Article Text

Abstract
Objective 30 mm Hg drops in office systolic blood pressure are reported in trials of renal denervation, but ambulatory reductions are much smaller. This disparity is assumed to have a physiological basis and also be present with antihypertensive drugs.
Design We examine this office-ambulatory discrepancy through meta-analysis of drug and denervation trials, categorising by trial design.
Patients (studies) 31 drug trials enrolling 4121 patients and 23 renal denervation trials enrolling 720 patients met the criteria.
Results In drug trials without randomisation or blinding, pressure reductions are 5.6 mm Hg (95% CI 2.98 to 8.22 mm Hg) larger on office measurements than ambulatory blood pressure monitoring (p<0.0001). By contrast, with randomisation and blinding, office reductions are identical to ambulatory reductions (difference −0.88 mm Hg, 95% CI −3.18 to 1.43, p=0.45). For renal denervation, there are no randomised blinded trial results. In unblinded trials, office pressure drops were 27.6 mm Hg versus pretreatment, and 26.6 mm Hg versus unintervened controls. By contrast, ambulatory pressure drops averaged 15.7 mm Hg across all trials. Among those where the baseline ambulatory pressure was not the deciding factor for enrolment (avoiding regression to the mean), ambulatory drops averaged only 11.9 mm Hg.
Conclusions Discrepancies in drug trials between office and ambulatory blood pressure reductions disappear once double-blinded placebo control is implemented. Renal denervation trials may also undergo similar evolution. We predict that as denervation trial designs gradually improve in bias-resistance, office and ambulatory pressure drops will converge. We predict that it is the office drops that will move to match the ambulatory drops, that is, not 30, but nearer 13.
Statistics from Altmetric.com
Introduction
Renal sympathetic denervation is a recently introduced therapy that has been reported to deliver large reductions in blood pressure in patients with resistant hypertension. This holds promise for reducing morbidity and mortality of cardiovascular disease which globally is now the dominant cause of death.1
However, the degree of blood pressure reduction has a wide range of reported values. It is conceivable that this is due to differences in the technical method of achieving renal denervation. Alternatively, it could be related to how the study is conducted and how measurements are collected.
Office blood pressure measurements are widely used in daily clinical practice, but have relatively poor test–retest reproducibility2 as well as challenges, such as digit preference3 and the temptation to remeasure any values that appear clinically inconsistent.4 Ambulatory blood pressure measurement, by capturing and averaging many values over 24 h, offers better test–retest reproducibility.5
The same denervation studies seem to find ambulatory pressure reductions to be much smaller than the office reductions in the same patients.6–8 It has been claimed that office and ambulatory pressure reductions similarly differ in antihypertensive drug trials.9 ,10 If correct, this would be curious since ambulatory pressures are merely an average of repeated single measurements.
We formed the Calibration of Office against circadiaN Values: Expectations for Renal denervation-Generated Effect (CONVERGE) working group to explore the disparity between office and ambulatory reductions in order to gauge what blood pressure drop should be genuinely attributed to denervation.
First, we investigated the hypothesis that ambulatory pressure drops are systematically much smaller than office pressure drops, by meta-analysis of the therapeutic effect of hypertensive drugs on these two markers. Because of potential susceptibility of easily repeated pressure measurements to selection bias,11 we identified studies with two levels of trial design12: (1) uncontrolled, single-armed studies and (2) double-blinded placebo-controlled trials.
Second, we evaluated the blood pressure drop seen from renal denervation in the context of the type of blood pressure measurement (office or ambulatory), and the choice of comparator for the postdenervation measurements (patients with a procedural failure, predenervation measurements, unblinded controls and blinded controls).
Methods
Data sources and search strategy
Antihypertensive drug trials including baseline and final values for both office and ambulatory pressure were identified through a search of the MEDLINE and EMBASE databases (2000–2012).
Randomised controlled trials, case series, case-control studies and conference abstracts of renal denervation in resistant hypertension were identified through a search of the MEDLINE and EMBASE databases. In addition, the Hypertension Device Sector of cvPipeline13 was consulted from which first-in-man data from four renal denervation catheters were accessed. Conference presentations of these devices have since been made publicly available.6 ,14–16
For both searches the strategies are covered in full in online supplementary appendix 1. Search terms were agreed upon by two authors (JPH and ANN) who went on to perform independent review of the articles chosen for further analysis.
