Article Text

Abstract
Objectives Prasugrel and ticagrelor both reduce ischaemic endpoints in high-risk acute coronary syndromes, compared with clopidogrel. However, comparative outcomes of these two newer drugs in the context of primary percutaneous coronary intervention (PCI) for ST-elevation myocardial infarction (STEMI) remains unclear. We sought to examine this question using the British Cardiovascular Interventional Society national database in patients undergoing primary PCI for STEMI.
Methods Data from January 2007 to December 2014 were used to compare use of P2Y12 antiplatelet drugs in primary PCI in >89 000 patients. Statistical modelling, involving propensity matching, multivariate logistic regression (MLR) and proportional hazards modelling, was used to study the association of different antiplatelet drug use with all-cause mortality.
Results In our main MLR analysis, prasugrel was associated with significantly lower mortality than clopidogrel at both 30 days (OR 0.87, 95% CI 0.78 to 0.97, P=0.014) and 1 year (OR 0.89, 95% CI 0.82 to 0.97, P=0.011) post PCI. Ticagrelor was not associated with any significant differences in mortality compared with clopidogrel at either 30 days (OR 1.07, 95% CI 0.95 to 1.21, P=0.237) or 1 year (OR 1.058, 95% CI 0.96 to 1.16, P=0.247). Finally, ticagrelor was associated with significantly higher mortality than prasugrel at both time points (30 days OR 1.22, 95% CI 1.03 to 1.44, P=0.020; 1 year OR 1.19 95% CI 1.04 to 1.35, P=0.01).
Conclusions In a cohort of over 89 000 patients undergoing primary PCI for STEMI in the UK, prasugrel is associated with a lower 30-day and 1-year mortality than clopidogrel and ticagrelor. Given that an adequately powered comparative randomised trial is unlikely to be performed, these data may have implications for routine care.
- prasugrel
- ticagrelor
- clopidogrel
- antiplatelet drugs
- primary PCI
Statistics from Altmetric.com
Introduction
Dual antiplatelet therapy using aspirin plus P2Y12 inhibitor agents such as clopidogrel in percutaneous coronary intervention (PCI) have improved clinical outcomes, with reductions in stent thrombosis and improved ischaemic outcomes.1 2 However, there are important limitations with the use of clopidogrel. Genetic variability in the enzymatic activation of clopidogrel is associated with functional ‘hypo’-responders to this drug, with individuals at increased risk of adverse ischaemic events.3 The relatively slow onset of action, even with high-dose loading regimens,4 may be disadvantageous in the emergency setting of primary PCI for ST-elevation myocardial infarction (STEMI). Such limitations stimulated the drive for novel P2Y12 inhibitors, including prasugrel and ticagrelor, offering faster onset and more potent inhibition of platelet activity. Both prasugrel and ticagrelor have been shown to have clinical outcome benefit in large randomised trials in a variety of acute coronary syndromes (ACS)5 6 although at increased risk of non-coronary artery bypass graft (CABG) related major bleeding. Use of these novel agents in the UK has been targeted in real-world practice to those contexts where ischaemic risks are greatest, such as in primary PCI. It is notable that the post hoc analyses of both Platelet Inhibition and Patient Outcomes (PLATO) and Trial to Assess Improvement in Therapeutic Outcomes by Optimizing Platelet Inhibition with Prasugrel-Thrombolysis in Myocardial Infarction 38 (TRITON TIMI 38) failed to show a statistically significant benefit for ticagrelor or prasugrel over clopidogrel in the primary PCI subgroups of their heterogeneous ACS populations,7 8 and in fact, only 68% of the TRITON TIMI 38 STEMI cohort underwent primary PCI,9 ,10Similarly, in the PLATO trial, out of 7544 ACS patients with STEMI or left bundle branch block patients only 65.6% (n=4949) underwent primary PCI.
