Article Text

Abstract
Contemporary mechanical reperfusion therapy for acute myocardial infarction is aimed at early and complete restoration of myocardial perfusion. However, successful restoration of epicardial blood flow does not guarantee restoration of flow at the myocardial tissue level. The incidence of inadequate myocardial reperfusion after primary percutaneous coronary intervention (PCI) varies from 15–70%, based upon the diagnostic modality used.
The Doppler flow guidewire can be used immediately after primary PCI to identify patients with apparently restored epicardial flow but impaired reperfusion at the myocardial microcirculatory and tissue level. Characteristic findings by intracoronary Doppler flow velocity measurements such as a reduced coronary flow velocity reserve, and, in particular, systolic flow velocity reversal and a short diastolic deceleration time are associated with the presence of microvascular obstruction.
Detection of microvascular obstruction by the Doppler flow wire directly after primary PCI can identify patients who may benefit from adjunctive therapy after primary PCI.
- Acute myocardial infarction
- Doppler flow wire
- microvascular function
- prognosis
Statistics from Altmetric.com
Introduction
Contemporary mechanical reperfusion therapy in acute coronary syndromes is aimed at early and complete restoration of myocardial perfusion. However, successful restoration of epicardial blood flow does not guarantee restoration of flow at the myocardial tissue level. In about 15–30% of patients, the capillary structure becomes disorganised owing to endothelial swelling, compression by tissue, myocyte oedema and neutrophil infiltration, leading to microvascular obstruction.1 2 This inadequate microvascular perfusion is clinically relevant, as it is associated with larger myocardial infarct size, reduced left ventricular function and a worse clinical outcome than in patients with adequate myocardial reperfusion.3–5
Several diagnostic modalities are currently applied to detect microvascular obstruction. A thrombolysis in myocardial infarction (TIMI) flow grade ≤2 in the absence of macrovascular obstruction is often used as a definition of microvascular obstruction.6 However, even in patients with TIMI flow grade 3, microvascular perfusion can be impaired. The TIMI perfusion grade and the myocardial blush grade are also frequently used to assess myocardial reperfusion using coronary angiography.7 8 Another readily available and widely used marker of tissue-level reperfusion is resolution of ST-segment elevation.9 More accurate, non-invasive imaging modalities such as myocardial contrast echocardiography (MCE) and delayed contrast enhancement using cardiac magnetic resonance imaging (CMR) can also be used to detect microvascular obstruction.4 5 10 11