Data processing
From each study report, the baseline and final values of office and ambulatory systolic blood pressures were extracted. To be categorised as double-blind placebo-controlled randomisation required adequate concealment of future allocation, that is, a randomisation process more bias-resistant than the discredited17 ,18 sealed-envelope method. Papers presenting secondary analyses of patients from previous trials were excluded.
Statistical analysis was performed using Microsoft Excel 2010 and The Cochrane Collaboration's Review Manager V.5.2.
Antihypertensive drug trials
Antihypertensive drug trials were classed as either one-armed trials or double-blinded randomised placebo-controlled trials. Differences in baseline pressures were calculated using an unpaired two-tailed Student t test.
The disparity between office and ambulatory pressure drops for each class of study were calculated with their 95% CIs using an inverse variance-weighted meta-analysis with a random effects model. For trials which listed only SDs for baseline and final pressures, rather than that of the actual pressure drop, an imputed SD was taken from those that did.
Renal denervation trials
Renal denervation trials were classed as either uncontrolled, unblinded controlled, or blinded controlled. For procedural studies, it is also, in principle, possible to compare patients who underwent therapy against those who did not, either because of technical difficulties or because the patient refused.19 Where studies provided this information we calculated the consequent value.
For each class of study, a weighted mean of systolic blood pressure drop was calculated. Weighting was by sample size.
Results
Antihypertensive drug studies reporting both office and ambulatory pressure drops
Study characteristics
Seventeen one-armed studies, enrolling a total of 2779 patients met the criteria; 14 double-blinded randomised placebo-controlled trials, enrolling a total of 1342 patients met the criteria. The baseline office and ambulatory blood pressures were similar between one-armed trials (161 and 147 mm Hg, respectively) and double-blinded placebo-controlled trials (159 and 148 mm Hg, respectively) with p=0.49 and 0.76, respectively (table 1). Full baseline blood pressure data and study characteristics are shown in online supplementary appendix 2.
Antihypertensive drug trials reporting office and ambulatory pressure reductions, categorised as either one-armed or double-blinded randomised placebo controlled trials
Office and ambulatory pressure drops in one-armed drug trials
