Article Text

Abstract
AIM To analyse the immediate response of heart rate variability (HRV) in response to orthostatic stress in unexplained syncope.
SUBJECTS 69 subjects, mean (SD) age 42 (18) years, undergoing 60° head up tilt to evaluate unexplained syncope.
METHODS Based on 256 second ECG samples obtained during supine and upright phases, spectral analyses of low (LF) and high frequency (HF) bands were calculated, as well as the LF/HF power ratio, reflecting the sympathovagal balance. All variables were measured just before tilt during the last five minutes of the supine position, during the first five minutes of head up tilt, and just before the end of passive tilt.
RESULTS Symptoms occurred in 42 subjects (vasovagal syncope in 37; psychogenic syncope in five). Resting haemodynamics and HRV indices were similar in subjects with and without syncope. Immediately after assuming the upright posture, adaptation to orthostatism differed between the two groups in that the LF/HF power ratio decreased by 11% from supine (from 2.7 (1.5) to 2.4 (1.2)) in the positive test group, while it increased by 11.5% (from 2.8 (1.5) to 3.1 (1.7)) in the negative test group (p = 0.02). This was because subjects with a positive test did not have the same increment in LF power with tilting as those with a negative test (11% v 28%, p = 0.04), while HF power did not alter. A decreased LF/HF power ratio persisted throughout head up tilt and was the only variable found to discriminate between subjects with positive and negative test results (p = 0.005, multivariate analysis). During the first five minutes of tilt, a decreased LF/HF power ratio occurred in 33 of 37 subjects in the positive group and three of 27 in the negative group. Thus a decreased LF/HF ratio had 89% sensitivity, 89% specificity, a 92% positive predictive value, and an 86% negative predictive value.
CONCLUSIONS Through the LF/HF power ratio, spectral analysis of HRV was highly correlated with head up tilt results. Subjects developing syncope late during continued head up tilt have a decrease in LF/HF ratio immediately after assuming the upright posture, implying that although symptoms have not developed the vasovagal reaction may already have begun. This emphasises the major role of the autonomic nervous system in the genesis of vasovagal (neurally mediated) syncope.
- heart rate variability
- vasovagal syncope
- head up tilt test
Statistics from Altmetric.com
Vasovagal syncope is a common disorder, and the head up tilt test is now recognised as a valuable diagnostic tool for identifying patients suffering from the vasovagal syndrome.1-3 However, the precise aetiology and pathophysiological events underlying vasovagal syncope are not fully understood.4 Several mechanisms such as reduced blood volume, increased venous pooling, increased β adrenergic sensitivity, and augmented high pressure baroreceptor activity have been proposed to explain the development of syncope.5-9 None of these explanations has been definitive, but despite the variety of triggering factors there is a consensus that the autonomic nervous system is the final common pathway leading to syncope.
During the last decade, much progress has been made in understanding autonomic haemodynamic regulation through power spectral analysis of heart rate variability.10 Spectral analysis of heart rate variability is believed to provide important information on sympathovagal interactions11 and has been applied to the evaluation of autonomic function during head up tilt.12-20 However, most of these studies, involving small numbers of patients, have characterised autonomic changes at the time when syncope occurs, and few have examined the immediate response to tilt in patients susceptible to vasovagal response. Morilloet al 16 and Kochiadakiset al 20 previously reported an abnormal sympathovagal balance response immediately after assumption of the upright posture in subjects with unexplained syncope and a positive head up tilt response.
In the present study of patients undergoing head up tilt for evaluation of unexplained syncope, we went a step further in investigating the immediate response to tilt, using multivariate analysis to identify potentially discriminant variables. Based on the key role of the autonomic nervous system in the genesis of vasovagal syncope, we hypothesised that autonomic abnormalities occurring early during head up tilt would help to distinguish subjects with positive test results from those with negative results.