Although prasugrel and ticagrelor are both Adenosine diphosphate (ADP)-receptor antagonists, there are a number of differences between them, including their pharmacodynamics, drug interactions and side-effect profile.11 Switching between the two agents produces demonstrable changes in platelet function.11 12 The landmark ACS trials (PLATO and TRITON) also found important differences in outcomes with these two drugs.5 7 However, outcomes from these landmark trials cannot be directly compared due to important differences in study populations, study design and inclusion/exclusion criteria.13
There has been no head-to-head randomised comparison of clinical outcomes for prasugrel versus ticagrelor until the recently presented PRimary Angioplasty in patients with myocardial infarction transferred from General community hospitals to angioplasty Units of tertiary cardiology centers with or without Emergency thrombolysis (PRAGUE)-18 trial in STEMI and highest-risk NSTE-ACS14 in which no significant differences were observed in either the 7-day composite efficacy (primary) endpoint or the 30-day key safety endpoint. However, this trial was prematurely stopped after interim analysis and a severe statistical underpowering to address the planned aim. A trial of adequate power for a head-to-head comparison between prasugrel versus ticagrelor would probably require a sample size approaching 15 000 patients,15 with implications for the iNtracoronary stenting and antithrombotic regimen: Rapid early action for coronary treatment 5 randomised controlled trial (RCT) aimed at addressing this question.16
In the context of (a) limited data regarding comparative outcomes associated with ticagrelor and prasugrel use and (b) the unlikelihood of an adequately powered randomised trial to compare them in the future, our aim was to use the national British Cardiovascular Intervention Society (BCIS) PCI registry to explore outcomes associated with different P2Y12 antiplatelet agents in a large real-world national cohort that captures >99% of PCI cases performed in the UK.
Methods
Study design and data collection
This is a retrospective analysis of prospectively collected national data for all patients undergoing primary PCI in England and Wales from January 2007 to December 2014. BCIS records information on PCI practice in the UK with data collection managed by the National Institute of Cardiovascular Outcomes Research.17–20 The BCIS database contains 113 clinical, procedural and outcome variables with more than 80 000 new records added each year. Using the Medical Research Information Services, we tracked the life status of patients using their National Health Service (NHS) number, a unique identifier for any person registered within the NHS. All the data were collected as part of a national audit and were anonymised; therefore, institutional review board approval was not required for this study.
Outcomes
Our outcomes were mortality at 30 days and 1 year, inhospital major bleeding complication and major adverse cardiovascular events (MACE). Bleeding complications were defined as a composite of reported gastrointestinal bleed, intracerebral bleed, retroperitoneal haematoma, tamponade, blood or platelet transfusion, or an arterial access site complication requiring intervention,17 21 22 while a composite of inhospital mortality, reinfarction and revascularisation (emergency CABG or reintervention PCI) constituted MACE.19 21
Study aim
The primary aim of this study was to investigate the association between the use of a particular antiplatelet drug (clopidogrel, prasugrel and ticagrelor) and 30-day and 1-year mortality.
Statistical analysis
Patient exclusion criteria
The data presented relate to all reported primary PCI procedures undertaken in patients in England and Wales between 1 January 2007 and 31 December 2014. Procedures were excluded if outcome data, age or gender were missing from the dataset.
Descriptive statistics
For basic analyses of demographics, procedural details and unadjusted outcomes, continuous variables were evaluated as median and IQR, while categorical variables were reported using frequencies and proportions (in percentages). Medians, IQRs, frequencies and percentages quoted for unadjusted data refer to numbers within the cohort where data were available. χ2 tests were used to assess the significance of differences in proportions between groups for categorical variables. Kruskal-Wallis rank-sum test was used for continuous variables. All statistical tests were two-tailed and an alpha of 5% (for significance) was used throughout.
Multiple imputations for missing data
Multiple imputation methods were used in order to reduce potential bias created by missing data.23 To this aim, we used the mice R package V.2.2524 which is freely available on the The Comprehensive R Archive Network repository (https://cran.r-project.org). Chained equations were used to impute data for all variables with missing values to generate 10 dataset instances for use in the analyses.
