNEF), and they have a similarly poor prognosis as those with heart failure and reduced ejection fraction (HFREF). HFNEF is a growing health problem and is intriguing. The precise underlying pathophysiology is still debated and there is currently no evidence-based treatment for improving survival.1
We and others have previously reported abnormalities in regional systolic function at rest in patients with HFNEF using tissue Doppler velocities, particularly in long-axis function. However, these studies were criticised for lack of pre- or afterload adjustment and therefore not genuinely reflecting LV contractility.2–7
Recently, speckle-tracking echocardiography (STE) has allowed measurement of myocardial deformation in longitudinal, radial, circumferential and transverse directions in addition to ventricular rotation and torsion, which are not subject to the angle of insonation, tethering and translation effects associated with tissue Doppler velocities. It provides mechanistic insight into the ventricular pathophysiology of HFNEF at rest and during exercise. Recent studies using STE have demonstrated in smaller numbers of patients with HFNEF that LV systolic longitudinal and radial strains are reduced,8 9 with significantly lower systolic longitudinal functional reserve and systolic rotation on exercise.9 In addition, Borlaug et al10 demonstrated with standard echocardiography that in asymptomatic hypertensive heart disease myocardial contractility (assessed by circumferential mid-wall fractional shortening) increases to match arterial load but that progression to HFNEF is associated with both impaired contractility and increased passive myocardial stiffness.10
We sought to compare resting LV systolic performance, contractility and myocardial deformation in three groups of subjects: healthy controls, patients with HFNEF and patients with HFREF, by assessing their LV ventricular geometric, mass, systolic stiffness, contractility and ventricular–arterial coupling using standard two-dimensional, Doppler and STE.
Methods
Subjects
A prospective cohort of 287 patients was recruited after hospitalisation for pulmonary oedema due to heart failure, with a documented LV ejection fraction (LVEF) by two-dimensional (2D) echocardiography within 72 h of admission. Among the patients, 112 met the criteria of the Heart Failure and Echocardiography Associations of the European Society of Cardiology for HFNEF with LVEF≥50%, and 175 had HFREF with LVEF<50% by echocardiography and had signs and symptoms of heart failure.11 We used the clinical diagnosis of the admitting doctor and verified results of subsequent care of the patients; this essentially represented the signs and symptoms of congestive heart failure (orthopnoea, raised jugular venous pressure, gallop sounds, lung crepitations, pulmonary oedema) with radiographic evidence of pulmonary congestion and/or clinical response to intravenous diuretics sufficient to account for the disease.
Serum B-type natriuretic peptide (BNP) was measured by fluorescence immunoassay at the time of echocardiography using a triage BNP test (Biosite Diagnostics, California, USA). Sixty normal healthy subjects from community who presented for a routine physical evaluation, and had normal echocardiographic findings were included as a control group. We excluded patients with heart failure presenting with acute coronary syndromes. All eligible patients were carefully screened for non-cardiac causes of heart failure symptoms. Lung diseases such as chronic obstructive pulmonary disease were ruled out by chest radiography and lung function tests. Other exclusion criteria included (1) atrial fibrillation, sick sinus syndrome, second- or third-degree heart block with or without a pacemaker, (2) significant congenital or valvular heart disease, (3) infiltrative, restrictive or hypertrophic cardiomyopathy, (4) obesity using Chinese standards of a body mass index >25 kg/m2, and/or waist circumference >90 cm for men and >80 cm women,12 (5) primary renal disease or serum creatinine ≥250 μmol/l and/or estimated glomerular filtration rate ≤30 ml/min/1.73 m2, (6) primary hepatic disease or cirrhosis, (7) systemic infection, (8) pregnancy and (9) suboptimal image quality on echocardiography. Written informed consent was obtained from all subjects and the study was approved by the institution's research ethical committees.