Methods
SUBJECTS
Sixty nine consecutive patients with unexplained syncope (34 women and 35 men, mean (SD) age 42 (18) years, range 16 to 75 years) referred to our department for head up tilt testing were included prospectively in this study. All of them had a history of at least one episode of syncope and several presyncopal spells, or a single episode of syncope associated with injuries during the previous six months. Medical history, clinical examination, and standard non-invasive investigations, including a 12 lead ECG in all cases, were not diagnostic of a predisposing condition. In patients managed on an ambulatory basis (the great majority), an echocardiogram, a 24 hour Holter ECG, an EEG, and a transaxial tomographic brain scan, performed at the discretion of the referring physician, were all normal. None of the patients had evidence of diabetes mellitus or neuropathy, or was taking any drug known to affect heart rate or to cause orthostatic hypotension. Tilt testing was chosen as the most appropriate way of evaluating the patients’ symptoms after the normal findings on non-invasive assessment.
Patients younger than 16 years, and those not in stable sinus rhythm or with underlying cardiac or systemic disease, were excluded from the study. Elite athletes and sports professionals were also excluded.
TILT TEST PROTOCOL
Our protocol has been detailed previously.21 Briefly, subjects were tested in the absence of any active cardiovascular drug, in the fasted state, in a quiet room with dimmed lights. Surface ECG leads I, II, and III and blood pressure using a finger cuff (Finapres, 2300 Ohmeda, Englewood, USA) were monitored continuously. The arm was support to maintain the transducer at the heart level. Baseline measurements were obtained after 15 minutes of stabilisation in the supine position. Subjects were then tilted upright to 60° for a period of 45 minutes on an electrically driven table, and if no symptoms occurred after this passive phase, isoprenaline was given in increasing doses ranging from 0.02 to 0.08 μg/kg. During the test, the subjects were asked not to speak.
HEART RATE VARIABILITY ANALYSIS
Spectral analysis of heart rate variability was performed using a previously described system.22 The device was built with a commercially available microcomputer (IBM PC, AT compatible). The ECG analogue signal was derived from a classic cardiotachometer connected to a multichannel acquisition network. The digitised signal was obtained from a smart sensor which was built with a microcontroller including an analogue to digital converter and a numerical communication port. The software allows both recording and on-line treatment of the RR intervals.
Heart rate trend was built from RR intervals, which were computed after QRS complex detection and validation. The rejection of ventricular premature complexes or any other artefact was assumed applying thresholds at ±15% of a reference RR duration. Time series data for the RR intervals were generated and then converted in a tachogram representing the fluctuations of the instantaneous cardiac frequency. The power spectrum curve was computed from a 256 second window moving along the tachogram. For each window, the mean value was removed and Bartlett windowing applied. A fast Fourier transform algorithm producing a 512 point spectrum for the 0.01 to 1.0 Hz frequency band was used to extract the spectral content. For each step of the temporal moving window, the spectrum curve was displayed to give a two or three dimensional view of the power spectrum, where the X, Y, and Z axes, respectively, represented frequencies (Hz), power (beats/min2), and time (seconds). The low frequency (LF; 0.04 to 0.15 Hz) and high frequency (HF; 0.15 to 0.4 Hz) power and bandwidth areas were calculated, as well as the LF/HF power ratio, reflecting the sympathovagal balance.23 Power was assessed by the peak frequency in the defined bands, and bandwidth area was calculated as the natural logarithm of the quotient by integrating the power density in the defined bands (beats/min2/Hz).10