Multivariate statistical modelling
Multivariate logistic regression models were performed over the multiple imputed dataset instances in order to elucidate associations, in the form of ORs, between antiplatelet drug selection and adverse outcomes. We also used multivariate Cox regression models to estimate HRs between antiplatelet and survival time outcome censored to 1 year. In order to control for potential confounding, all models were adjusted for the following covariates: age, gender, smoking status, diabetes, history of peripheral vascular disease (PVD), hypertension, hypercholesterolaemia, history of renal disease, previous CABG, previous myocardial infarction (MI), previous stroke, previous PCI, left ventricular ejection fraction, preprocedural TIMI flow score, access site, vascular closure device use, stent type, vessel attempted, cardiogenic shock (CS), intra-aortic balloon pump (IABP) use, ventilatory support, thrombectomy, glycoprotein IIb/IIIa inhibitors (GPIs) use, bivalirudin use and year of procedure.
Propensity score matching
A sensitivity analysis was performed using propensity score matching. The method was implemented in three separated logistic regression models (prasugrel vs clopidogrel, ticagrelor vs clopidogrel and ticagrelor vs prasugrel) over the multiple imputed dataset instances using the aforementioned variables as explanatories and the antiplatelet drug use as the outcome. We used the MatchIt R package V.2.4–2125 to estimate the propensity scores and to form the new matched dataset instances according to them. As initial settings, we used the nearest-neighbour matching method, and no procedures were discarded. Depending on the type of outcome, binary or survival time, conditional logistic or Cox regression models were performed, respectively, over the matched dataset instances.
Results
A total of 125 424 primary PCI procedures were undertaken on patients in England and Wales between 2007 and 2014, of which 89 067 (71.0 %) were included in the descriptive analyses and statistical modelling. Figure 1 displays a detailed flow chart for procedure inclusion/exclusion criteria, the most common reasons being that antiplatelet agent was unknown in 34 265 procedures (27.42%).

Flow chart for procedure inclusion/exclusion. NHS, National Health Service.
Figure 2 provides details on antiplatelet agent in primary PCI use at primary care trust (England) and local health board (LHB, Wales) levels. This figure shows differences in use across England and Wales over time, ticagrelor mainly being prescribed in Northern England and in some parts of the London area, while prasugrel seems to be favoured in West England and some LHBs in Wales.
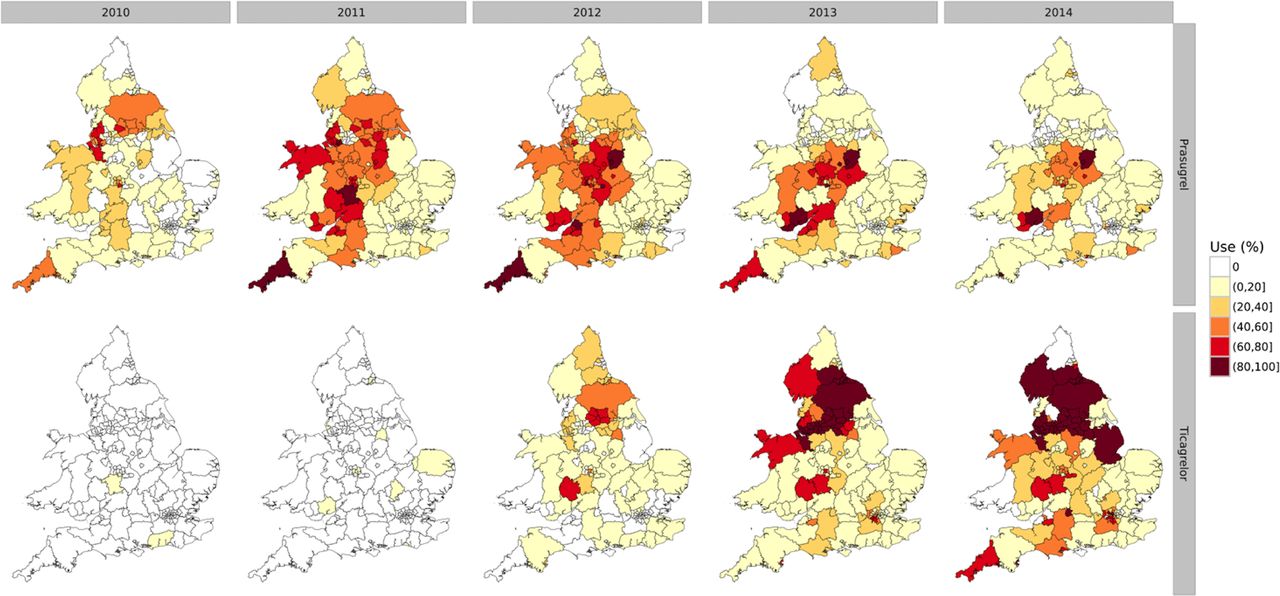
Changes in use of antiplatelet drugs in primary care trusts in England and local health boards in Wales.
