Article Text

Abstract
Objective: To determine the effect of a new CHOICE (Choice of Health Options In prevention of Cardiovascular Events) programme on cardiovascular risk factors in acute coronary syndrome (ACS) survivors.
Design: Single-blind randomised controlled trial.
Setting: Tertiary referral hospital in Sydney Australia.
Patients: 144 ACS survivors who were not accessing standard cardiac rehabilitation. Data were also collected on a further 64 ACS survivors attending standard cardiac rehabilitation.
Intervention: The CHOICE group (n = 72) participated in a brief, patient-centred, modular programme comprising a clinic visit plus telephone support, encompassing mandatory cholesterol lowering and tailored preferential risk modification. The control group (n = 72) participated in continuing conventional care but no centrally coordinated secondary prevention.
Main outcome measures: Values for total cholesterol, systolic blood pressure, smoking status and physical activity.
Results: CHOICE and control groups were well matched at baseline. At 12 months, the CHOICE group (n = 67) had significantly better risk factor levels than controls (n = 69) for total cholesterol (TC) (mean (SEM) 4.0 (0.1) vs 4.7 (0.1) mmol/l, p<0.001), systolic blood pressure (131.6 (1.8) vs 143.9 (2.3) mm Hg, p<0.001), body mass index (28.9 (0.7) vs 31.2 (0.7) kg/m2, p = 0.025) and physical activity (1369.1 (167.2) vs 715.1 (103.5) METS/kg/min, p = 0.001) as well as a better knowledge of risk factor targets. Also at 1 year, fewer CHOICE participants (21%) had three or more risk factors above widely recommended levels then controls (72%) (p<0.001).
Conclusions: Participation in a brief CHOICE programme significantly improved the modifiable risk profiles and risk factor knowledge of ACS survivors over 12 months. CHOICE is an effective alternative for dealing with the widespread underuse of existing secondary prevention programmes.
Trial registration number: ISRCTN42984084
Statistics from Altmetric.com
Providing acute coronary syndrome (ACS) survivors with active choice about their secondary prevention uniquely addresses the substantial international underuse of cardiac rehabilitation.1 2 Despite widespread recommendations3–5 that all ACS survivors participate in secondary prevention, only a minority attend existing rehabilitation programmes.1 2 Therefore, secondary prevention opportunities for extending survival, reducing cardiovascular events, decreasing revascularisation rates and enhancing quality of life (QoL)6 7 are often lost. Further and more disconcertingly, non-attendees are less likely to believe that rehabilitation is necessary,8 yet have higher baseline risk and poorer risk factor knowledge than those accessing rehabilitation.9 Very few studies have investigated alternative secondary prevention programmes that specifically target the majority of patients not accessing cardiac rehabilitation.
By 2010, it is estimated that cardiovascular disease will be the leading cause of death in developing countries and an estimated one in five Europeans will die before the age of 75 as a result of coronary heart disease (CHD).10 Given that about half the recent reduction in CHD deaths11 may be attributable to reductions in risk factors, it is imperative that innovative and cost-effective secondary prevention programmes are developed and tested. We therefore designed a brief, patient-centred intervention for ACS survivors not participating in rehabilitation. Cognitive-behavioural publications indicate that enhancing patient engagement in decision-making positively affects disease management, outcomes and psychosocial function.12 Offering patients choice and actively involving them in treatment decisions about their healthcare can lead to more appropriate and cost effective use of health services and confer better health outcomes.13 Concomitantly, setting mutually agreed achievable goals and allowing personal choice enhances relevance and independence to change behaviour.14 Also, patient-mediated interventions have been found to be effective in changing clinical practice, particularly the reminding of clinicians by patients about their risk management strategies.15 Further, making multiple concurrent changes to a patient’s behaviour may be counterproductive and step-by-step risk factor management may be more effective.
Implementation of individualised modular secondary prevention programmes has been proposed to close the evidence-practice gap.16 A dynamic and tailored programme with specific clinical modules has been suggested16 and may be readily adapted into clinical practice. We have previously reported significant improvements in risk factors at 3 months, following participation in a modular programme compared with controls, which are similar to those achieved with standard rehabilitation.17 However, while short-term changes are of interest, it is important to establish whether the benefits are maintained. This study aimed to determine the 1-year outcomes of change in modifiable risk factors and related knowledge in patients participating in a new CHOICE (Choice of Health Options In prevention of Cardiovascular Events) programme, compared with a randomised control group receiving usual care, and a contemporary reference group participating in rehabilitation.