Echocardiography
Comprehensive echocardiographic assessment was performed using a multi-frequency matrix probe (Vivid7, GE Healthcare, Chalfont St Giles, UK) with patients lying in the left lateral decubitus position, and results were interpreted in a blinded fashion. LV dimensions, volumes, ejection fraction, wall stress and LV mass indexed to body surface area (BSA) were measured offline using standard methods. Sex-specific definitions for ventricular hypertrophy based on LV mass index (>95 g/m2 for women and >115 g/m2 for men) were used.13 The LVEF was calculated by a modified biplane Simpson's method from apical four- and two-chamber views. Stroke volume (SV) was calculated by the difference between LV end-diastolic volume (LVEDV) and end-systolic volume (ESV) derived from Simpson's method, and was used to calculate cardiac index (SV × heart rate/BSA). Endocardial fractional shortening (FS) was calculated as the LV dimension difference between end-diastole and end-systole divided by the LV end-diastolic dimension. Mid-wall fractional shortening (MWFS) was calculated by the following formula: MWFS=((LVIDd + SWTd/2 + PWTd /2)−(LVIDs + inner shell))/(LVIDd + SWTd /2 + PWTd/2), where inner shell=((LVIDd + SWTd /2 + PWTd /2)3−LVIDd3 + LVIDs3)1/3−LVIDs with LVID as the LV dimension, SWT as the septal wall thickness, PWT as the posterior wall thickness, s as in end-systole and d in end-diastole.14 The stroke work index was calculated as the product of SV and mean arterial blood pressure indexed to BSA.15 Left ventricular end-diastolic pressure was estimated from echo-Doppler and tissue-Doppler echocardiography. Early (E) and late (A) transmitral flow velocities, and deceleration time of early filling were measured by pulsed-wave Doppler echocardiography. The medial mitral annular early diastolic velocity (e′) by pulsed-wave tissue Doppler imaging was measured for calculation of E/e′ ratio.16 Brachial blood pressure was determined by sphygmomanometry. LV end-systolic pressure (LVESP) was approximated as 0.9 × systolic blood pressure (SBP).17 18
Speckle tracking
The LV apical long, four- and two-chamber images and short-axis views at basal, mid-papillary and apical levels at frame rates between 40 and 80 frames/s were used for assessing 2D LV longitudinal, radial, circumferential strains and rotation. Global strain was derived from the average of 18 segments in the longitudinal, or radial and circumferential planes—that is, six evenly divided segments in each of the three long-axis or short-axis views. LV torsion or twist was calculated as the net difference of peak systolic rotational strain between six basal and six apical segments. The end of systole was defined as the point of aortic valve closure. In each study subject, we verified that the heart rate for the cardiac cycle in which the timing of aortic valve closure was ascertained was the same as that used for analysis of the LV rotation parameters. Tissue Doppler imaging and 2D strain images were analysed offline on a PC workstation (EchoPAC version BTO8 GE-Vingmed, Horten, Norway) equipped with custom software as previously described.19
Ventricular contractility assessment
Load-independent myocardial contractility was assessed by (1) the relationship between MWFS and circumferential end-systolic wall stress (cESS) using the two-shell method of Shimizu and others,10 14 20 (2) LV end-systolic elastance (Ees=0.9×SBP/ESV) indexed to BSA and corrected by either LV mass, EDV or LV mass/EDV ratio17 18 21 and (3) preload recruitable stroke work index (PRSW) by a validated single-beat method.22 To minimise afterload dependence, stress-corrected MWFS (sc-MWFS) and stress-corrected FS (sc-FS) were determined as a percentage of that predicted for any given wall stress using the regression equations derived from the healthy control population. sc-MWFS <0.78 (ie, 78% of predicted that corresponded to the 5th centile in the control population) and sc-FS <0.80 were considered indicative of depressed LV performance.23
Vascular function analysis
Total afterload was determined by estimated arterial elastance (Ea=0.9 ×SBP/SV).15 Total arterial compliance was estimated by the SV-to-pulse-pressure ratio and systemic vascular resistance index by mean brachial cuff pressure (diastolic blood pressure + (pulse pressure/3)) divided by cardiac index × 80.24 The ventricular–arterial interaction was assessed by the coupling ratio (Ea/Ees).
Statistical analysis
Sample size was estimated from a pilot study and previously published data. For Ees for an expected mean difference of 0.7 and SD 0.8 a sample size of 50 would provide 99% power with α=0.05. Statistical analysis was performed using SPSS version 13.0. Continuous variables were expressed as mean±SD and nominal variables as percentages. Continuous variables were compared by analysis of covariance with post hoc Fisher's least significant difference test between normal controls and disease subgroups, adjusted for age and sex. The p values after adjustment are presented. Categorical variables were compared between study groups by the χ2 test. Intra- and interobserver variability was calculated as the mean percentage error, defined as the absolute difference between the two sets of measurements divided by the mean of the measurements, using readings from 10 randomly selected patients. In our previous study, intra- and interobserver variability was 8.2% and 9.8% for torsion, 5.9% and 9.4% for mean global systolic circumferential strain, 6.1% and 8.1% for mean global radial strain and 2.3% and 3.1% for mean global longitudinal strain, respectively.19 Two-sided values of p<0.05 were considered statistically significant.