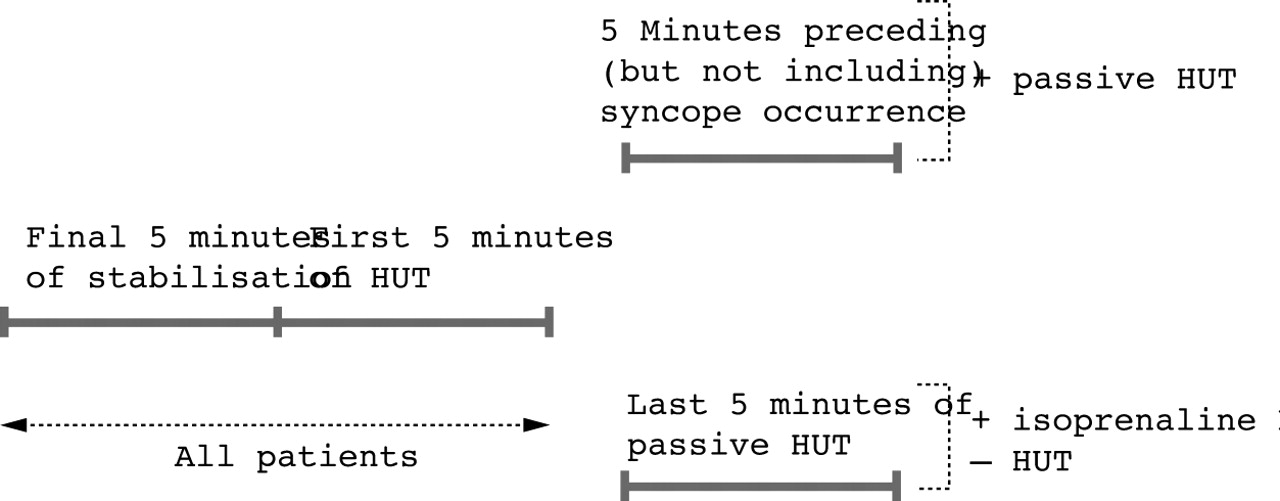
Supine variables were measured during the final five minutes of stabilisation, and upright variables during the first five minutes of head up tilt, and just before the end of its passive phase (that is, just before isoprenaline) (fig 1). If there was a positive response to head up tilt, the latter represented the five minutes immediately before the occurrence of syncope. Where the ECG recordings contained substantial amounts of noise or artefact they were classified as unanalysable and the patients were excluded.

ECG recordings for heart rate variability analysis. HUT, head up tilt.
DEFINITIONS AND DIAGNOSTIC CRITERIA
The end point of head up tilt was the induction of syncope or presyncope reproducing the patient’s clinical symptoms. Syncope was defined as a transient loss of consciousness incompatible with other altered states of consciousness, and presyncope as any of various premonitory signs and symptoms of imminent syncope. Vasovagal syncope or presyncope was diagnosed when symptoms were associated with hypotension (systolic blood pressure ⩽ 90 mm Hg) or bradycardia (heart rate ⩽ 45 beats/min), or both. Psychogenic syncope or presyncope was diagnosed when the induced symptoms where not accompanied by any change in blood pressure but were associated with intense subjective fear, tremor, sinus tachycardia (heart rate ⩾ 120 beats/min) or hyperventilation, or both, identical to spontaneous episodes.
The completion of the full duration of head up tilt, including isoprenaline infusion, was considered a negative test. Subjects who did not complete the full duration of head up tilt for reasons other than a positive test were excluded.
STATISTICAL ANALYSIS
Statistical analysis system programs (SAS Inc, Carey, North Carolina, USA) were used for the data analysis. The general linear model procedure was used to determine changes over time. The normality of each data set was examined. Two sided unpairedt tests were used to assess differences between the groups. The Welch alternate ttest was used when variances were inhomogeneous. Contingency tables were analysed using Fisher’s exact test. Stepwise linear discriminant analysis was used to study the way in which the groups differed with respect to the same clinical, haemodynamic, and heart rate variability indices. Data were expressed as mean (SD). A two tailed p value ⩽ 0.05 was considered statistically significant.
Results
HEAD UP TILT RESULTS, RESTING HAEMODYNAMIC MEASUREMENTS, AND HEART RATE VARIABILITY INDICES
Head up tilt was positive in 42 subjects: during the passive phase in 30 after a mean delay of 18 (12) minutes, and during isoprenaline infusion in the remaining 12. These positive responses included 21 cardioinhibitory responses, 16 vasodepressor responses, and five psychogenic responses. In 15 cases the positive responses corresponded to presyncope; the remaining cases were associated with frank syncope.
There were no differences between subjects with positive and negative head up tilt results with respect to age, sex distribution, number of syncopal episodes, and occurrence of trauma, injuries, or seizures during spontaneous episodes of syncope. No significant difference was observed in supine heart rate, blood pressure, or any of the spectral measures of heart rate variability (table 1).