In non-randomised, unblinded drug trials, office pressure drops are 5.60 mm Hg (95% CI 2.98 to 8.22) larger than ambulatory pressure drops (p<0.0001, figure 1A).
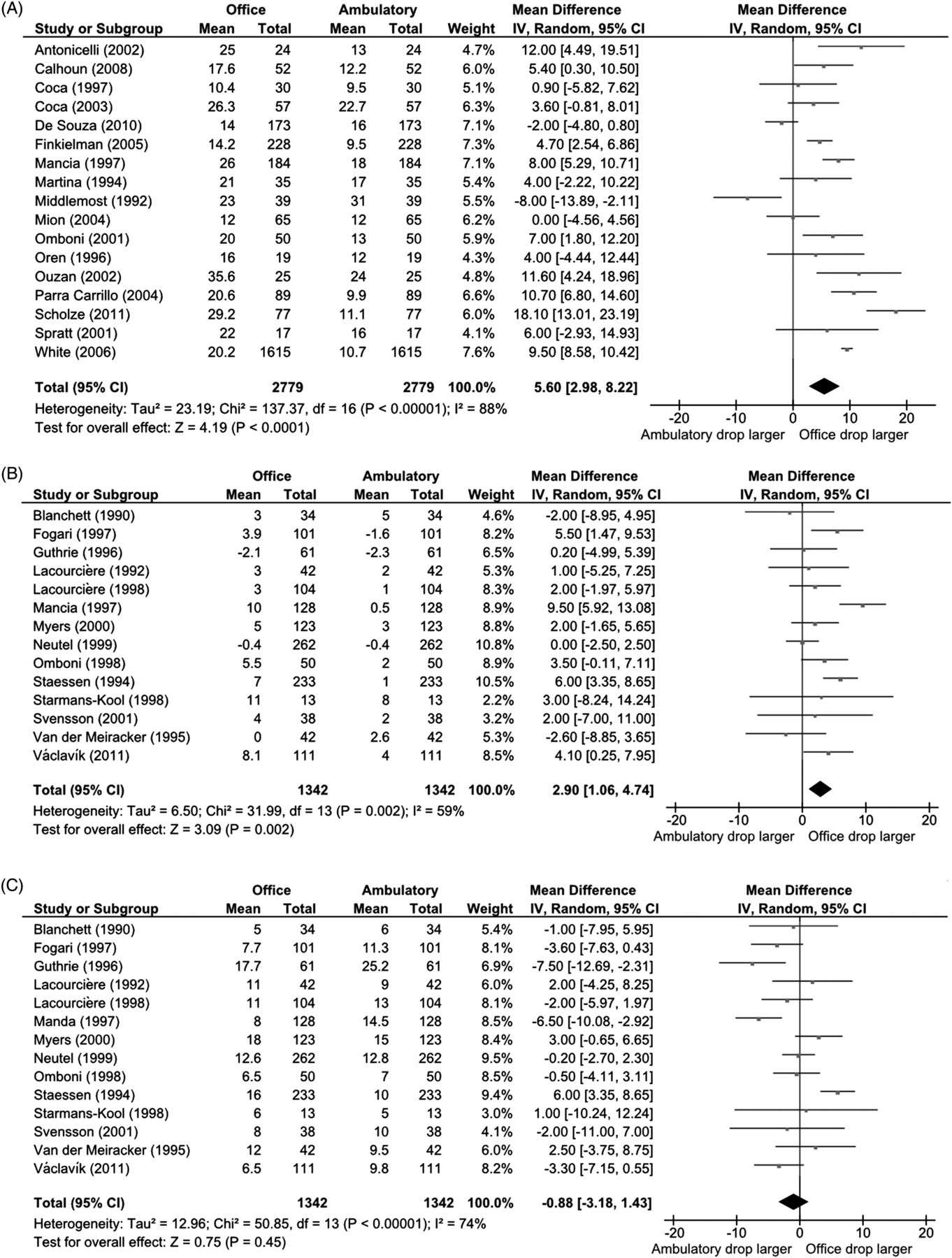
(A) Forest plot of office versus ambulatory pressure reductions in open-label drug trials. Office pressure reductions were 5.60 mm Hg higher than ambulatory pressure reductions (p<0.0001). (B) Forest plot of office versus ambulatory pressure reductions in placebo-treated patients in randomised blinded placebo-controlled drug trials. Office pressure reductions were 2.90 mm Hg higher than ambulatory pressure reductions (p=0.002). (C) Forest plot of office versus ambulatory pressure reductions in active drug-treated patients in randomised blinded placebo-controlled drug trials. The incremental effect of the active drugs was identical on office and ambulatory pressure monitoring (office drops numerically 0.88 mm Hg smaller, p=0.45).
Office and ambulatory pressure drops in randomised placebo-controlled drug trials
In the placebo arms, the pressure drops documented by staff in the office were 2.90 mm Hg larger than those documented on automatic ambulatory pressure monitoring (95% CI 1.06 to 4.74, p=0.002, figure 1B).
Beyond this, the incremental effect of the active drugs (ie, the drop genuinely attributable to the drug) was identical between office and ambulatory pressure drops (office drops numerically 0.88 mm Hg smaller; 95% CI −3.18 to 1.43, p=0.45, figure 1C).
Renal sympathetic denervation trials in drug-resistant hypertension
Study characteristics
Twenty-three studies of renal denervation enrolling a total of 720 patients with resistant hypertension were identified reporting drops in either office pressures or ambulatory pressures or both. Two studies were randomised controlled trials, three were case-control studies, and the remainder were one-armed case series. Study characteristics including format, average age and sex of study participants are available in online supplementary appendix 3.
Ten studies were industry funded and nine did not declare their source of funding. The average age of patients varied across studies between 50 and 69 years. One study used an ultrasound-based renal denervation system.15 The remaining studies used radiofrequency ablation catheters. Eleven measured only office blood pressures. Five measured only ambulatory blood pressures. Seven measured both office and ambulatory blood pressures. While all studies were said to have excluded patients with secondary hypertension, the number that stated how this was done was zero.