Results
Subject characteristics
A total of 389 consecutive subjects were screened with 42 (11%) excluded where speckle tracking could not reliably be measured. The remaining 347 subjects (287 patients and 60 control subjects) had adequate echocardiographic images for interpretation. Patients with HFNEF were older with more women, and had higher systolic blood pressure than HFREF or control groups. Both heart failure groups had comparable prevalence of hypertension, diabetes, hyperlipidaemia, New York Heart Association (NYHA) classes, BSA as well as body mass index but coronary artery disease (CAD) was more prevalent in the patients with HFREF (p<0.01, table 1). Patients with HFNEF had more impaired relaxation than HFREF and control subjects. In patients with HFNEF, 41% had pseudonormal and 17% had a restrictive LV filling pattern, whereas roughly one-third of those with HFREF had either grading of the diastolic dysfunction (p<0.001). The BNP levels were higher in the HFREF than the HFNEF group with considerable scatter in both populations.
Subject characteristics
LV geometry
After adjustment for age and gender, both control and HFNEF groups had a similar LVEDV index, SV and cardiac index but patients with HFREF had significantly more dilated left ventricles and reduced SV and cardiac index. Both heart failure groups had a greater LV mass index and ratio of LV mass to volume than the control (both p<0.001), with the highest mass index in the HFREF group and greatest mass:volume ratio in the HFNEF group. After adjustment for age and gender, relative wall thickness was increased in HFNEF but decreased in HFREF compared with the control subjects. The percentage LV hypertrophy was greatest in HFREF followed by HFNEF and the control group (table 2).
Left ventricular geometry and cardiovascular function
Ventricular-arterial stiffness and coupling
With adjustment for age, gender and BSA, where appropriate, both disease groups showed increased afterload (Ea and SVRI), LV end-systolic wall stress and decreased total arterial compliance compared with control subjects (all p<0.001). Ees was increased in HFNEF but reduced in HFREF compared with control group (both p<0.001), even after correction for their LV mass or volume. However, when normalising to the LV mass/EDV ratio (Ees divided by LV mass/volume ratio), there was progressive decrease of the corrected Ees from controls (2.9±0.8 mm Hg/g) to HFNEF (2.2±0.9) followed by HFREF (0.8±0.3; all p<0.001). The coupling ratio (Ea/Ees) was similar between control and HFNEF groups but was significantly higher in the HFREF than the control group (p<0.001). The LV work efficiency was significantly decreased with higher Ea/Ees and lower stroke work index in HFREF than in HFNEF and control groups (both p<0.001, table 2).
LV diastolic function
Both heart failure groups had comparable numbers with pseudonormal LV filling. e′ was significantly reduced and the estimated LVEDP (septal E/e′) was markedly raised to a similar level in both HFNEF and HFREF groups compared with normal controls.
Load-independent LV contractility
After adjusting for age, gender and BSA, there was progressive increase of both circumferential and meridional end-systolic wall stresses with progressive decrease of load-independent measure of chamber contractility (PRSW, stress-corrected MWFS or FS) from control subjects, to patients with HFNEF to patients with HFREF (all p<0.001) (table 3). A total of 7% and 64% of patients with HFNEF and HFREF had stress-corrected FS <80% of predicted respectively (all p<0.001), whereas 34% and 82% of patients with HFNEF and HFREF had stress-corrected MWFS <78% predicted respectively (all p<0.001) (table 3). Patients with HFNEF with or without CAD had similar PRSW, stress-corrected MWFS or FS, suggesting that the differences in LV contractility between controls and HFNEF could not be attributed solely to the presence of CAD.