Moreover, coronary blood flow can be measured invasively by an intracoronary Doppler-tipped guidewire. Since the 1970s, when catheter-based Doppler systems were first introduced by Benchimol and later Hartley and Cole, many improvements have been made to its design.12–14 A typical contemporary Doppler guidewire transmits and receives pulsed-wave ultrasound signals generated by a piezoelectric ultrasound transmitter (figure 1). Characteristic coronary blood flow patterns in patients with coronary microvascular obstruction are systolic flow reversal, rapid deceleration of diastolic flow and a reduced coronary flow velocity reserve (CFVR).11 15
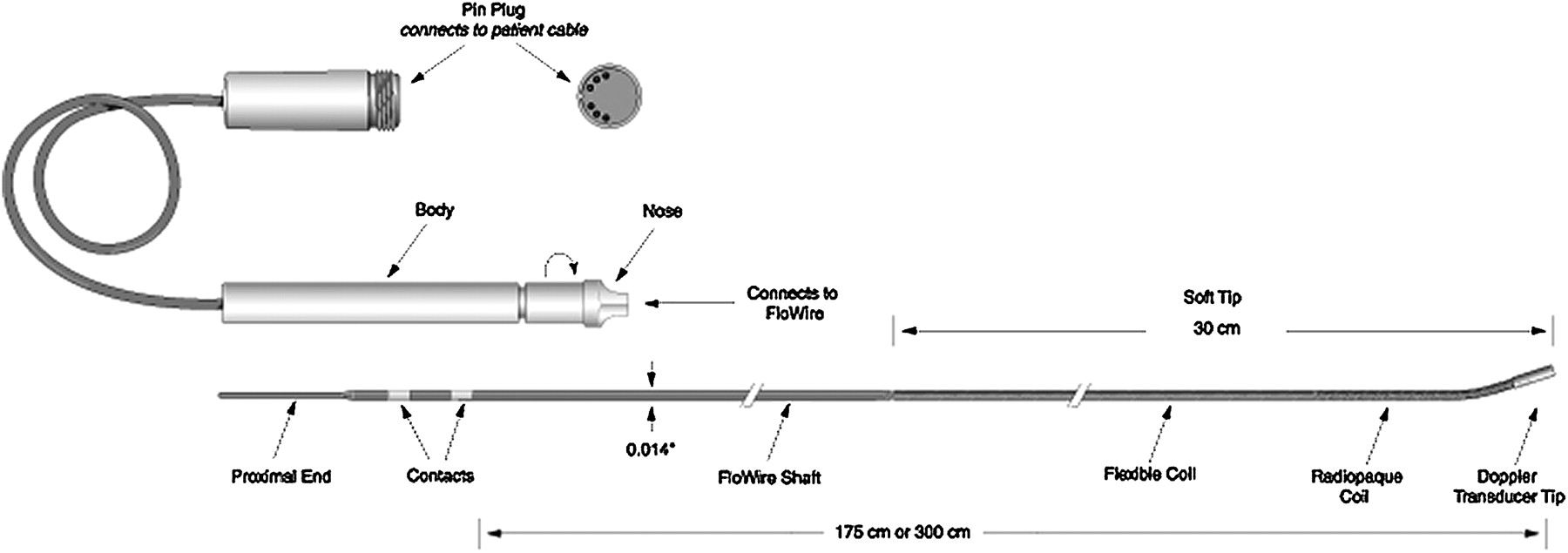
A typical Doppler-tipped guide wire used for instantaneous measurement of intravascular flow velocity.
Coronary flow reserve in acute myocardial infarction
In 1996, Kern et al were the first to study coronary blood flow directly in patients in the setting of acute myocardial infarction (MI) by using a Doppler-tipped guidewire. In 41 patients with an acute MI, coronary blood flow velocity measured in the culprit artery during primary angioplasty by Doppler guidewire was compared with TIMI flow grade.16 In these patients, TIMI flow grades <3 were consistently associated with low baseline coronary blood flow velocity. However, among the 35 patients with post-interventional TIMI flow grade 3, 13 had a low baseline coronary blood flow velocity of <20 cm/s. In the total cohort of 42 patients, 11 patients had a clinical event during a median follow-up period of 18 months; of these events, nine occurred in patients with angiographic TIMI flow grade 3 but a low baseline blood flow velocity in the infarct-related arteries. This study shows that patients with TIMI flow grade 3 after primary percutaneous coronary intervention (PCI) have a wide range of flow velocity patterns and suggests that Doppler flow velocity measurement can further distinguish patients at increased risk for clinical events.
Ishihara et al measured relative CFVR in infarct-related arteries (IRAs) in a series of 14 patients with a first anterior wall acute MI directly after primary angioplasty and at 14 days and 6 months' follow-up.17 Absolute CFVR is calculated as the ratio of hyperaemic to baseline average peak flow velocity. A CFVR of <2.0 is generally considered to be abnormal. Relative CFVR is calculated as the ratio of the absolute CFVR in the IRA to the absolute CFVR in the reference artery. The CFVR measures the functional status of the distal microvascular bed and depends on multiple factors, including myocardial resistance, metabolic demands, neurohumoral activation, filling pressures and vascular resistances of epicardial coronary arteries and distal microvascular bed. Ishihara et al observed an abnormal CFVR in the IRA directly after angioplasty, while CFVR gradually improved at 14 days and 6 months. However, even at 6 months, CFVR in the IRAs was still impaired (mean CFVR 2.34±0.38) in comparison with angiographically normal coronary arteries in reference patients (mean CFVR 3.13±0.48).