Effect of trial design on relative size of office and ambulatory pressure drops in denervation trials
The studies and the sizes of the reported drops are shown in table 2. These results were plotted to visualise the impact of the choice of the comparator group, and choice of the variable measured (office or ambulatory pressures) on the size of the pressure drop calculated (figure 2). Where ambulatory drop was reported for only a subset of a main study, we have listed the ambulatory values separately, to recognise that the patients were not exactly the same as the overall cohort.
The format of renal denervation trials and their outcomes

A plot showing the relationship between trial design and the reductions in office and ambulatory blood pressures. Each data point represents a trial. In unblinded trials, office pressure drops were 27.6 mm Hg versus pretreatment, and 26.6 mm Hg versus unintervened controls. Ambulatory pressure drops averaged 15.7 mm Hg across all trials. Dotted circles representing trials represent those with atypical blood pressure measurement strategies and are discussed in the paper.
Office pressure drops
The first category, ‘denervation versus failure’, consisted of one study, Symplicity-HTN 1, which reported office pressure changes separately for patients who successfully underwent the procedure, and those in whom it could not be completed, most often for anatomical reasons. Mean weighted office pressure drop with denervation was 53.0 mm Hg in the ‘denervation versus failure’ category.
The secondary category, ‘denervation versus preprocedure’ showed a mean weighted office pressure drop of 27.6 mm Hg.
The third category, ‘denervation versus open control’ showed a mean weighted office pressure drop of 26.6 mm Hg.
The fourth category, ‘denervation versus blinded control’ is currently empty, as only now are such trials underway.
Ambulatory pressure drops
Mean weighted ambulatory pressure drop was 15.7 mm Hg over all the study categories.
There were five trials which had two characteristics setting them apart from general clinical practice:
-
office blood pressures were not measured (or at least not reported)
-
enrolment into the trial appeared to have been based solely on the ambulatory pressure that was then also used as the baseline, exposing them to the ‘regression to the mean’ artefact.
These five trials are marked with dotted circles in figure 2. Their weighted mean ambulatory blood pressure reductions had mean size of 19.3 mm Hg. One of them showed the raw blood pressure values for the patients. All 20 pressure values were multiples of 5 mm Hg.20 The probability of this occurring in values arising from algebraic averaging, or indeed from any form of machine measurement of blood pressure, is (1/5)20, that is, p=0.00000000000001.
If those five studies are set aside, the remaining seven studies, all of which reported both office and ambulatory pressures, showed a mean ambulatory pressure reduction of 11.9 mm Hg.
Discussion
Office pressure drops are larger than ambulatory drops in drug trials, but only when the trial is non-randomised and not blinded. In randomised, blinded drug trials, the incremental office blood pressure drop beyond placebo seems to be no bigger than the corresponding ambulatory pressure drop.
No randomised blinded denervation study has yet been completed and reported. Our analysis suggests that when this eventually occurs,21 the office and ambulatory blood pressure reductions may converge. It suggests that the incremental office drop beyond placebo (ie, the drop genuinely due to the intervention) under such bias-resistant conditions may decrease to values seen on ambulatory blood pressure monitoring, that is, ∼10–15 mm Hg.
The office-to-ambulatory ratio of pressure drop in drug trials depends on trial design
This study finds that the large apparent conflict between office blood pressure drops and ambulatory blood pressure drops with renal denervation is an anomaly not seen in well-designed antihypertensive drug trials.
Office pressure drops may be artifactually larger than ambulatory drops in renal denervation trials (and patients treated with placebos in drug trials, as shown in our study) because of either overestimation of baseline office pressures, or underestimation of final office pressures.
Overestimation of baseline blood pressure may occur because of the phenomenon of regression to the mean which applies whenever patients are selected on the basis of exceeding a threshold on any marker that naturally fluctuates with time. In hypertension trials, any patient has a better chance of meeting inclusion criteria on a day when their blood pressure is above their own long-term average. If the patient's blood pressure is then followed up, its average will tend to return to that individual's true mean pressure, even if there was no intervention. This phenomenon is observed frequently in hypertension trials22–24 and is sometimes confused with the placebo effect. The size of the regression to the mean is dependent on the size of the natural variability. Since a 24 h ambulatory average incorporates dozens of raw values, its variation between visits is correspondingly smaller, and regression to the mean is reduced. However, due to day-to-day variations in blood pressure it is not eliminated,2 and could remain a significant source of bias if ambulatory pressures at enrolment are used as the baseline. This could explain why trials only measuring ambulatory blood pressures show a tendency for larger ambulatory blood pressure reductions than trials where ambulatory pressures are measured after enrolment (19.3 mm Hg vs 11.9 mm Hg). This phenomenon can be neutralised in placebo-controlled trials because the office pressure drop in the placebo arm can be subtracted from that in the treatment arm to isolate the true effect.