METHODS
Study design
The study was a single-blind randomised controlled clinical trial of 208 ACS survivors with 12-months’ follow-up. Appropriate ethical approval was obtained for the study and it was conducted at a tertiary referral hospital in Sydney, Australia between September 2004 and May 2006. The design and methods have been described elsewhere.18 Patients not accessing rehabilitation were randomly allocated to either the control or CHOICE intervention groups. Both groups received medical treatment, including pharmacotherapy and lifestyle counselling, as determined by their usual doctors. The intervention group also participated in the 3-month CHOICE programme for continuing secondary prevention. A third contemporary, non-randomised reference group starting outpatient cardiac rehabilitation was also recruited. Rehabilitation included two 60 min gym sessions and a 2 h education session weekly for 6 weeks.
Participants and randomisation
We identified potential participants from consecutive hospital ACS admissions over 10 months using relevant diagnostic related codes. Reasons for ineligibility have been described previously18 and include living outside a 20 km radius of the hospital, insufficient English to provide informed consent, diagnosed congestive heart failure, the presence of a severe comorbidity and death. For randomisation, a computer-generated random allocation sequence was constructed by an independent research group and was implemented by a researcher using consecutively numbered envelopes. Randomisation took place at a mean (SEM) of 6.2 (0.3) months after index ACS admission in order to maximise numbers available for recruitment.
CHOICE intervention
The CHOICE intervention included a 1 h initial consultation and multiple follow-up phone calls over 3 months.18 The CHOICE programme was designed as a patient-mediated intervention, and development was based on behavioural research indicating that actively engaging patients in treatment decisions and giving choices improves health outcomes.12 15 The programme allowed patients to choose from a range of locally available risk factor modification interventions that included medically directed strategies and self-management options according to their personal preference and circumstances.