Left ventricular load and load-independent measures of contractility in all subgroups
Global two-dimensional strains and torsion
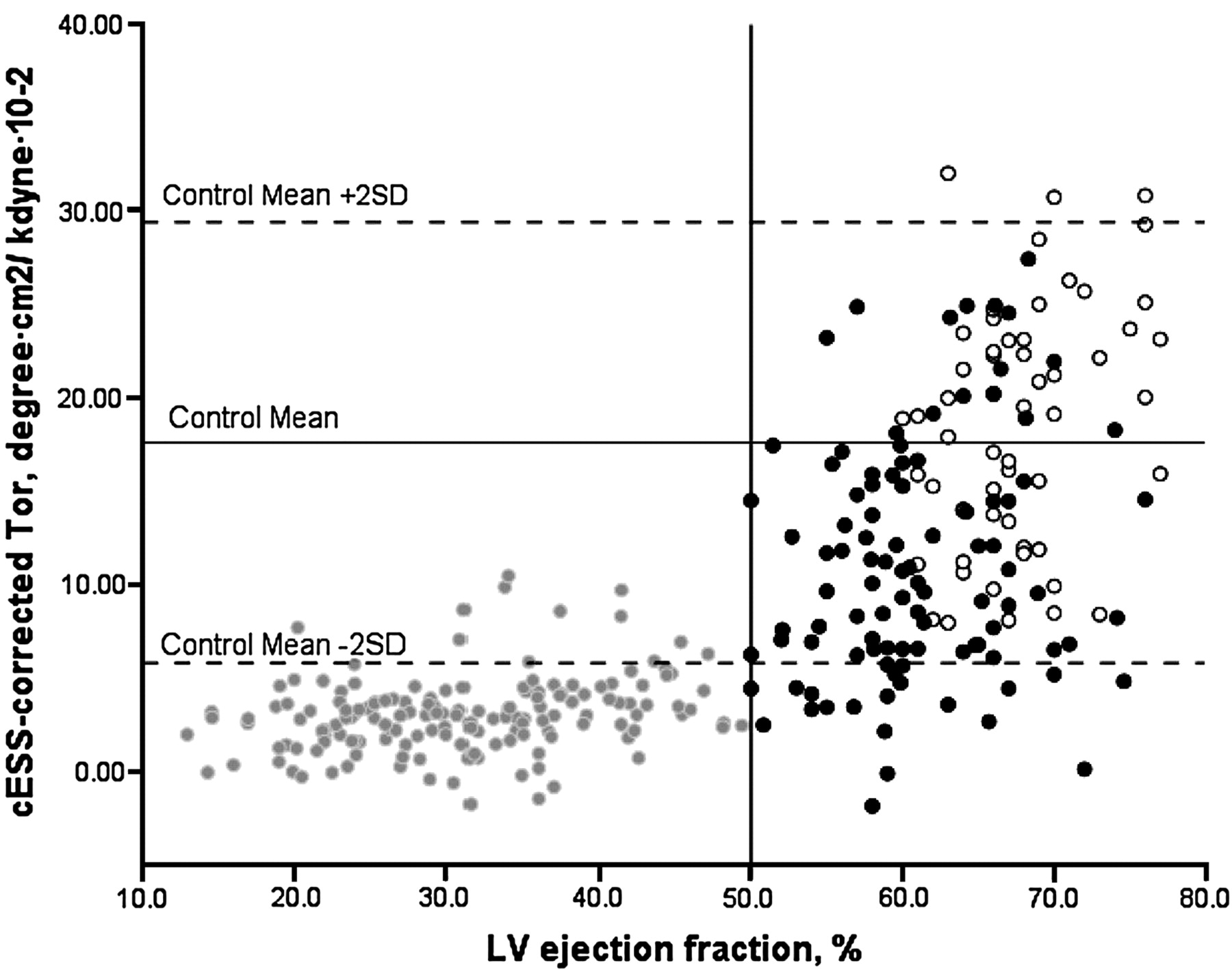
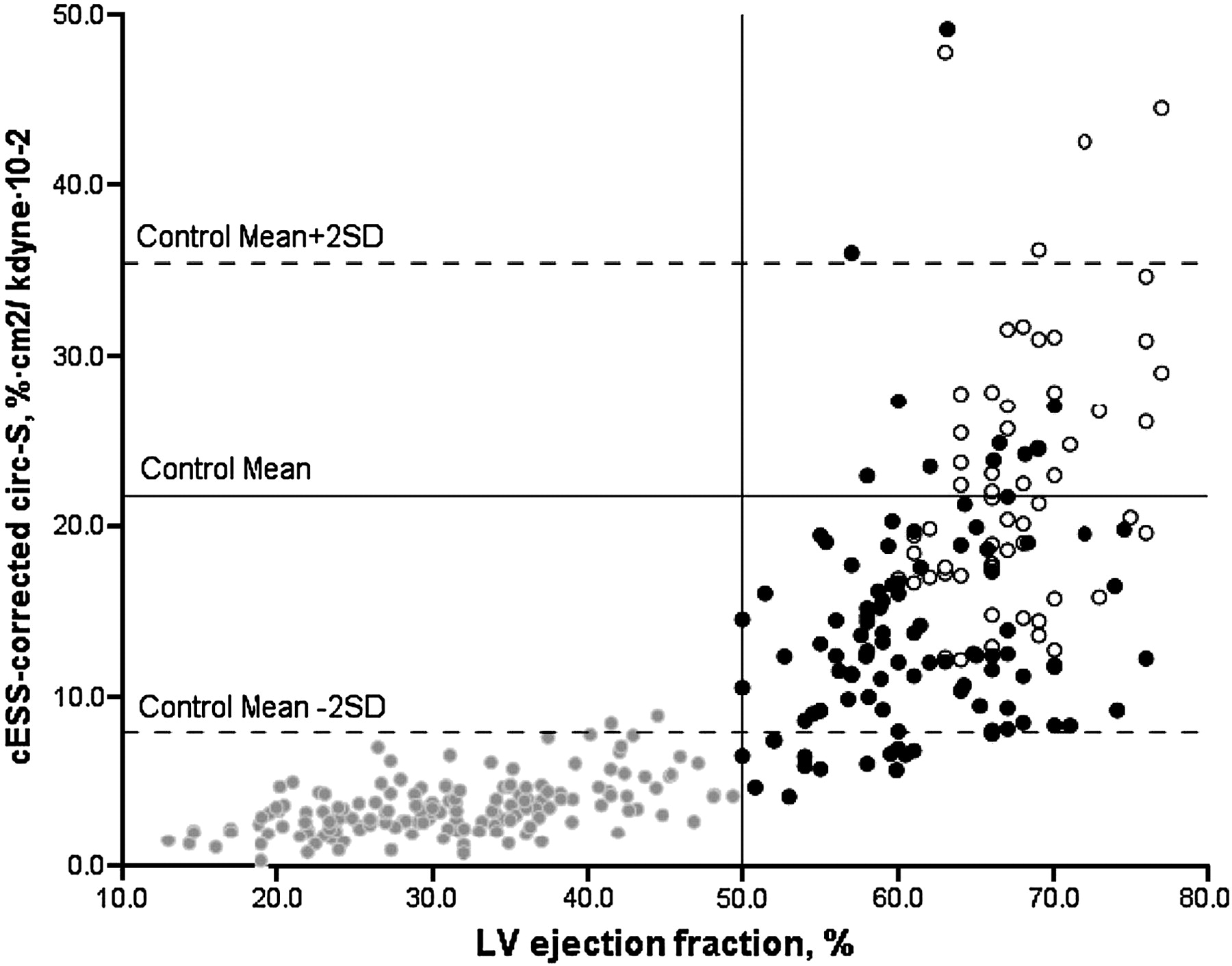
In adjusted comparisons for age, gender and BSA, there was progressive decrease of global 2D circumferential, radial and longitudinal strain as well as torsion from normal, HFNEF to HFREF groups, even after adjustment for end-systolic wall stress or EDV (all p<0.01, table 3). Of note, patients with HFNEF with or without CAD displayed similar aforementioned findings (all p<0.001 vs controls) but with no difference between the two subgroups (p=NS, table 4). In the patients with HFNEF, about 14%, 12%, 37%, and 20% of cESS-corrected global circumferential, radial, longitudinal 2D strain and torsion were below the 5th centile of the normal controls, respectively. About 50% of patients with HFNEF had at least one global strain or torsion parameter depressed, and below the 5th centile. More importantly, >85% of these patients fell below the normal stress-corrected mean values for their corresponding global 2D strains and torsion (figure 1–4).