Clinical characteristics, supine haemodynamic measurements, and heart rate variability indices of subjects with a positive head up tilt test (HUT) compared with those with a negative test
COMPARISON OF HEART RATE VARIABILITY RESULTS BETWEEN GROUPS AND WITHIN GROUPS
As shown in table 2, supine and upright spectral indices of heart rate variability were similar for patients developing syncope either during the passive phase of head up tilt or after isoprenaline sensitisation. They were therefore analysed together for the purpose of this study.
Comparison of heart rate variability indices between subjects with a positive head up tilt test (HUT) during the passive phase of tilt and those in whom HUT was positive during isoprenaline infusion
Analysis of heart rate variability during the first five minutes of head up tilt
Five subjects were excluded from the present analysis because syncope occurred during the first five minutes of head up tilt (table3).
Haemodynamic measurements and heart rate variability indices of subjects during 60° head up tilt (HUT) position
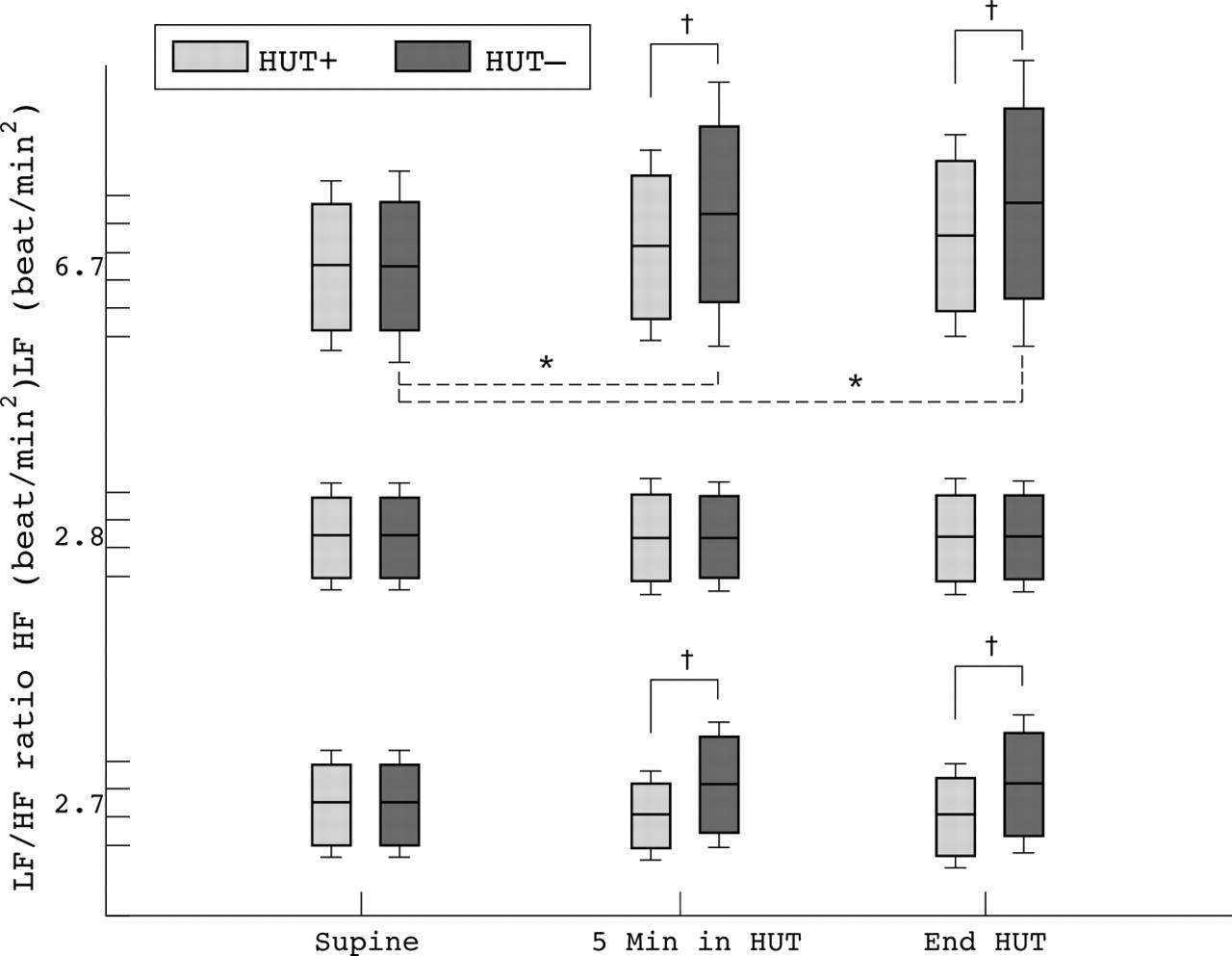
In response to upright tilt, the mean heart rate and blood pressure increased significantly and to a similar degree in both groups. These values therefore did not differ between subjects with a negative or a positive test. In contrast, the LF/HF power ratiodecreased by 11% compared with the supine value (from 2.7 (1.5) to 2.4 (1.2)) in subjects with a positive test while it increased by 11.5% (from 2.8 (1.5) to 3.1 (1.7)) in those with a negative test. The reason for this significant difference (p = 0.02) was that subjects with a positive test did not experience the same increment in LF power