The programme has four stages and was designed as an individualised, structured, case-management approach and was overseen by treating doctors. Stage 1 involved the development of modules and tailoring of leaflets, initially by thorough investigation of local programmes for each risk factor. Available programmes and resources were then summarised into patient information leaflets for each risk factor. Stage 2 involved face-to-face risk factor assessment and measurement, generating a list of each patient’s relevant risk factors. In stage 3, the patients made guided choices about which risk factors they would lower, participated in goal-setting informed by current national targets for the chosen risk factors, selected which management option(s) they would use to lower risk and were provided with a tailored resource package that had been previously developed and tested in consultation with consumers.19 Stage 4 comprised telephone follow-up over 3 months, during which each patient’s risk factor(s) goals and strategies were re-evaluated and mutually changed if necessary to enhance success. If goals had been achieved, patients also had the opportunity to add another module they had previously not elected to undertake. All patients were strongly encouraged to communicate openly about their goals and interventions with their family doctor and cardiologist who were made aware of their action plan.
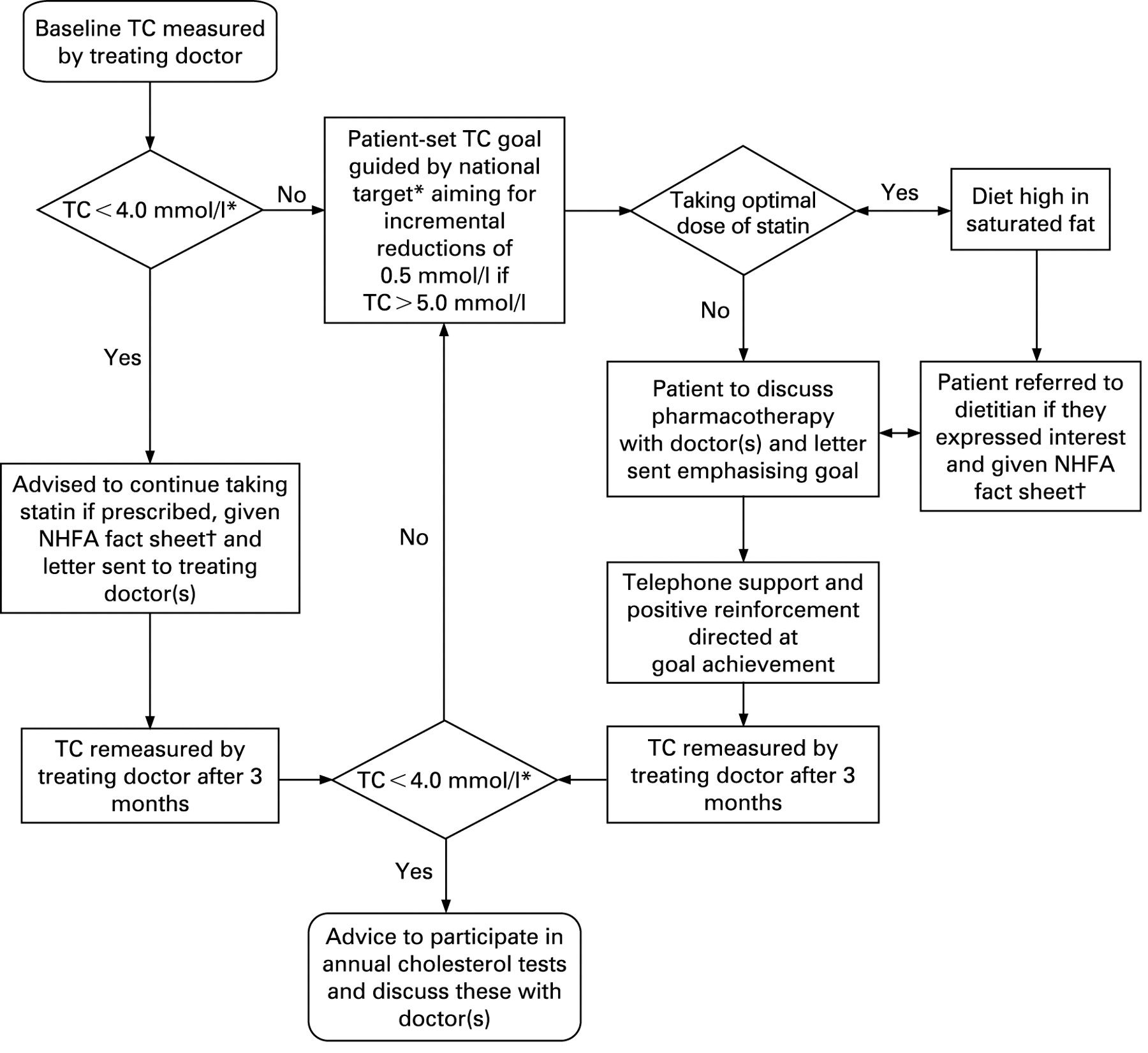
All CHOICE patients participated in a core module for lowering cholesterol (including healthy eating advice and pharmacotherapy), given its major impact on reducing recurrent events.20 The core cholesterol-lowering module (fig 1) involved a stepwise process of initial (more than 6 weeks after ACS) and 2–3-monthly blood cholesterol tests, as arranged by their treating doctor, until their goal (based on the nationally recommended target) or a satisfactory and stable response was achieved.
Up to two choice modules, including blood pressure (BP) lowering, smoking cessation and increased physical activity were also offered. After choosing relevant risk factor modules, patients selected their preferred management option(s). These were broadly summarised as doctor-directed (eg, physical activity “script” from the family doctor), hospital programme (eg, hospital-based group exercise programme), individual programme (eg, home activity programme) or self-help (eg, devising and managing their own activity programme).
Outcomes and follow-up
The primary outcome measures were fasting total cholesterol (TC) level using standardised procedures, resting systolic BP (SBP) measured according to published guidelines using an Omron automatic sphygmomanometer, smoking status by self-report confirmed with an Airmet Scientific Micro-smokerlyzer and physical activity using the 7-day international Physical Activity Recall Questionnaire21 (METS/kg/min) at 12 months.