Underestimation of final office pressures may be explained by observer bias, a phenomenon noted in other studies.25 This might be an understandable natural extension of the common clinical practice of repeating measurements that seem to be erroneously high. In a patient openly having had treatment, if a final office reading unexpectedly appears to have increased from baseline, the physician may choose to remeasure. For a patient openly in the control arm, however, such a value might not be considered erroneous. Higher than average values will be dismissed for the treatment cohort, but recorded for the control. The rejection of only a few values viewed to be biologically implausible can lead to the emergence of a false trend.4 Blinding of treatment groups would minimise this form of bias, and any residual bias would be evident in the placebo arm.
There is an additional possibility that undergoing an invasive procedure may affect a patient's compliance with medication. Some patients do not take the medication prescribed. Selecting a cohort of hypertensive patients in whom many drugs are prescribed but the reduction in pressure is small is an excellent way of enriching a population for such non-adherent individuals. Low adherence to medication has been seen in other studies of resistant hypertension.26 ,27 To go on to perform an invasive procedure on patients with such variable medication compliance could be predicted to seriously influence their future medication habits. This may manifest as decreased compliance due to the belief of having received a ‘curative’ procedure, or increased compliance as a catheter ablation may signify the seriousness of their condition. Such phenomena could significantly confound measurements taken to assess a blood pressure reduction from renal denervation. In a double-blinded trial, the bias would be equal in both arms and would therefore be neutralised.
Curious disappearance of the alerting response in open trials of renal denervation
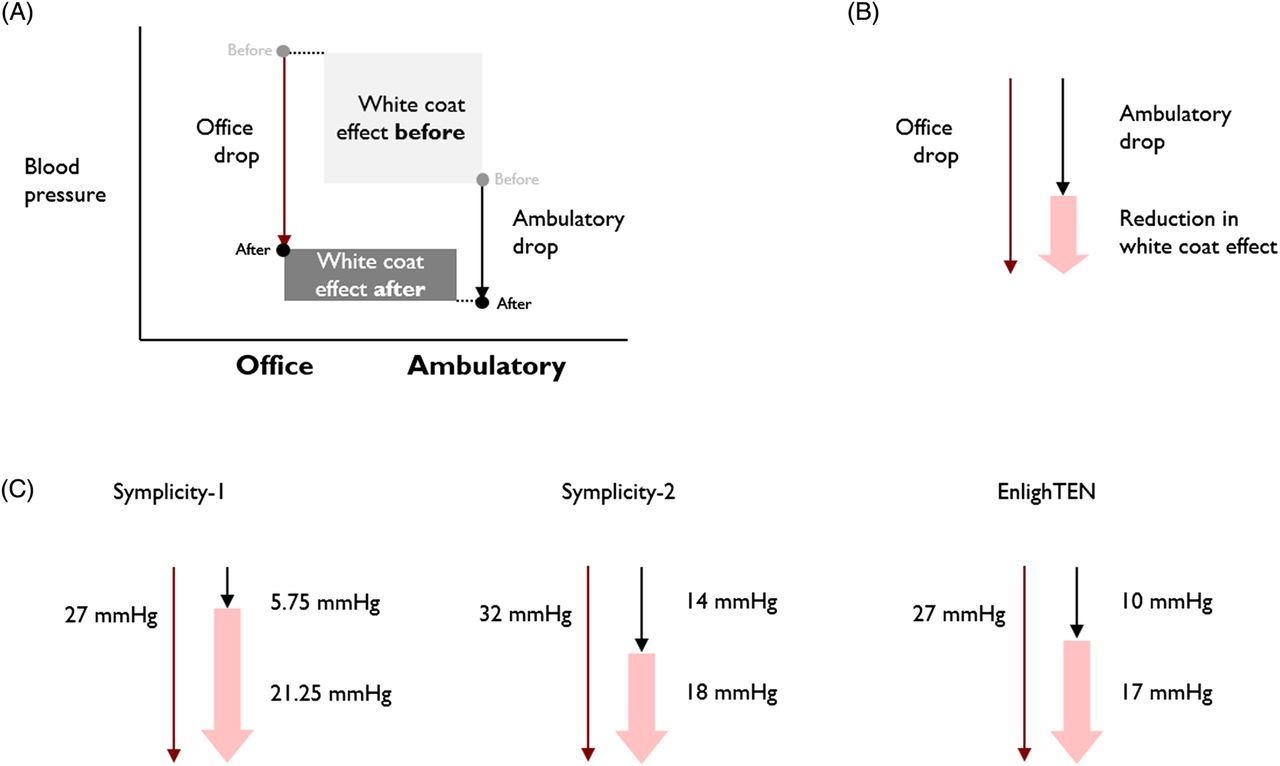
If office and ambulatory pressure reductions from renal denervation truly are significantly different, there must be a specific reduction in the size of the ‘white coat effect’.8 Absolute office pressures are typically higher than ambulatory pressures. The term ‘white coat effect’ can be used to refer to this gap. Our analysis shows office pressure drops to be ∼28 mm Hg depending on trial design, while ambulatory pressure drops are significantly smaller. If office pressures fall further than ambulatory pressures, this white coat effect must shrink, as shown in figure 3.
{kind=link}
{kind=link}
{kind=link}
Because of their interlinking (A), the office drop equals the ambulatory drop plus the reduction in white coat effect (B). There was an average 18.75 mm Hg reduction in white coat effect, implying that it either began above 18.75 mm Hg and was reduced by at least this amount, or finished negative (ie, to say blood pressure dropped during clinic measurement), each of would be highly surprising.