with tilting as those with a negative test (11%v 28%, p = 0.04), while HF power changes did not differ significantly between the two groups (figs 2 and 3). The LF/HF bandwidth area ratio varied in the same way (p = 0.05), as shown in table 3. When using multivariate analysis, a decreased LF/HF power ratio was the sole variable found to discriminate between patients with a positive head up tilt result and those with a negative result (p = 0.005). The 95% confidence intervals of the estimates were 2.03 to 2.77 and 2.43 to 3.77, respectively.

Changes in low frequency (LF), high frequency (HF), and LF/HF power ratio with upright tilt in the study group. HUT, head up tilt; *p < 0.05, upright v supine;†p < 0.05, positive HUT v negative HUT.
{kind=link}
{kind=link}
{kind=link}
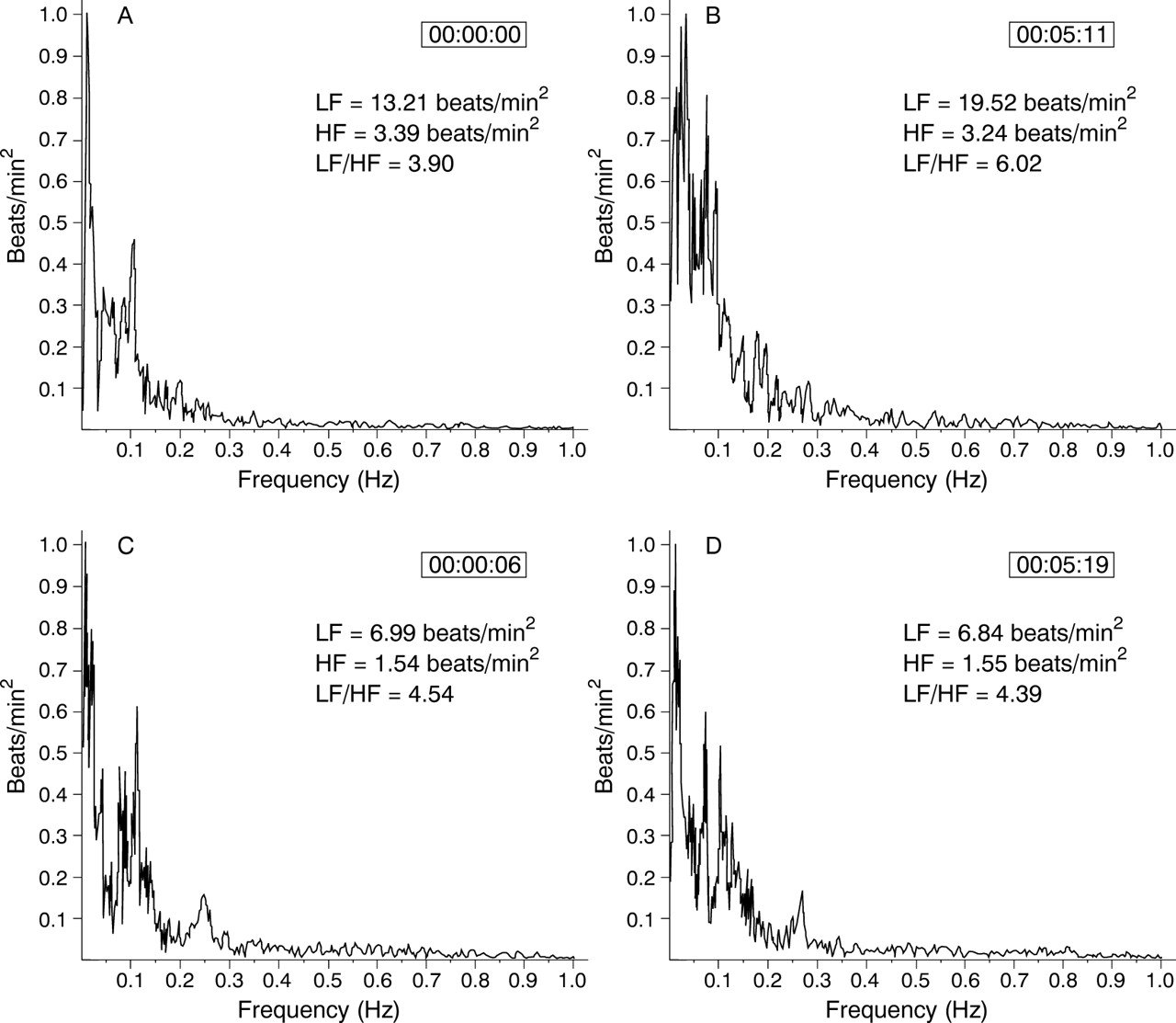
Heart rate variability power spectrum calculated by fast Fourier transform algorithm. Example of supine (A) and upright (B) spectrum of a patient with a negative head up tilt test, compared with those of a patient with a positive test (C, D).
Spectral analysis of heart rate variability at the end of the passive phase of head up tilt
A decreased LF/HF power ratio was also observed at the completion of the test (that is, during the five minutes preceding symptoms for subjects with a positive passive head up tilt or during the last five minutes of passive head up tilt for all the others), and was once again the sole variable found to discriminate between the two groups (table3; fig 2). The overall increase in the LF power compared with the supine value was 15% in the positive group and 32% in the negative group (from 6.7 (3.4) to 7.7 (3.6) beats/min2 v 6.8 (4.1) to 8.9 (4.8) beats/min2, p = 0.04), without any change in the HF power (table 3).