Secondary outcomes were the prevalence of coronary risk factors, global risk, drug use, QoL and depressed mood using the cardiac depression scale (CDS).22 Cut-off points for determining the prevalence of risk factors were based on the prevailing Australian guidelines defined as TC >4 mmol/l, low-density lipoprotein (LDL) cholesterol >2.5 mmol/l, SBP ⩾140 mm Hg, current smoking, physical inactivity (<150 min/week), body mass index (BMI) ⩾30 kg/m2, documented diabetes and a CDS score ⩾100 for depression.22 We calculated global risk of a future cardiac event using the LIPID risk score (for secondary prevention) that classifies patients as low (score⩽4), medium (5–6), high (7–9) or very high risk (⩾10).23 QoL was assessed using the Short Form-36 (SF-36) version 2.24
Other secondary outcomes were participant’s knowledge of their own risk factors and their frequency of medical consultations. To assess knowledge, participants were asked if they could state any of their own predisposing factors and if they knew the national targets for TC, BP, physical activity and smoking. To investigate the frequency of medical consultations during follow-up we surveyed each participant’s family doctor (77% response rate) and cardiologist (79% response rate).
Statistical analysis
Assuming a 10% loss to follow-up we estimated 72 patients for each group were required to provide 80% power to detect a 0.5 mmol/l reduction in TC, based on initial TC measurements in the LIPID study,20 with a significance level of <0.05. Data were analysed using SPSS for Windows (version 12.01). Baseline characteristics are presented as means and standard errors (SEM) and percentages. Follow-up values are presented as mean (SEM) for the entire cohort in each group. Data were analysed by intention to treat and p values were calculated using a general linear model (repeated measures analysis of variance (ANOVA)) with study group included as a fixed effect. The significance of differences in percentages between groups was assessed using a χ2 test.
RESULTS
Flow of study participants and baseline characteristics
Figure 2 shows the flow of participants through the CHOICE study. We identified 824 hospital admissions for ACS, of whom 446 were eligible for secondary prevention. One hundred and forty-four eligible volunteers who were not accessing rehabilitation were randomly allocated to the control (n = 72) or CHOICE group (n = 72) after blinded baseline assessment.

Baseline characteristics of the control and CHOICE groups have been previously published13 but are summarised in table 1. There were no significant differences between the control and CHOICE groups except for the proportion who were working. We have previously reported that there were no significant differences in any major risk factors between those who participated in the study and those who declined to volunteer.9 Reasons for not attending rehabilitation were not significantly different for the CHOICE and control groups and included a lack of referral (42% vs 51%), no transport (19% vs 18%), work commitments (22% vs 10%), already exercising (6% vs 11%) and not interested (11% vs 10%). Of the 37 patients with hypertension in the CHOICE group, 30 (81%) chose to participate in the BP-lowering module. Of the 62 CHOICE patients who were inactive, 53 (85%) chose to participate in the physical activity module and of the 14 smokers, 10 (71%) chose to participate in the smoking cessation module. Although there was no specific weight loss module, of the 32 CHOICE patients who were obese (BMI >30 kg/m2), 25 (78%) chose to participate in the physical activity module and at 12 months eight (32%) had a BMI <30 kg/m2.
Frequency of medical consultations
During the course of the study, almost all (96%) patients saw their family doctor or cardiologist (73%) at least once and most (83%) saw their doctor at least five times. There was no difference between groups for the frequency of family doctor visits but patients in the CHOICE (46%) and rehabilitation (50%) groups were at least three times more likely than controls (28%, p = 0.04) to visit a cardiologist.
Risk factor level and prevalence
At baseline, there was no significant difference between CHOICE and control groups for mean level or prevalence of any risk factor (table 1). At follow-up, the CHOICE group was less likely to have risk factors above recommended cut-off points (table 2), were less likely to have three or more risk factors (fig 3), had a significantly lower mean TC, LDL, SBP, BMI and significantly greater physical activity level than controls (table 2, fig 4). Of great importance, the levels achieved by the CHOICE group at 3 months were maintained for 1 year (fig 3).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Knowledge of modifiable risk factors
At baseline, the majority of patients in the CHOICE (48/72, 67%) and control (59/72, 82%) groups were unable to state any of their own risk factors. There were also no significant differences between the CHOICE and control groups in the proportion who could state the recommended levels for TC, BP and physical activity (table 3). Risk factor knowledge improved significantly only in the CHOICE group and to a proportion much higher than for controls at 3 months (not shown) and this improvement was maintained for 12 months (table 3).
At 1 year follow-up, univariate analysis of the relationship between achieving the risk factor target and patient’s knowledge of target showed a significant correlation for TC (p = 0.04) and physical activity (p = 0.01). Because of the extremely strong group effect of the CHOICE intervention on knowledge, it was not possible to show an effect of knowledge independent of group assignment in multivariate analysis.