Ventricular–arterial coupling and load-independent measures of left ventricular contractility in the subgroup of patients with heart failure and normal ejection fraction and controls

The relationship between global circumferential strain (circ-strain, %·cm2/ kdyne·10−2) corrected for circumferential end-systolic wall stress (cESS) and left ventricular ejection fraction (LVEF,%) showing mean (solid line) and 2 standard deviation limits (dashed lines) in control subjects (open black dots) with data points for heart failure patients with normal ejection fraction (HFNEF, solid black dots) and those with reduced ejection fraction (HFREF, grey dots).

The relationship between global radial strain (rad-strain, %·cm2/ kdyne·10−2) corrected for circumferential end-systolic wall stress (cESS) and left ventricular ejection fraction (LVEF,%) showing mean (solid line) and 2 standard deviation limits (dashed lines) in control subjects (open black dots) with data points for heart failure patients with normal ejection fraction (HFNEF, solid black dots) and those with reduced ejection fraction (HFREF, grey dots).
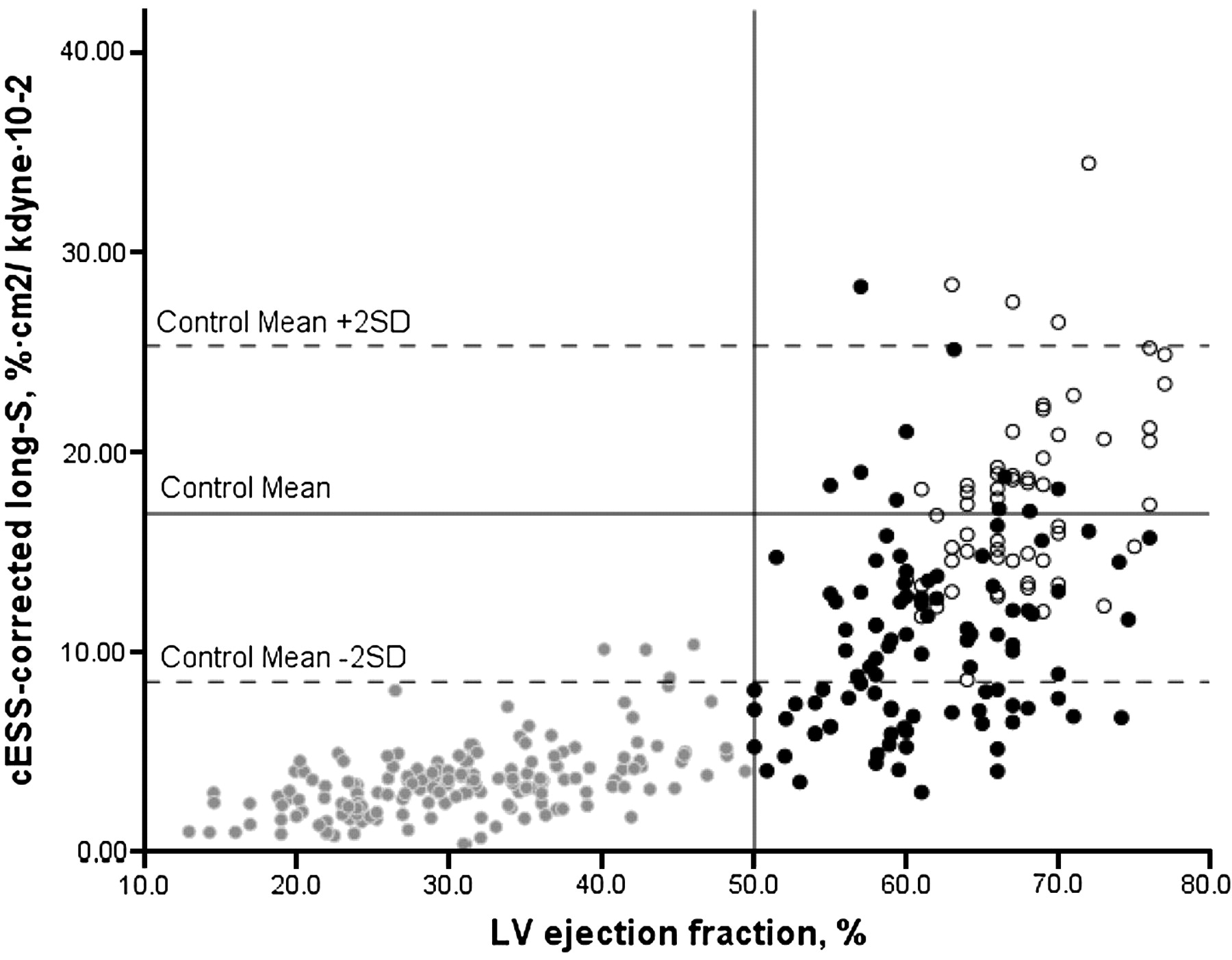
The relationship between global longitudinal strain (long-strain, %·cm2/ kdyne·10−2) corrected for circumferential end-systolic wall stress (cESS) and left ventricular ejection fraction (LVEF,%) showing mean (solid line) and 2 standard deviation limits (dashed lines) in control subjects (open black dots) with data points for heart failure patients with normal ejection fraction (HFNEF, solid black dots) and those with reduced ejection fraction (HFREF, grey dots).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The relationship between global torsion (tor, degree) corrected for circumferential end-systolic wall stress (cESS) and left ventricular ejection fraction (LVEF,%) showing mean (solid line) and 2 standard deviation limits (dashed lines) in control subjects (open black dots) with data points for heart failure patients with normal ejection fraction (HFNEF, solid black dots) and those with reduced ejection fraction (HFREF, grey dots).