Table 1 presents baseline patient demographics, procedural details, pharmacology and outcomes for the three antiplatelet groups. . Results of statistical tests included in table 1 illustrate significant differences among the groups. For instance, patients from the clopidogrel group were older and more likely to be female, and to have a history of PVD, hypertension, hypercholesterolaemia, renal disease, CABG, MI, stroke or PCI. Patients prescribed with prasugrel are younger, more likely to be male and current smokers, and less likely to be diabetics, while patients in the ticagrelor group were more likely to be non-smokers.
Baseline patient demographics, procedural details, pharmacology and outcomes
Differences in procedural characteristics between the three groups were also observed, with procedures within the clopidogrel group less likely to be undertaken through the radial route, more likely to have multivessel PCI and present with CS, and to require the use of IABP, although less likely to receive thrombectomy. Procedures within the prasugrel group were more likely to have patients with TIMI 0 flow, but less likely to require ventilatory support, while drug-eluting stents were more likely to be used within the ticagrelor group. In addition, the use of bivalirudin is considerably less frequent within the clopidogrel group while GPIs are less likely used within the ticagrelor group.
Crude mortality at both 30 days and 1 year were highest in patients treated with clopidogrel (6.5% and 10.2%, respectively; P<0.0001) and lowest in patients treated with prasugrel (3.6% and 5.9%; P<0.0001) (ticagrelor 5.5% and 8.5%; P<0.0001). Similarly, inhospital MACE was significantly lower in the prasugrel group (3.2%) compared with either the group receiving clopidogrel (4.9%) or ticagrelor (4.8%), P<0.0001, while crude inhospital bleeding rates were higher in the clopidogrel group (1.5%) compared with either prasugrel (0.7%) or ticagrelor (0.6%), P<0.0001.
Table 2 shows the results of fitting multivariate logistic regression models to the original multiple imputed datasets. Compared with clopidogrel, prasugrel was associated with a lower risk of mortality at both 30 days (OR 0.87, 95% CI 0.78 to 0.97, P=0.014) and 1 year (OR 0.89, 95% CI 0.82 to 0.97, P=0.011). Prasugrel was also associated with decreased inhospital major bleeding (OR 0.73, 95% CI 0.59 to 0.91, P=0.005) although no significant differences in inhospital MACE were observed (OR 0.94, 95% CI 0.84 to 1.06, P=0.30). In contrast, no significant differences in either 30-day (OR 1.07, 95% CI 0.95 to 1.21, P=0.24) or 1-year mortality (OR 1.06, 95% CI 0.96 to 1.16, P=0.25) were observed between patients receiving ticagrelor compared with those receiving clopidogrel. Finally, ticagrelor was associated with an increased risk of 30-day (OR 1.22, 95% CI 1.03 to 1.44, P=0.020) and 1-year (OR 1.19, 95% CI 1.04 to 1.35 P=0.01) mortality compared with the prasugrel group. A similar increased risk of inhospital MACE (OR 1.25, 95% CI 1.06 to 1.47, P=0.008) was observed associated with the use of ticagrelor compared with prasugrel, although no significant differences in inhospital major bleeding were observed.