Medications
Although similar at baseline (table 1), by 12 months, significantly more CHOICE participants than controls were taking a statin (table 2). Also, the simvastatin dose-equivalent at baseline was similar in the CHOICE (46.3 (25.3) mg) and control (45.0 (23.9) mg) groups but significantly higher in the CHOICE (56.5 (25.8) mg) than control group (43.7 (23.9) mg) at 12 months (p = 0.04). There were no other significant differences between the two randomised groups in the proportion taking any other class of cardiovascular drug or antidepressant at 12 months (table 2).
Quality of life
The CHOICE group scored significantly better (better QoL) than controls for the physical functioning domain of the SF-36 at baseline (75.6 (2.2) vs 67.6 (2.0), p<0.01) and at 12 months (76.4 (2.7) vs 64.3 (2.8), p<0.01). There were no other domain differences.
Comparison with non-randomised group attending standard rehabilitation
At baseline, participants starting rehabilitation were less likely to have a past history of cardiovascular disease (p<0.05) and more likely to have had coronary surgery (p<0.01) than participants in the control and CHOICE groups. Also at baseline, significantly more CHOICE than rehabilitation participants had three or more modifiable risk factors above the recommended level (45/72 vs 7/64, p<0.001) and fewer CHOICE than rehabilitation patients knew the recommended levels for TC (24/72 vs 43/64, p<0.001), BP (24/72 vs 35/64, p<0.01) and physical activity (22/72 vs 36/64, p<0.01). Also, as reported previously,17 CHOICE participants had higher mean levels for TC, LDL, CDS score, LIPID score and lower physical activity than the non-randomised rehabilitation group.
At 12 months, there were no significant differences between the CHOICE and rehabilitation groups for mean risk factor levels (fig 4), number with three or more risk factors (14/67 vs 16/63), proportion taking a statin (55/67 vs 57/63) and related risk factor knowledge. During the course of the study, the trajectory of risk factor levels was similar in the CHOICE and rehabilitation groups for TC and LDL. For physical activity, the mean level peaked at 3 months in the rehabilitation group, but continued to improve for 12 months in the CHOICE group (fig 4).
DISCUSSION
This randomised controlled trial focusing on the majority of ACS survivors not accessing rehabilitation demonstrates that the brief CHOICE intervention improved multiple risk factors and related knowledge compared with usual care for at least 1 year. The findings provide evidence that the previously reported short-term results17 are maintained without further intervention. The study found a large treatment effect for all primary outcomes, with baseline TC falling by 0.7 mmol/l over 12 months in the CHOICE intervention group. In the control group, there was no significant change in cholesterol concentration despite most of the patients being prescribed a statin and seeing their family doctor at least five times during the year.
Critically, our brief CHOICE intervention is feasible and potentially has broad appeal. It involved only a 1 h face-to-face consultation and a median of four 10-min phone calls over 3 months. Therefore, the programme is likely to be cost effective compared with traditional rehabilitation and can be easily translated into clinical practice in almost any location. In Australia, the majority of cardiac rehabilitation services are hospital-based, group programmes for a defined period of about 6–12 weeks. Despite rehabilitation being funded within the public hospital system, attendance rates are relatively low at 10–30%2 but are comparable to international figures. In this study, it was encouraging that about 40% of eligible patients not accessing rehabilitation volunteered. We expect that offering CHOICE as part of routine care, rather than as a research study, to all eligible patients at the time of the acute admission, or shortly thereafter, would significantly further increase its uptake and bring the programme into effect at the time of highest risk. We hypothesise that the programme was successful because the intervention engaged local service providers and was based on cognitive-behavioural research, suggesting that fostering patient active engagement is associated with improved health outcomes.12 13 15 This aspect is of particular importance for chronic diseases where patients need to make lifelong behaviour changes.