A similar experiment was conducted in a larger cohort by Bax et al, who measured CFVR in both IRAs and non-IRAs immediately after the primary angioplasty in 73 patients with a first anterior MI, at 1 week and at 6 months.18 Figure 2 shows CFVR, and baseline and hyperaemic average peak flow velocity in IRAs and non-IRAs. Immediately after primary PCI, CFVR was reduced in both IRAs and non-IRAs, although more pronounced in IRAs. At 1 week, CFVR was still impaired in IRAs, but in non-IRAs CFVR had almost returned to normal. Unlike the findings by Ishihara et al, CFVR was found to be normalised in IRAs at 6 months. This discrepancy can possibly be explained by the fact that all patients in the Japanese cohort were treated with balloon angioplasty alone, rather than coronary stenting. Furthermore, the Japanese study was hampered by small sample size (n=14). The reduced CFVR was mainly due to a decreased hyperaemic blood flow velocity. The explanation for decreased hyperaemic blood flow velocity during the acute phase of MI is multifactorial. Neurohumoral responses to ischaemia lead to microvascular vasoconstriction in both IRAs and non-IRAs, and distal (micro-)embolisation in IRAs. Moreover, microvascular damage and endothelium dysfunction as a result of ischaemia and reperfusion lead to disturbed autoregulation. The microvascular resistance index was measured as the ratio of transvascular pressure gradient (mean aortic pressure minus right atrial pressure) to hyperaemic blood flow velocity. The microvascular index was found to be increased during the acute phase of MI, and almost normalised at 1 week. Therefore, this study suggests that reduced CFVR after MI is partly explained by increased microvascular resistance, but to a greater extent by disturbed autoregulation.
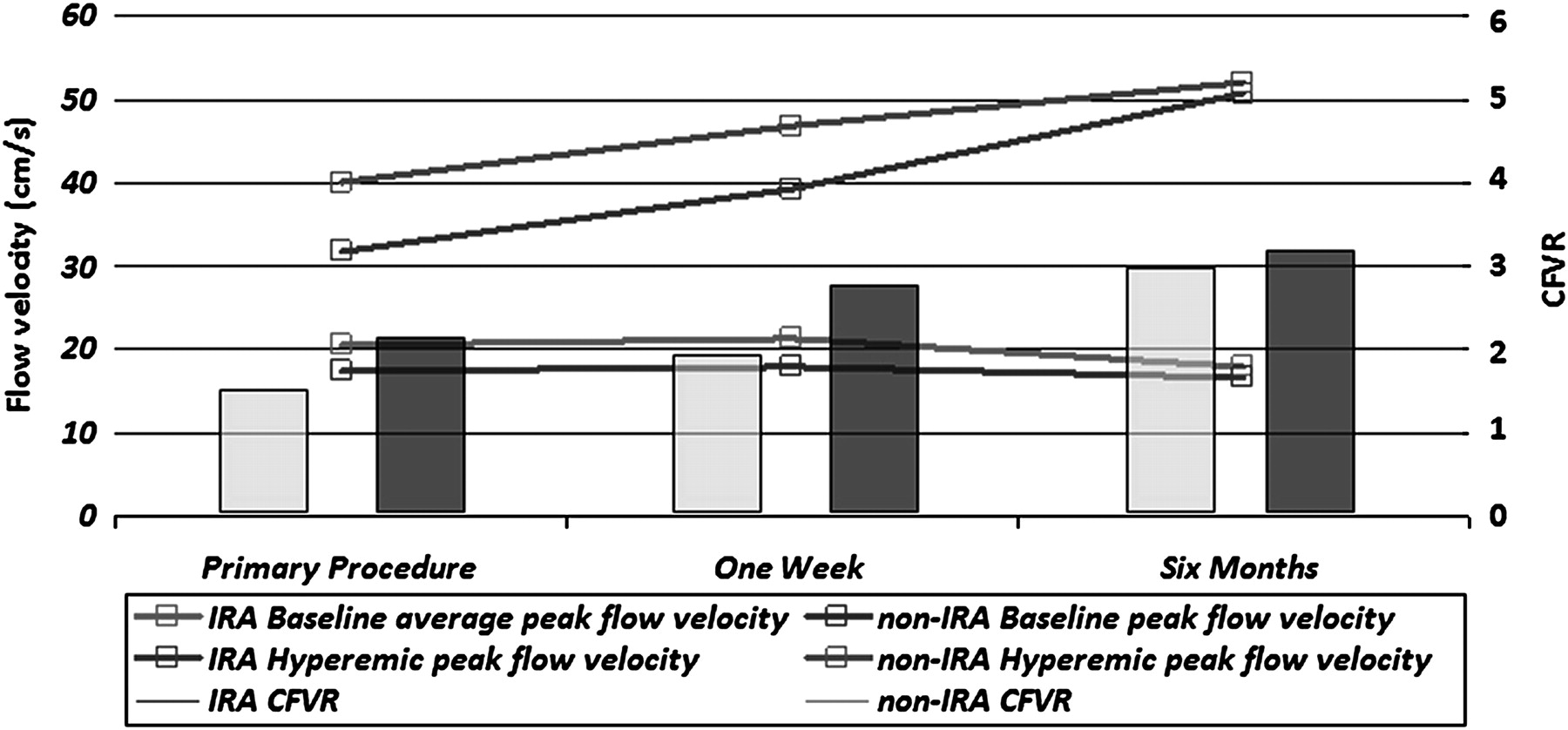
CFVR, Baseline and hyperaemic peak flow velocity in IRAs and non-IRAs immediately after the primary procedure, after 1 week and after 6 months. CFVR, coronary flow velocity reserve; IRA, infarct-related artery.