Results of multivariate logistic regression models
Figure 3 displays the Kaplan-Meier estimates of the survivor function for the three cohorts and adjusted for the same set of covariates used before. Survival analyses were performed using multivariate Cox regressions, in which the survival time outcome was censored at 1 year. Table 3 summarises the results, which shows associations between antiplatelet use and mortality. Prasugrel was associated with no significant difference in mortality compared with clopidogrel (HR 0.94, 95% CI 0.87 to 1.01, P=0.084), while use of ticagrelor was associated with a significant increased mortality risk (HR 1.10, 95% CI 1.02 to 1.19, P=0.019). Patients treated with ticagrelor also had a significantly greater risk of mortality than those patients receiving prasugrel (HR 1.13, 95% CI 1.01 to 1.27, P=0.030).

{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier curves for the propensity-score-matched datasets. CIs are represented by coloured shades.
Results of multivariate Cox regression models with survival time censored at 1 year
A sensitivity analysis was performed by fitting conditional logistic and Cox regressions over 10 propensity-score-matched dataset instances (see online supplementary table S2 that provides an overview of the propensity-score-matched datasets and table 4), and in general, the findings were materially similar, namely, use of prasugrel was associated with a lower risk of mortality compared with ticagrelor, although no significant differences in mortality were demonstrated associated with the use of ticagrelor (compared with clopidogrel). Furthermore, prasugrel use was independently associated with a lower risk of mortality compared with ticagrelor. Three further sensitivity analyses were performed using, first, a restricted dataset containing procedures undertaken since 2010 only, when all three antiplatelet drugs were available in the UK, and second, a dataset which extends the prasugrel and ticagrelor group definitions to allow inclusion of procedures in which patients were prescribed clopidogrel and prasugrel, and clopidogrel and ticagrelor (presumably reflecting pretreatment with clopidogrel prior to prescription of either ticagrelor or prasugrel that was observed in 1.8% of cases), respectively. Finally, a third sensitivity analysis was undertaken by including the patients in whom the antiplatelet status was unknown. Results from these analyses are presented in online supplementary tables S3–S5. Supplementary Table S5 also describes details of patient demographics, procedural details, pharmacology and outcomes for patients where antiplatelet regimen was missing.
Supplementary file 1
Sensitivity analysis 1. (A) Results of conditional logistic regression models. (B) Results of Cox regression models with survival time censored at 1 year.
Discussion
Rationale for the present study
Both prasugrel and ticagrelor are associated with lower rates of ischaemic endpoints compared with clopidogrel in large randomised trials that included a heterogeneous population of patients with ACS. However, two important questions that relate directly to clinical practice remain unclear. First, whether the newer agents are significantly better than clopidogrel in a primary PCI population, and second, the relative benefits of these two novel agents compared with each other.
With a specific focus on STEMI, the landmark RCTs came to different conclusions in their relevant post hoc subgroup analyses. In the PLATO subgroup of patients treated with primary PCI within 12 hours of STEMI,10 ticagrelor did not show a significant reduction in the primary efficacy endpoint versus clopidogrel, nor did it reduce cardiovascular death (in contrast with the overall study population). The possible reasons for this are various but include the smaller cohort size (around 4000 patients) compared with over 70 000 patients included in our analysis. Similarly, the TRITON subgroup that underwent primary PCI (with around 2300 patients) also demonstrated no significant reduction in the primary endpoint with prasugrel compared with clopidogrel.9 We therefore attempted to evaluate the relative benefits of prasugrel versus ticagrelor in primary PCI from a large observational registry, and the present analysis provides the first comparative evaluation between prasugrel and ticagrelor in the ‘real world’ from a national perspective.