Based on research from other studies, it is likely that the multiple risk factor reductions reported in this study would translate into reduced coronary events and admissions to hospital. Secondary prevention lowering of blood cholesterol consistently improves all-cause mortality, cardiac mortality and vascular event rates.20 Similar benefits are reported for BP lowering25 and smoking cessation.26 Modelling our data with secondary prevention trials in total cholesterol20 and exercise rehabilitation27 support a likely double-digit reduction in combined events. Despite having no specific weight loss module the lower mean BMI in the CHOICE group at 12 months probably resulted from the increased level of physical activity during the course of the study. Importantly, reducing multiple risk factors concurrently, as shown in our study, as against a single factor, is likely to deliver greater reduction in events.28
Recent evidence suggests that brief secondary prevention programmes are as effective as the traditional cardiac rehabilitation model.7 As a result of these findings there is a suggestion that secondary prevention programmes might become more individualised.16 Randomised controlled trials of individualised secondary prevention programmes in Europe,29–31 the USA32 33 and Australia34 report reductions in TC compared with usual care. These interventions are based on individualised risk factor reduction to specified targets and generally involve telephone or home-based follow-up, or both. Similarly, our CHOICE programme provides further evidence for such an individualised approach but, unlike the previous studies, CHOICE allows patients to make guided choices about managing their disease, which is likely to enhance long-term behaviour change and provides extensive flexibility for patients from different geographical areas and cultural backgrounds.
In keeping with a previous study,35 our cohort of ACS survivors had poor knowledge of their risk factors, with 70% unable to state any of their own risk factors. Importantly, there is evidence that improving risk factor knowledge is positively associated with improved risk factor levels, enhanced patient active orientation, better health status and QoL.36 Our results support previous studies as we found there was a correlation between knowledge and adherence to lifestyle changes. Therefore, these results challenge clinicians to develop and investigate methods of improving patient’s knowledge and understanding of risk factors to motivate long-term change in behaviour.
Various systematic reviews and meta-analyses have reported the short-term benefits of standard cardiac rehabilitation, including improvements in risk factors as well as reductions in major CHD events, cardiac mortality and hospital readmissions compared with usual care.6 7 27 Although facility-based rehabilitation is beneficial for those who attend, it is associated with suboptimal attendance rates,1 2 and increased cost and those who do not attend are likely to have higher baseline risk.9 Very few studies have directly targeted secondary prevention of ACS survivors who do not access rehabilitation. Our findings support a previous report that patients often prefer an alternative secondary prevention model.35 Therefore, offering flexibility for patients may be the best way for enhancing uptake of secondary prevention and dealing with the evidence practice gap. Our finding that the CHOICE group compared well with the reference rehabilitation group suggests that CHOICE may be a clinically effective alternative for ACS survivors and, if offered together, the programmes may have additive effect on long-term risk factor benefits.
This study has important strengths in the nature and brevity of the intervention, the longevity of the response and the demonstrated good uptake by patients not accessing rehabilitation. However, our trial was a conducted at a single centre, which results in less heterogeneity in intervention delivery but also limits the generalisability of results, and therefore our results require replication in a multicentre trial. Future research is needed to determine which parts of the CHOICE programme are most important for maximising patient uptake and health outcomes. Also, given that many patients improve their diet after ACS with cardiac rehabilitation,37 further research investigating a CHOICE programme with a specific healthy eating module may enhance long-term adherence to dietary changes. Finally, in this study, it was noted that antiplatelet therapy was suboptimal and future interventions of this nature should consider ways to maximise prescription and adherence to proven treatments, particularly for drugs like antiplatelet agents, which do not relate directly to classical risk factor management.
CONCLUSIONS
The CHOICE study provides an important step in dealing with the evidence-practice gap resulting from suboptimal uptake of cardiac rehabilitation. Given that an estimated one in five Europeans will die before the age of 75 as a result of CHD,10 it is vital that innovative secondary prevention programmes are developed and tested. Participation in a brief CHOICE programme improves multiple risk factor levels and related knowledge for 12 months, compared with usual care. Consequently, CHOICE provides an effective alternative for the large numbers of patients not accessing traditional rehabilitation.
Acknowledgments
We thank the National Heart Foundation of Australia for their financial support, the participating patients and staff at Concord Hospital as well as Professor Jennifer Peat and Professor Adrian Bauman, and Monique Menzies for their advice and assistance.
REFERENCES
Footnotes
See Editorial, p 441
Funding: This study was supported by the National Heart Foundation of Australia in the form of a grant-in-aid (G03S1204) and postgraduate clinical research scholarship (PC0351258 for JR). The funding body was completely independent from the researchers, design, analysis and reporting of the study.
Competing interests: None.
Ethics approval: Ethical approval was obtained for the study.