COMPARISON BETWEEN SUBJECTS WITH VASOVAGAL SYNCOPE AND SUBJECTS WITH A NEGATIVE TEST
Results were similar when comparison was restricted to the 37 subjects in whom vasovagal syncope occurred during head up tilt (that is, after withdrawal of the five subjects with psychogenic syncope) (table 4).
Upright haemodynamic variables and heart rate variability indices of patients with tilt induced vasovagal syncope compared with those with a negative head up tilt test (HUT)
Comparison within patients with a positive test
Supine and upright heart rate variability measurements were not different in subjects with cardioinhibitory responses compared with those with vasodepressor or psychogenic syncope (table 5). Surprisingly, subjects with psychogenic syncope had the same decline in the LF/HF power ratio as those with vasovagal syncope.
Clinical characteristics, upright haemodynamic measurements, and heart rate variability indices among the 42 patients with head up tilt test (HUT) induced symptoms
LF/HF ratio as a predictor of head up tilt induced syncope
A decrease in the LF/HF power ratio was noted in 33 of the 37 subjects with a positive test (89%) during the first five minutes of tilt, and in 35 of the same group (95%) at the completion of the protocol. In the negative group, three of the 27 patients (11%) had a decrease in the LF/HF power ratio during the first five minutes of tilt and 10 (37%) at the end of the protocol. Thus a decrease in the LF/HF power ratio after five minutes of tilt had 89% sensitivity, 89% specificity, a 92% positive predictive value, and an 86% negative predictive value for predicting the tilt test result.