Interpreting key findings of our study
Association of P2Y12 antagonist and clinical outcomes
Certain baseline demographics are noteworthy when considering the association of oral antiplatelet agents and mortality in the present work. For example, radial access was far more frequently employed in patients receiving ticagrelor and prasugrel than in those receiving clopidogrel. The reasons behind this are not immediately clear but may be partly time-dependent, since radial use in the UK progressively increased over the study period (2009–2014)18 and a greater proportion of the clopidogrel cases were undertaken in the earlier part of this period compared with the other two agents. Given the relationship between radial access and reduced major bleeding and mortality in STEMI,22 26 27 this would favour outcomes in groups that received prasugrel and ticagrelor. Furthermore, the group that received clopidogrel had a higher incidence of adverse risk factors for outcome, for example, evidence of CS at presentation and a history of previous stroke. Hence, it was not surprising to find that unadjusted (raw) data indicated both novel potent antiplatelets were associated with a significant mortality advantage over clopidogrel.
After multivariate adjustment for differences in baseline covariates, the significant mortality impact of the newer agents (each compared with clopidogrel) was found to persist for prasugrel but not for ticagrelor. The mortality finding for prasugrel versus clopidogrel in our main adjusted analyses is interesting, since a reduction in the primary endpoint (of cardiovascular death, MI or stroke) at 15 months was also observed in the TRITON STEMI subgroup that underwent PCI (with around 3000 patients) with prasugrel compared with clopidogrel (HR 0.79, 95% CI 0.65 to 0.97; P=0.022),9 although not in the primary PCI subgroup (HR 0.89, 95% CI 0.69 to 1.13). The primary PCI subgroup in TRITON was much smaller in size than ours (2340 vs over 70 000 cases), hence it may simply be that the much larger population in our registry allowed a mortality effect too small to detect in the RCT to be demonstrated. Another pertinent factor arises from the likely pattern of use of prasugrel in our study versus that in TRITON. Given the real-world setting of our study, it is likely that prescribing guidance for prasugrel was largely followed and hence groups with neutral or adverse effect with prasugrel from TRITON were under-represented in our study’s prasugrel group (as seen from patient age and history of stroke in table 1). This too may have contributed to a larger advantage of prasugrel over clopidogrel in our work, compared with the landmark RCT. For the comparison of prasugrel versus ticagrelor, our mortality findings at both early (30 days) and later (1 year) time points favoured prasugrel in the main analysis. Although there are potential unadjusted confounders or selection bias inherent in a study such as this, the differences described here may well reflect a genuine difference in clinical effect, rather than related to confounders or selection bias. Compliance may be a factor, since prasugrel is a once-daily medication whereas ticagrelor has a two-times-a-day regimen for use, and this may predispose to better adherence to prasugrel prescriptions. Another possible influence on compliance is the differing side-effect profiles—for example, dyspnoea sometimes noted with ticagrelor (but not prasugrel) might be a reason underlying non-compliance or unplanned switching to another agent, again potentially impacting on outcomes. Differences in pharmacodynamics between prasugrel and ticagrelor in patients presenting with STEMI may contribute to our findings.28 For example, in one randomised study 2-hour postloading dose ticagrelor achieved 12% platelet inhibition compared with 48% with prasugrel. Furthermore, the mean time to achieve platelet reactivity <240 units (using Accumetrics VerifyNow) was 3±2 hours with prasugrel compared with 5±4 hours in patients treated with ticagrelor.28 In a further analysis of 16 000 patients with ACS managed with PCI, treated with either prasugrel or ticagrelor, both MACE (HR 0.80, 95% CI 0.64 to 0.98, P=0.03) and net adverse clinical events (HR 0.78, 95% CI 0.64 to 0.94, P=0.009) were significantly lower in the prasugrel groups compared with ticagrelor in a propensity-score-matched cohort.29 Similarly, a recent network meta-analysis of 37 studies including 88 402 patients that sought to compare the clinical efficacy and safety of P2Y12 inhibitors in patients with STEMI undergoing primary PCI demonstrated that prasugrel was associated with reduced risk of 30-day mortality (OR 0.69, 95% CI 0.56 to 0.84) and 30-day MACE (OR 0.69, 95% CI 0.56 to 0.84), but not cardiovascular mortality (OR 0.74, 95% CI 0.43 to 1.25) or major bleeding (OR 0.76, 95% CI 0.57 to 1.05).30