The white coat effect typically averages 10–25 mm Hg.28–31 Results of the three denervation trials reporting ambulatory and office pressure drops indicate that the white coat effect must drop by ∼18 mm Hg from baseline to final (figure 3), implying that the white coat effect almost completely disappears or even reverses. Such a drastic shrinkage or reversal implies that the white coat effect is almost entirely mediated by the renal nerves. This discovery would be profound.
If renal denervation does eliminate the alerting response, one would expect daytime ambulatory pressures to be reduced far in excess of nocturnal blood pressures. A recent analysis of patients from the Symplicity HTN-1 and Symplicity HTN-2 trials, however, shows this is not the case with daytime and nocturnal ambulatory pressure reductions to be similar at 12.2 and 11.1 mm Hg, respectively.32 It is therefore unlikely that the large disparity between office and ambulatory blood pressure drops is caused by disproportionately higher reductions in daytime, and therefore office, blood pressures.
Representativeness
It may at first appear that the major renal denervation trials have focused on patients with unusually severe hypertension who may be very different from patients in drug trials and daily clinical practice. However, the largest ever renal denervation study reporting baseline office and ambulatory blood pressures, EnligHTN-1, showed the baseline ambulatory pressure to be only 150 mm Hg. This is very similar to the 148 mm Hg average ambulatory pressure in the double-blinded randomised drug trials (see online supplementary appendix 2).
The corresponding baseline ambulatory values for Symplicity-HTN 1 and Symplicity-HTN 2 remain undisclosed, surprisingly.
Realistic expectation for pressure drop from denervation
The genuine effect on blood pressure from the act of denervation itself is not directly calculable from routine clinical data. It requires a randomised blinded trial, and ideally one that separates the denervation step from all the accoutrements of the procedure and corresponding bias in the patients’ compliance and observers’ measurements. Patients would need to have a reproducible and bias-resistant baseline assessment of blood pressure, for which ambulatory measurements are well suited.33 They would be randomly allocated to attempted denervation or no attempt at denervation, but would otherwise undergo the same invasive steps, with their status concealed from them by appropriate sedative or amnesic agents. The physicians caring for their blood pressure should likewise be unaware of the allocation arm, and the final measurement should be in a reproducible and bias-resistant modality such as ambulatory pressure. Such trials are now underway.21
Until these trials report, the most bias-resistant and, therefore, accurate measurements of the true blood pressure reduction from renal denervation are those from trials measuring ambulatory pressure drops.