Discussion
BACKGROUND AND MAIN FINDINGS
In normal subjects, the autonomic response to head up tilt has been well documented. Increased LF power and decreased HF power, as well as an increased sympathovagal balance, reflect the normal response to upright tilt.23-26
Our major finding here is that patients with a positive tilt test have a different autonomic response to orthostatism. In those patients who subsequently developed syncope considerably later during continued head up tilt, a decline in the LF/HF power ratio occurred immediately after they assumed the upright position, implying that although symptoms had not yet developed the vasovagal reaction may already have begun. Moreover the LF/HF power ratio—reflecting the sympathovagal balance—was found to be the sole variable allowing discrimination between the two groups studied, and was highly predictive of the occurrence of syncope.
PATHOPHYSIOLOGICAL IMPLICATIONS
The nature of the events leading to tilt induced vasovagal syncope is unclear, but it is thought to be a clinical example of the Bezold-Jarisch reflex.4 The currently accepted model is that reduced filling pressure and increased inotropic activity leads to firing of left ventricular mechanoreceptors, with consequent abrupt withdrawal of sympathetic tone and an increase in parasympathetic tone.5 Central to this model is the role of the autonomic nervous system, both as a trigger and as the ultimate effector in producing syncope.
Spectral analysis of heart rate variability has been used to explore dynamic mechanisms in the cardiovascular system and appears to provide a quantitative evaluation of the sympathovagal interaction that modulates cardiovascular function.11 It has been shown that harmonic oscillations in heart rate are concentrated into at least two distinct bands. The one referred to as the low frequency band is affected by the oscillatory rhythm of the baroreceptor system and is thought to be mediated by both sympathetic and parasympathetic influences. The other, the high frequency band, has respiration as the primary rhythmic stimulus and is mediated by changing levels of parasympathetic tone. Heart rate variability involves a complex interaction between several mechanisms working to maintain heart rate and blood pressure within normal limits.
Results of heart rate variability during head up tilt tests have been conflicting.13 ,15-20 In the present study, we did not observe any withdrawal of LF power in patients with a positive head up tilt test, but in contrast we noted an inappropriate increase in LF power when they assumed the upright posture. This is in agreement with the findings of Morillo et al and Kochiadakis et al,16 ,20 who also noted the absence of sympathetic stimulation and reported a markedly lower LF/HF power ratio immediately after head up tilt and during the last few minutes before the end of tilt in patients with induced syncope.
On the other hand, it has been presumed that parasympathetic tone increases in the presyncopal period in vasovagal syncope.5In our study, we were unable to find any significant difference in the HF power to support this view. Previous reports by Sneddonet al,14 Morilloet al,16 and Prinz-Zaisset al,18 in which an increase in the HF component did not appear to be associated with tilt induced vasovagal reactions, are also in agreement with our results. Moreover Lippman et al, using time domain analysis, found that parasympathetic tone—assessed by the root mean square of successive differences in RR intervals—failed to decrease in vasovagal patients and predicted a positive head up tilt response with 100% specificity and 41% sensitivity.17
HAEMODYNAMIC RESPONSE TO TILTING AND HEART RATE VARIABILITY IN NORMAL SUBJECTS
Using analysis of heart rate variability, previous investigators have already shown that in normal subjects LF oscillations are modulated by the baroreflex response, and that an increase in LF power is usually interpreted as mainly indicating an increase in sympathetic tone.23-26 In fact on standing, the rapid migration of blood from the thorax to the lower parts of the body results in a decrease in venous return and a fall in cardiac output. These changes promptly activate compensatory mechanisms, among which the baroreflex is of primary importance, and which include vagal withdrawal and sympathetic stimulation, with a consequent increase in heart rate and total peripheral resistance. In the light of these data and the inadequate sympathovagal response to tilt found within patients with induced syncope in our study, it seems likely that firing of one or more groups of arterial or cardiopulmonary baroreceptors may be at least partly responsible for the vasovagal response.