Discussion
In this study, we have performed a comprehensive evaluation of resting systolic and diastolic ventricular function in consecutive patients with HFNEF and HFREF using traditional and newer echocardiographic parameters normalised for both preload and afterload and for remodelling (both volume and mass), and we have demonstrated a variety of abnormalities of both systolic and diastolic function in HFNEF. These include impaired load-independent LV contractility (LV elastance (Ees) normalised to LV mass/volume ratio, PRSW, stress-corrected FS or MWFS), preserved ventricular–arterial coupling ratio at the expense of both increased LV systolic stiffness Ees and effective arterial elastance (Ea), and impairment of global LV longitudinal, radial and circumferential strain and torsion with or without correction by LV volume and end-systolic wall stress. Recent work has demonstrated that abnormalities exist in LV systolic properties, ventricular–arterial coupling, LV diastolic function, torsion or twist, ventricular–ventricular interaction, atrial dysfunction, pericardial constraint, with impaired chronotropic, vasodilator reserves and pulmonary hypertension.25 Our study confirms and extends some of these previous findings and, in particular, our results are in agreement with the two recent publications by Tan et al9 and Borlaug et al.10 A more comprehensive picture of the combination of systolic and diastolic abnormalities in HFENF is now available as a result of these studies and ours.
Patient characteristics and LV morphology
In previous studies, mainly hypertensive patients with HFNEF were enrolled with variable degrees of CAD (up to 56%) and diabetes mellitus (up to 37%).8 10 14 26–33 Our cohort reflects the local prevalence of disease patterns in Hong Kong, in that 32% of patients with HFNEF had CAD, 8% had previous myocardial infarction, 63% and 45% had hypertension and diabetes mellitus, respectively. While the prevalence of CAD in HFNEF has remained almost the same in Hong Kong during the past 10 years,34 diabetes mellitus is rising in Southeast Asia. HFNEF is therefore a heterogeneous condition owing to its underlying pathophysiology and also the associated disease conditions relating to geographical and race-specific differences. Age, diabetes and hypertension are all associated with abnormalities of the microvasculature, which lead to reduced coronary flow reserve and this may be part of the underlying mechanism and explain the high mortality in HFNEF.35 However, the differences in aetiology between HFNEF (mainly hypertension) and HFREF (primarily acute myocardial infarction and CAD) may explain the different pattern and progression of these two phenotypes of HF. Myocardial infarction appears to be a powerful stimulus for fibrosis and ventricular enlargement, whereas such remodelling is slow in hypertensive heart disease. This may explain the lack of mortality benefit in reverse-remodelling treatment in patients with HFNEF.1 25 Our results on LV volumes in HFNEF were consistent with previous population-based studies that demonstrated patients that patients with HFNEF had either decreased or normal LV volumes compared with healthy or hypertensive control subjects.10 26 27 31 In contrast, a small subgroup of 35 hypertensive patients with HFNEF with renal impairment in the Cardiovascular Health Study had larger LV volumes but normal systolic ventricular and vascular stiffness. This may explain the enhanced sensitivity to fluid overload from increased LV remodelling and dilatation with volume-dependent elevation of filling pressures.29 33
LV systolic performance
Similar to recent studies, our mean values of the stroke work index (SW/EDV) and Ees appeared higher in HFNEF than in controls.10 14 26 This may not necessarily represent increased contractility in HFNEF as SW/EDV could be load dependent and, more importantly, normalisation of the Ees by the ratio of LV mass to volume led to lower value than for controls with increased LV systolic stiffness.