Nevertheless, in keeping with all observational studies, the potential for undetected or unquantified confounders exists. An important limitation, specific to this work, relates to the recording of P2Y12 blocker choice on the registry database at the time of the primary PCI procedure. Hence, it is not possible to detect cases where there may have been premature drug discontinuation or substitution of the initially selected agent later in the clinical course, for example, due to side effects or whether the antiplatelet agent was given preprocedure or postprocedure. We acknowledge that there is likely to be selection bias, in that newer antiplatelet agents are more likely to be prescribed to less sick, younger patients that may drive some of our observations, although it is unlikely that such a mechanism would explain the differences in outcomes that we report between the two newer (prasugrel and ticagrelor) agents. Finally, our secondary endpoints (inhospital major bleeding and inhospital MACE) are based on retrospective recording (by operators or other team members) of these complications and are not externally validated. This is in contrast with the highly robust mortality tracking, derived from linkage of the PCI registry to the national UK mortality database. Hence, the conclusions drawn from these secondary endpoints are acknowledged to be less robust than our mortality outcomes.
Conclusions
In a cohort of just over 89 000 patients undergoing primary PCI for STEMI in clinical practice in the UK, prasugrel is associated with a lower 30-day and 1-year mortality than clopidogrel and ticagrelor. Give that it is unlikely that an adequately powered randomised trial will be undertaken to compare them in the future, these data may have implications for routine clinical care.
Key messages
What is already known on this subject?
Both prasugrel and ticagrelor have been shown to have clinical outcome benefit in large randomised controlled trials (RCTs) of heterogeneous populations with acute coronary syndromes. However, there have been no head-to-head adequately randomised comparisons of clinical outcomes for prasugrel versus ticagrelor in primary percutaneous coronary intervention(PPCI).
What might this study add?
We observe that prasugrel was associated with significantly lower mortality than clopidogrel at both 30 days and 1 year post-PCI while ticagrelor was not associated with any significant differences compared with clopidogrel at these time points. Ticagrelor is associated with significantly higher mortality in PPCI than prasugrel at both time points.
How might this impact on clinical practice?
Our findings regarding the use of different P2Y12 antiplatelet agents in ST-elevation myocardial infarction and their association with mortality are a timely and important contribution to the literature and one that may influence practice as best currently available evidence in the absence of a more definitive RCT.
References
Footnotes
IO and AS contributed equally.
Contributors MAM, IO and AS designed the study, acquired and interpreted data, and drafted the first draft of manuscript. IO analysed the data. MAM and IO agree to be the guarantors who are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. NC, TK, PL, JB, MR, DJRH-S, MAdB and AB made substantial contributions to the design of the work and critically revised the report.
Funding Unrestricted educational grant from Daiichi Sankyo to MAM.
Disclaimer The funder had no role in the design of study, preparation of manuscript or access to the contents of the manuscript prior to submission.
Competing interests MAM has received unrestricted educational grants from Terumo and Daiichi Sankyo. NC has received unrestricted research grants from Haemonetics, HeartFlow, Boston Scientific and speaker fees/consultancy from Haemonetics, HeartFlow, Boston Scientific, Abbott Vascular, Volcano-Phillips.
Patient consent Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
Provenance and peer review Not commissioned; externally peer reviewed.