Systolic flow reversal and rapid deceleration of diastolic flow: characteristic Doppler flow-velocity patterns in microvascular obstruction
Iwakura et al were the first to report characteristic Doppler flow velocity patterns in microvascular obstruction after acute MI.11 They examined the Doppler-flow wire derived coronary blood flow velocity pattern in 42 consecutive patients with acute MI. Additionally, MCE was performed in all patients both before and after primary angioplasty. Microvascular obstruction was detected in 11 patients (26%) by MCE. The coronary flow velocity pattern appeared to be normal in patients without microvascular obstruction on MCE (Figure 3a). However, in patients with microvascular obstruction the coronary blood flow velocity pattern was characterised by the appearance of abnormal retrograde flow in early systole, and rapid deceleration of the diastolic flow velocity (Figure 3b). Early retrograde systolic flow was seen in 10 of 11 patients with signs of no reflow compared with only one patient without signs of no reflow on MCE. The rate of decline in flow velocity in diastole was calculated as the diastolic deceleration rate (cm/s2). Mean diastolic deceleration rate was 106.4±76.1 cm/s2 in the no-reflow group compared with 55.9±31.2 cm/s2 in the reflow group (p<0.01).

{kind=link}
{kind=link}
{kind=link}
(A) The coronary flow velocity spectrum shows antegrade systolic flow without systolic retrograde flow (SRF) and a normal diastolic deceleration time (DDT). (B) The coronary flow velocity spectrum shows SRF and a short DDT.
A short diastolic deceleration time and systolic flow reversal were also studied by Okamura et al in a cohort of 72 patients with first acute anterior MI.19 Microvascular obstruction was measured by MCE directly after primary PCI. Left ventricular ejection fraction and regional wall motion were measured by left ventriculography during the primary angioplasty procedure and again at discharge (24±2 days). Ten minutes after primary PCI, Doppler flow wire measurements were performed.