Load, LV contractility and ventricular–arterial coupling
Our findings on patients with HFNEF were entirely consistent with those of Borlaug et al, who demonstrated that hypertensive patients with or without HFNEF had similarly increased arterial load, LV systolic stiffness and preserved ventricular–arterial coupling ratio (LV work efficiency) but only patients with HFNEF had depressed load-independent LV contractility (PRSW, stress-corrected FS and MWFS).10 This indicates that hypertensive heart disease progresses to HFNEF because of processes that impair LV contractility and increase systolic stiffness. Our study showed that about one-third of patients with HFNEF were below the 5th centile in the control population for the stress-corrected MWFS and 7% for the stress-corrected FS. More importantly, the depressed LV contractility in the HFNEF group was unrelated to the presence of CAD in our study.
Global systolic function by 2D strain
Global 2D strain reflects global systolic performance rather than contractility, which is better evaluated by strain rate. Measurement of the latter is limited by adequate temporal resolution of current technology of the 2D speckle tracking. However, these global deformation parameters were corrected for loading conditions in an attempt to provide evidence of LV contractility. Our study demonstrated global impairment of 2D torsion and strain in different directions in HFNEF even after normalising to LVEDV and end-systolic wall stress. Since patients with HFNEF had a similar EDV index to that of controls and a significantly higher estimated LVEDP, it is reasonable to conclude that the preload was not reduced in HFNEF as compared with normal control subjects. Wang et al8 reported that only LV longitudinal and radial strains were reduced in 20 patients with HFNEF, with LVEDV, LVESV, LV mass, torsion, meridional and circumferential end-systolic wall stresses comparable to those of 17 normal controls. In addition, only LVEF and circumferential strain were independent predictors of LV torsion.8 We further adjusted our torsion values for LVEF (SV/EDV) and the results were unchanged. Our results differ from those of Wang et al in that our HFNEF and normal control groups were older (HFNEF: mean age 74±12 vs 63±16; Normal:53±10 vs 42±11). Our HFNEF cohort had more female patients (64% vs 35%) with a lower prevalence of CAD (32% vs 75%), higher LV mass index and end-systolic wall stresses. The presence of CAD did not affect our overall results. Our results on torsion, however, are in agreement with the results of Tan et al,9 who also found reduced apical rotation at rest and more importantly on exercise. It is probable that the cohort studied by Wang et al represents the early stage of HFNEF in which the subendocardial longitudinal fibres are primarily affected so that the counterclockwise apical rotation of subepicardial fibres become unopposed and may increase rotation of the apex. With more advanced fibrosis or damage as seen in a more elderly HFNEF population, torsion will become impaired with global impairment of systolic performance and contractility.
Limitations
The non-invasive methods for assessing systolic and diastolic function have been validated against invasive techniques. Nevertheless, echocardiography-derived parameters have inherently greater variability than their invasively derived counterparts. Our data are cross-sectional in nature and therefore cannot prove causality or temporal progression of HFNEF. All patients in the study were taking medication, because it was considered unethical to stop treatment entirely. It is probable that the effect of treatment would be to improve deformation or strain and rotation as β blockers improve EF in heart failure and there is a suggestion that ACE inhibitors or receptor antagonists might improve longitudinal function in patients with HFENF.36
Conclusions
We have demonstrated that patients with HFNEF have a range of LV systolic and diastolic abnormalities at rest. These include impaired load-independent ventricular contractility, preserved ventricular–arterial coupling ratio at the expense of both increased LV systolic stiffness and effective arterial elastance, and impairment of global LV longitudinal, radial and circumferential strain and torsion with or without correction by LV volume or end-systolic wall stress. Their systolic performance and contractility appeared to be intermediate between the control and HFREF groups. HFNEF is not a disease of diastolic function alone and abnormalities in systolic properties do contribute equally to its pathophysiology.
References
Footnotes
Funding This research was funded by General Research Fund (project #479509) from the Research Grants Council of Hong Kong.
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the Joint The Chinese University of Hong Kong-New Territories East Cluster Clinical Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- PostScript