Study limitations
This meta-analysis uses data from multiple hypertension and renal denervation trials. The renal denervation trials appear to be particularly heterogeneous, with a variety of trial designs, inclusion criteria and blood pressure measurement strategies. The methods through which secondary hypertension were excluded were not covered in any of the articles.
In many of these denervation trials, there were changes in medication during follow-up, so that the net effect on blood pressure cannot be assumed to be caused by denervation alone. However, this should not have caused the divergence between office and ambulatory blood pressure drops that we have observed.
Only two randomised controlled trials of denervation have so far been reported. The majority of denervation trials included in this analysis were case-control studies or case series (table 2).
We included all eligible studies, even though there were unclear aspects in some, such as the existence of a five-study subset that described the clinically unusual habit of carrying out only ambulatory pressure measurements with no office pressure measurements at all. The ambulatory pressure drops in them seemed similar to office pressure drops from other denervation studies. Moreover, where raw data were published, the final-digit characteristics suggested (p=0.00000000000001) accidental mislabelling of manually documented office pressures as 24 h ambulatory monitoring. This could easily happen in a fast moving field, such as denervation.
However, since we cannot tell if all five (or indeed any) had inadvertently mislabelled office measurements as ambulatory, we merely mark them and present separate weighted average responses, with them included and excluded.
Clinical implications
If the genuine pressure drop from renal denervation as established from future bias-resistant (blinded, placebo-controlled) trials turns out to be between 10 and 16 mm Hg, this is still a substantial benefit which could be expected to deliver ∼20% reduction in cardiac events and ∼40% reduction in stroke.34 The ability to extrapolate confidently, that is, from a reliable effect size, is important because adequately powered hard endpoint trial results will not arrive soon.
Conclusion
The large disparity between office and ambulatory pressure drops reported with renal denervation is unique. If it is to be explained as a recognised feature in drug trials, then it should be noted that it only occurs when the drug trials are open to bias by lack of blinding and lack of controls. With blinding and randomisation implemented, to neutralise bias, the effect disappears, that is, office and ambulatory pressures fall equally. Even with only placebo tablets, staff documenting office blood pressures record significantly larger drops than automatic machines recording ambulatory blood pressures (p=0.002).
Renal denervation will soon have blinded trial results. If the effect size beyond placebo is not 30 mm Hg, but only a fraction of this, we should not assume that these more rigorously designed trials are the ones in error. Ambulatory pressure drops, from a baseline measured separately from enrolment values, average 11.9 mm Hg. This analysis makes the formal scientific prediction that excess office pressure drop beyond the control arm drop, in bias-resistant trial designs, will converge towards a similar value.
In our search for device-based therapies for hypertension, we have a responsibility to derive the most reliable information from patients volunteering to undergo permanent physiological modification to advance science. Now that our analysis is published, we recommend future investigators, seeking to quantify the true effect of renal denervation on blood pressure, should avoid further unblinded studies using office measurements. These two ingredients have been a recipe for gross exaggeration.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix 1
- Data supplement 2 - Online appendix 2
- Data supplement 3 - Online appendix 3
Footnotes
-
Contributors JPH: designed the study; retrieved and processed the data; designed the images; drafted and revised the manuscript; ANN: codesigned the study; retrieved and processed the data; designed the images; drafted and revised the manuscript; DPF: initiated the study; codesigned the study; designed the images; drafted and revised the manuscript. Guarantor: DPF.
-
Funding DPF is funded by a British Heart Foundation Senior Research Fellowship FS/10/038.
-
Competing interests DPF is a consultant to Medtronic Inc, which manufactures devices for renal denervation. This analysis is a permissible independent academic activity not instigated, supported, censored or condoned by industry. Data used are in the public domain. We have no knowledge of the data of the Symplicity-HTN-3 trial and no involvement in its design. We have reported an unblinded, uncontrolled pilot study of renal denervation in heart failure,35 and are now conducting a blinded randomised controlled trial.36
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement All data analysed within this study are available from the corresponding papers. All data used is visible within this paper and the online supplementary appendices 1–3.