The principal finding of their study was that with advancing severity of damage in the infarcted myocardium, the diastolic deceleration time shortened first, followed by the appearance of systolic flow reversal and finally, by disappearance of systolic antegrade flow. Microvascular obstruction on MCE was not detected in patients without abnormal coronary flow characteristics on Doppler flow examination. Of the 41 patients with at least one of the aforementioned abnormal Doppler flow characteristics, 28 (68%) had evidence of microvascular obstruction on MCE. Furthermore, these characteristic flow velocity characteristics were associated with reduced recovery of regional wall motion and left ventricular ejection fraction.
It has been suggested that rapid deceleration of diastolic flow is caused by an increase in microvascular impedance and a decrease of intramyocardial blood pool volume. In normal individuals, the intramyocardial capillaries and venules are filled during diastole without an increase in intramural pressure.20 However, owing to capillary obstruction the capacitance of the myocardial microvasculature decreases. This has an impeding effect on diastolic flow, resulting in a rapid decrease in coronary flow velocity. Rapid deceleration of diastolic flow is associated with poorer tissue perfusion, worse functional outcome, left ventricular remodelling and an increased rate of adverse cardiac events.21
However, rapid deceleration of diastolic flow also occurs in patients without signs of microvascular obstruction measured by MCE or CMR. Therefore, rapid deceleration of diastolic flow alone has a high sensitivity, but a relatively low specificity for detecting microvascular obstruction.
Systolic flow reversal is another accurate marker of microvascular obstruction. The increased microvascular impedance resulting from microvascular injury hampers the heart's ability to squeeze blood forward into the venous system during systole, and consequently, blood will be squeezed back into the arterial system, resulting in systolic flow reversal. In the most severe case of microvascular obstruction, a high back pressure persists throughout systole, resulting in total disappearance of systolic antegrade flow.
Doppler flow wire as a tool to predict recovery of left ventricular recovery after acute MI
Kawamoto et al investigated the clinical value of the Doppler flow guidewire-derived coronary flow pattern in predicting left ventricular function in 23 patients with a first anterior acute MI.21 The coronary flow pattern was recorded immediately after the primary angioplasty and left ventricular function was assessed before recanalisation and at 1-month follow-up by echocardiographic anterior wall motion score index. In this study, a short diastolic deceleration time (<600 ms) and low average systolic peak velocity (<6.5 cm/s) were associated with a lack of recovery of regional left ventricular function.
Bax et al compared the predictive value of CFVR with TIMI flow grade, corrected TIMI frame count, myocardial blush grade and resolution of ST-segment elevation for recovery of left ventricular function in the aforementioned series of 73 patients with a first anterior MI treated with primary PCI.22 Two-dimensional echocardiography was performed immediately before the primary PCI and repeated after 1 day, 1 week and 6 months. After multivariate linear regression analysis, CFVR as measured by the Doppler flow guidewire in comparison with the aforementioned, commonly reported angiographic and clinical parameters, was better in predicting recovery of left ventricular function. All patients with a CFVR>2.0 directly after primary PCI showed improved left ventricular function (measured as echocardiographic 16-segment wall motion index) at 6 months' follow-up. Doppler-derived CFVR was independently correlated with recovery of global and regional left ventricular function. No independent relation was found between angiographic parameters or ST-segment resolution and recovery of left ventricular function. Recovery of left ventricular function after acute MI can be accurately predicted by intracoronary Doppler flow velocity measurement during primary PCI.
Comparison of Doppler flow velocity measurement and contrast-enhanced CMR
The assessment of microvascular injury by coronary Doppler flow velocity measurement has been found to correspond well to evaluation by contrast-enhanced CMR. A series of 27 consecutive patients with a first anterior MI underwent CMR and repeat catheterisation for intracoronary flow measurement within 1 week in a study by Hirsch et al.10 All patients had a postprocedural TIMI flow grade 3. However, CMR showed microvascular obstruction in 19 patients (70%). Based on the extent of microvascular obstruction detected by contrast-enhanced CMR, patients were subsequently stratified as having mild or severe microvascular obstruction. Systolic flow reversal was seen in none of eight patients without microvascular obstruction, in four of 10 (40%) patients with mild microvascular obstruction and in six of nine patients (67%) with severe microvascular obstruction. In accordance with previous studies, the diastolic deceleration time was reduced in patients with mild (mean 575 ms) and severe (mean 382 ms) microvascular obstruction in comparison with patients without microvascular obstruction (mean 708 ms). The extent of microvascular obstruction seen by CMR was independently correlated with systolic flow reversal, a short diastolic deceleration time, and low CFVR of the IRA.