SUSCEPTIBILITY TO VASOVAGAL (NEURALLY MEDIATED) SYNCOPE
In the present study, we tested the hypothesis that autonomic abnormalities early during head up tilt would help distinguish patients with positive test results from those with negative results. The decrease in the LF/HF power ratio which occurred earlier during head up tilt, long before symptoms developed in the syncopal patients, emphasises the major role of autonomic abnormalities in the genesis of vasovagal syncope. An explanation of this phenomenon may be an abnormal response of the arterial or cardiopulmonary baroreceptors in patients susceptible to vasovagal syncope, which could be triggered by orthostatic stress such as provoked by head up tilt, or by psychological stress. Preliminary data reported by Cohen et al suggest that there is a parallel response between the LF/HF ratio and forearm vascular resistance when lower body negative pressure is applied.27 Sneddonet al reported an impaired immediate vasoconstrictor response in patients with vasovagal syncope long before the onset of syncope, and suggested there was an abnormality of the cardiopulmonary baroreceptor reflex arc.28 Manyariet al found an abnormal range of forearm venomotor responses during mental arithmetic stress,29 and Van Den Berg and Smit30 reported abnormally slight responses to sympathetic tests in some patients with vasovagal syncope, lending support to this concept. Finally, on the basis of our findings and those of previous investigators, it could be—as suggested by recent animal studies31 or by tilt induced hypotension and bradycardia after heart transplantation in humans32—that activation of cardiac mechanoreceptors is not the sole mechanism mediating the vasovagal response. Abnormalities of vascular control immediately after standing up may play an important early role in vasovagal (neurally mediated) syncope.
In the present study, the same decline in the LF/HF power ratio in response to orthostatism was found in patients with vasovagal syncope as in those with psychogenic syncope. It is usually considered that psychiatric disorders are marked by a loss of HF activity and by increases in LF tone,33 in contrast to our findings. However, psychogenic syncope is probably not a homogeneous entity. Although panic attacks are an extreme manifestation of sympathetic hyperactivity, blood phobia, which is another expression of anxiety disorder, involves bradycardia and hypotension which may ultimately lead to syncope.34 Therefore, one cannot rule out the possibility that there is a similar pathological mechanism in common vasovagal syncope and in the small group of psychogenic syncopal disorders in the present report.
STUDY LIMITATIONS
We used a fast Fourier transform method to analyse heart rate variability despite the fact that data segments obtained during early orthostatic stress were not rigorously stationary. Respiratory frequency was not controlled during the test and may have influenced the power spectrum of both frequency bands assessed. We did not include a group of normal control subjects because the purpose of our study was particularly to examine immediate differences in heart rate variability among patients referred for evaluation of suspected vasovagal syncope. Thus in the absence of a gold standard for this diagnosis (in the face of a negative head up tilt response), the influence of patient selection on our results is uncertain. Bearing in mind these limitations, data from control subjects are essential and further studies are necessary before heart rate variability analysis can be applied as a clinical test to predict a positive head up tilt result.
We also used the LF/HF power ratio as an index of the sympathovagal balance, on the basis of reports by Pagani et al.23 ,26 Recently, some limitations on the use this ratio as an index of sympathovagal balance have been reported in a very detailed review by Eckberg.35 However, despite these limitations and the use of an indirect method for the assessment of autonomic nervous activity (which can be assumed to represent global events), we consider that power spectral analysis of heart rate variability contributes to a fuller understanding of the pathophysiological mechanism of vasovagal syncope by providing a picture of the changes that occur throughout the tilt testing procedure.
CONCLUSIONS
There is a disturbed sympathovagal balance in response to orthostatism in patients with unexplained syncope and a positive response to head up tilt. In these patients, spectral analysis of heart rate variability showed that the LF/HF power ratio was highly correlated with head up tilt results after only five minutes of tilt. This findings suggest that in patients susceptible to vasovagal syncope, the cycle of events begins very soon after tilt, but only becomes clinically evident later on.
Acknowledgments
We thank Isabelle Fremaux, Christine Monier, and Dominique Debus for their nursing and technical assistance.