Limitations of the Doppler flow wire and alternative invasive techniques to assess microvascular injury
A few limitations of the Doppler flow wire should be mentioned. Although there is fair reproducibility of CFVR, it is dependent upon a number of haemodynamic conditions such as arterial pressure and heart rate.23–25 The haemodynamic dependence of CFVR is mainly because resting coronary flow velocity is very sensitive to changes in myocardial oxygen consumption. Furthermore, as the extent of microvascular obstruction is known to increase within the days after primary PCI, single Doppler flow velocity measurements immediately after primary PCI might underestimate the degree of microvascular obstruction subsequently present. Another limitation is the difficulty of detecting an adequate flow signal. A novel guidewire tipped with both a Doppler flow and a pressure sensor has made signal acquisition more cumbersome. A possible explanation might be the change in display from an analogue signal to a digital signal. Based upon our own experience, reversing the tip of the guidewire to make the sensors face the proximal part of the coronary artery may improve signal quality.
The Doppler flow wire interrogates the resistance of the entire vessel and may not differentiate diffuse epicardial disease or residual epicardial stenosis from microvascular obstruction. Combined pressure–flow velocity measurements are better suited for distinguishing between epicardial and microvascular resistance. Fearon et al reported the index of microcirculatory resistance, measured by a pressure sensor-tipped guidewire in combination with flow using thermodilution to be an independent predictor of recovery of echocardiographic left ventricular wall motion score in 29 patients after acute MI.26 Currently, assessment of microvascular injury by this index has not been compared with the ‘gold standard’ for detection of microvascular obstruction using contrast-enhanced CMR.
The introduction of the dual-sensor (Doppler velocity and pressure) tipped guidewire led to the introduction of physiological indices based upon combined pressure and flow measurements. These novel indices—most notably, hyperaemic microvascular resistance and hyperaemic stenosis resistance, have not yet been tested in the setting of acute MI.27
Another potential modality to assess microvascular injury is wave intensity analysis (WIA). On the basis of measurements of coronary arterial pressure and velocity, WIA allows for a better understanding of aortic, left ventricular and microcirculatory interactions in the coronary circulation. Although promising, WIA has not yet been tested in the setting of acute MI.28
Summary
Microvascular obstruction after acute MI has been associated with ventricular arrhythmias, adverse ventricular remodelling and poor clinical prognosis.4 5 10 Based upon coronary angiography, the incidence of inadequate myocardial reperfusion or a no-reflow phenomenon was approximately 15%.8 The results of non-invasive diagnostic techniques such as MCE and contrast-enhanced CMR yielded a higher incidence rate of up to 70% with CMR.4 5 10 Characteristic findings by intracoronary Doppler flow velocity measurements such as a reduced CFVR secondary to an impaired hyperaemic blood flow velocity, and, in particular, systolic flow velocity reversal and a short diastolic deceleration time, are associated with the presence of microvascular obstruction on MCE and contrast-enhanced CMR. An abnormal CFVR is strongly associated with reduced recovery of left ventricular function after MI.19 22
In primary PCI, the Doppler flow guidewire identifies patients with apparently restored epicardial flow but impaired reperfusion at the myocardial microcirculatory and tissue level. Such patients may benefit from adjunctive treatments such as intracoronary administration of streptokinase, which was recently found to have beneficial effects on infarct size, left ventricular volumes and left ventricular ejection fraction.29
References
Footnotes
Competing interests The authors report no conflicts of interest.
Provenance and peer review Not commissioned; externally peer reviewed.